

Abstract
Background:
Training and continuous dynamic communication between patients and health professionals in chronic diseases like diabetes, is important. The aim of this study is to evaluate the effects of diabetes self-care group education and nurse- telephone follow-up on glycemic control and compliance with treatment orders in patients with type 2 diabetes attending to diabetes clinic in khomein.
Methods:
In this clinical trial, 62 patients with type 2 diabetes who attending to the diabetes clinic selected and were randomly assigned to experiment and control groups. Self-care group education was applied for case group (n = 31) and they were followed up using telephone calls for 12 weeks by a nurse. The control group (n = 31) received the conventional management. Demographic characteristics, compliance with treatment recommendations (diet, drug use, exercise) and blood glucose control indices were recorded before and after interventions. Data were analyzed by SPSS software version 16 using independent t-test, paired t-test, Chi-square test, non-parametric tests, mixed model (ANOVA + repeated measure) and ANCOVA.
Results:
The mean age of intervention and control groups was 50.9 ± 7.3 and 55.1 ± 10.1 years, respectively. Blood glucose indices (FBS, 2 hpp BS, Hb A1C) were improved in both case and control group after intervention but it was only statistically significant in case group P > 0.0001. During study, percentage of patients with very good compliance in control group decrease from 12.5% to zero (0%), whereas in experiment group these amounts increase from 6.5% to 90.3% P > 0.0001.
Conclusions:
According to the results of the current study self-care group education and 12 weeks follow-up by a nurse using telephone causes significant improvement in metabolic parameters and adherence to treatment recommendations in diabetic patients.
Keywords: Adherence, diabetes control, group education, nurse-telephone follow-up
INTRODUCTION
Diabetes is the most common chronic metabolic disorder that is full of progressive and debilitating complications, involve 6-15% of the population.[1] and it is the main cause of blindness, end-stage renal disease, dialysis and amputation.[2] Type 2 diabetes include 90-95% of all cases of diabetes that occurs in adulthood and influenced by lifestyle.[3] Studies have shown that adequate control of blood glucose in diabetic patients is very important and could prevent or delay different complications of disease so that it is estimated with every 1% reduction in glycosilated hemoglobin (HbA1C) 37% of microvascular and 21% of macrovascular complications will be reduced.[4]
Chronic course of diabetes disease together with its influences on all aspects of patient life and high expenditure for health services justify conducting multiple studies with aim of finding effective ways for disease control. Recent studies show in spite of educational programs, misunderstanding of disease and its control are common among diabetic patients.[5] Research had been shown that adherence to treatment recommendations has the most effect on diabetic patients’ metabolic control, therefore support of diabetic patients which have many self-care problems in addition to educational programs, implementation of an appropriate follow-up plan for strengthening knowledge, improve attitude and behavior toward adherence enhancement to treatment recommendations will be necessary.[6] Some research studies, which used different telemedicine strategies, represent positive effects on blood glucose control and such interventions cause reduction or prevention of chronic diabetes complications.[7]
Because telephone has a widespread utilization among people, telephone centered programs in particular, would be a successful method for transporting management care services of diabetic patients to their homes through which blood glucose control could be improved. In fact utilization of telephone follow-up for delivery of cares not only decrease expenses and facilitate accessibility to effective services, but also cause promotion of patient-provider relationships and elimination of time or place problems related to patient education.[8]
There has been studies, to examine the effect of education and patient follow-up in various way. Kim and Oh have shown in their study that patient education and telephone follow-up lead to significant effect upon metabolic control.[9]
But in other study, the effect of these interventions was not so clear, for example in Wong's study the A1c reduction and diet and drug adherence scores were not significant statistically.[10]
In addition to the fact that increasing adherence to treatment recommendations may be cause to better control of diabetes and its complications, until now there is rare study to engage in diabetic patient adherence to treatment recommendations in Iran. Take into account this truth that education to diabetic patient alone do not guarantee adherence to therapeutic regimen, thus we decide to examine the nurse- telephone follow-up approach for metabolic control improvement and adherence enhancement of diabetic patients to treatment recommendations in a trial. The aim of this study is to examine the effectiveness of group education and nurse-telephone follow-up in controlling blood glucose and increasing adherence to treatment recommendations.
METHODS
This study was a randomized controlled clinical trial, in patients with diabetes type II attend to Khomein's diabetes clinic in 1389 year (2010). This study is subject to permission from the Research Council and Ethics Committee of Nursing and Midwifery School of Tehran University of Medical Sciences.
In this study, group education and nurse-telephone follow-up calls were as independent variables, and fasting blood sugar (FBS), blood glucose 2 h after meals (2 hpp BS), glycosylated hemoglobin (Hb A1C) and the patient's adherence to treatment programs as dependent variables. For data gathering, a two part questionnaire was used derived from Cheri Ann Hernandez study. This questionnaire was made of individual and sociodemographic information section and 13 questions about adherence to treatment recommendations.
Response to questions were classified as likert spectrum consist of always (all of week), often (4-5 days a week), sometimes (at least three days a week), rarely (1-2 days a week) and never (not once a week).
The validity of the questionnaire was determined using content and face validity (10-member expert panel and the ethics committee examination) and its reliability through Cronbach's alpha. Second part of questionnaire was related to adherence score determination. In total this section had 65 points and classification scores of this part were unfavorable (14-27), some favorable (28-40), favorable (41-52), very favorable (53-65) respectively. Information on disease duration and type of treatment and test results (FBS, 2 hpp BS, Hb A1C) was also recorded before and after the interventions.
The study samples were determined by reliability of 99% and with 95% power test, 62 samples entered study according to the probability of loss. The inclusion criteria were completed informed consent to participate in the study, access to telephones, lack of difficulty in speech, hearing and vision and absence of diseases associated with physical and mental illness. Exclusion criteria were hospital admission during study, changing treatment protocol, presenting with DKA (diabetic ketoacidosis) or NKHSS (nonketotic hyperosmolar syndrome), catching an infectious disease and go to journey or departure from city. Thus, 62 patients were randomly selected. The participants in the study were randomly assigned to two groups, experiment (n = 31 patients) and controls (n = 31 patients). In experiment group interventions consist of; two educational session lasting 60 min in two consecutive day about diabetes and its complications, importance and ways of self-care in diabetes, correct insulin injection, self monitoring blood glucose (SMBG) in home, emergent measures in hypoglycemia, regular use of drugs, diet in diabetes and significance of exercise and physical activity for diabetic patients.
Educations were in two route, directly by using a combination of lectures, face to face method, film demonstration and indirect method by booklet presentation to patients. This group of patients followed up 16 times by trained diabetes nurse of clinic through telephone (in first 4 weeks, 2 calls per week and for the remaining 8 weeks one calls every one week). Finally, patients were followed up for 3 month. In each call, patients in experimental group were asked about adherence to diet, drugs usage, exercise, self monitoring blood glucose (SMBG) at home, and possible questions raised on behalf of patients, had been responded instantly. During intervention period control group has been received conventional care and usual education for diabetic patients.
Collected data were analyzed by SPSS software version 16 using independent t-test, paired t-test, Chi-square test, non- parametric tests, mixed model (ANOVA + repeated measure) and ANCOVA.
RESULTS
Mean age at experiment and control groups were 50.9 ± 7.3 and 55.1 ± 10.1 years, respectively. In experiment group, 57.1% and in the control group 42.9% were men. At the start of study, participants in both group were identical on all characteristics except job status, duration of diabetes affliction and fasting blood sugar [Tables 1 and 2]. The amount of Hb A1c, FBS, 2 hpp BS before and after interventions in both groups are shown in [Table 3].
Table 1.
Sociodemographic characteristics of patients in the study before interventions

Table 2.
Patients’ characteristics in experiment and control groups before interventions
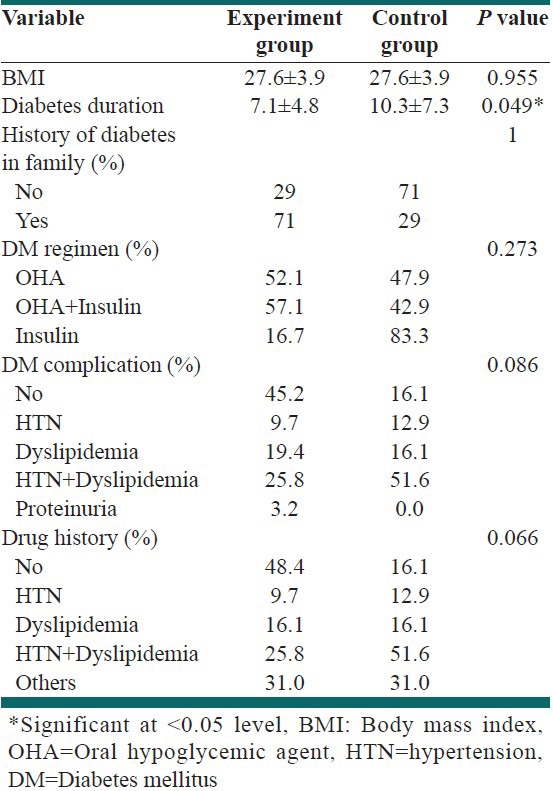
Table 3.
Comparison of blood glucose indices before and after interventions in experiment and control groups
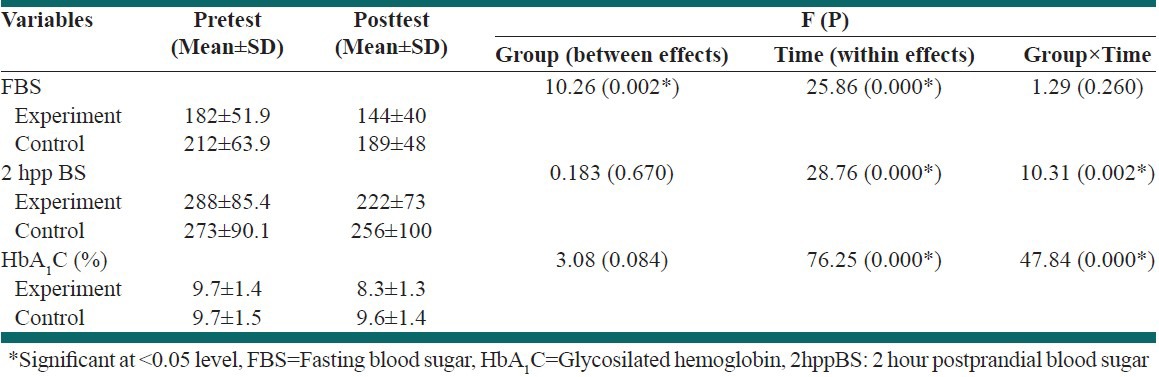
At the end of study, FBS reduced in both control and experiment group that was significant statistically (P < 0.008) but in control group, 2 hppBS and glycosylated hemoglobin levels (Hb A1c) had no significant change (P < 0.185, P < 0.198). whereas in experimental group these measures were substantially decreased so that show 66 mg/dl and 1.4% decline for 2 hpp BS and Hb A1c, respectively (P < 0.0001).
There are no cases in unfavorable group according to adherence score classification (14-27).
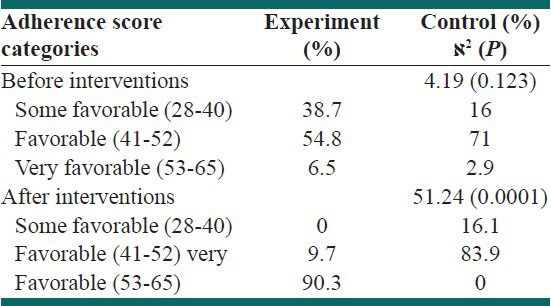
Chi-square test showed significant difference in adherence score categories before and after interventions in experiment group (P < 0.0001), but no significant change in control group (P < 0.123). In experimental group, before interventions 6.5% of patients were in most favorable adherence category (score 53-65) but at the end of study it was growing to 90.3%, this is very interesting and confirm that these type of interventions are very effective [Table 4].
Table 4.
Comparison of adherence to treatment score categorization before and after interventions in experiment and control groups
For advanced analysis, General linear Model (GLM) and Mixed Model (repeated measure + ANOVA) were used. The result of these analyses had been shown in [Table 3]. It is necessary to mention that overall there was an interaction effect for Group and Time variables (P < 0.0001), but univariate table showed in fact only for 2 hppBS and Hb A1c it is meaningful. It mean that in two measurements (before and after intervention) in control group amount of 2 hppBS and Hb A1c had no significant changes but for experiment group it was decreased significantly.
For controlling confounder variables, ANCOVA (Analysis of Covariance) were used. Age, BMI, diabetes duration, FBS1, 2 hppBS1 and HbA1C1 variables had been entered to model as covariates. ANCOVA were known FBS1, 2 hppBS1 and HbA1C1 as significant confounders. After adjusting for effects of confounders, comparison of adjusted means in two groups, again remained significant for FBS2, 2 hppBS2, HbA1C2 (P < 0.008, P < 0.006, P < 0.0001) respectively.
DISCUSSION
The aim of this study was to determine the effects of group education together with telephone follow-up on the blood sugar levels and adherence to treatment plan in type 2 diabetic patients. In the present study, educational interventions and 12 weeks telephone follow-up cause 1.4% reduction on glycosylated hemoglobin level (Hb A1c) in experiment group, also during study percentage of patients with very good compliance in control group decrease from 12.5% to zero (0%), whereas in experiment group these amounts increase from 6.5% to 90.3%, these findings indicates the impact of appropriate interventions, which applied and will be definitely result in preventive effects in the long term. Based on the results of this study, group education and 12 weeks telephone follow-up by a nurse trained in diabetes, improves metabolic control and adherence to treatment recommendations in diabetic patients.
In some studies, such as Rakhshandehroo and colleagues integrated training programs, will improve significantly knowledge, attitude and performance in diabetic patients and may improve their metabolic control.[11]
In Kim and his colleagues study, telephone intervention for three months in experiment group reduced glycosylated hemoglobin level about 1.2% and increase adherence to diet regimen significantly in diabetic patients, these results are consistent with present study.[9] Sung and Kim study in south Korea showed combination of educational intervention with telephone counseling and follow-up lead to blood glucose control and improvement of self- management or self- care of diabetic patients.[12] These findings confirm results of our study.
According to Nesari and colleagues research in Iran in 1386 (2007) year, with aim of examining the effect of tele-nursing on diabetic patients adherence to diet regimen, after diet counseling and self- care educations with 12 week calls follow-up, results showed reduction of Hb A1c level and increase of adherence to diet significantly in intervention group.[13]
These findings match with our study, although in present study we identify complete adherence effects to treatment plan including diet, exercise and drug use components. Nevertheless there are some evidence that show adverse results, for example in pietti study after self-care education to diabetic patients through telephone calls and follow-up every 2 week for 12 month, in experiment group a better adherence to treatment were observed but there is no significant change for Hb A1c compare to before intervention.[14] Also in the study of Wong and colleagues with aim of examining nurse- telephone follow up effects on diabetic patients, results showed no statistically significant reduction in level of Hb A1c and only significant improvement in exercise adherence score but not for diet or drug adherence scores.[10] According to two recent study results, nurse- telephone follow-up could not show acceptable change on blood sugar level and have controversial effects on adherence scores in diabetic patients.
CONCLUSIONS
The significance of this study is that can show implementation of group education and nurse-telephone follow-up for 3 month would result in improvement of blood sugar control and adherence to treatment recommendations (diet, exercise, drugs) in diabetic patients.
Some limitations of the current study are the relatively small sample size and single blindness (only patients) of trial and to some extent short period for patients follow-up.
Suggestions
Given the chronic nature of diabetes that requires constant attention of the patient and his relatives and medical staff, for strengthening of educations and improving patients care and adherence to treatment plan we offer utilization of nurse-telephone follow up. Studies of cost – effectiveness or feasibility and research in large samples size also recommend.
Footnotes
Source of Support: This study approved and was financially supported by Research Vice chancellor of Tehran University of Medical Sciences through research design number 457
Conflict of Interest: None declared.
REFERENCES
- 1.National Kidney Foundation. KDOQI clinical practice guideline for diabetes and CKD: 2012 update. Am J Kidney Dis. 2012;60:850–86. doi: 10.1053/j.ajkd.2012.07.005. [DOI] [PubMed] [Google Scholar]
- 2.Martinez-Castelao A, Gorriz JL, Garcia-Lopez F, Lopez-Revuelta K, De Alvaro F, Cruzado JM. Perceived health related QOL and co morbidity in diabetic patients starting dialysis (CALVIDIA study) J Nephrol. 2004;17:544–51. [PubMed] [Google Scholar]
- 3.Trasoff D, Delizo J, Du B, Purnajo C, Morales J. Diabetes in the middle East. Epinex Diagnostic, Inc. Corporate Information Series 4. [Last accessed on 2008]. Available from: http//www.epinex.com/pdf/Epinex .
- 4.Dalewitz J, Khan N, Hershey CO. Barrier to control of blood glucose in diabetes mellitus. Am J Med Qual. 2000;15:16–25. doi: 10.1177/106286060001500104. [DOI] [PubMed] [Google Scholar]
- 5.Rubin RR, Peyrot M. Quality of life and diabetes. Diabetes Metab Res Rev. 1999;15:205–18. doi: 10.1002/(sici)1520-7560(199905/06)15:3<205::aid-dmrr29>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- 6.Saito I, Fujiko I, Ikebe T, Moriwaki C, Tsubakimoto A, Yonemasu K, et al. Impact of diabetes on health-related quality of life in a population study in Japan. Diabetes Res Clin Pract. 2006;73:51–7. doi: 10.1016/j.diabres.2005.11.015. [DOI] [PubMed] [Google Scholar]
- 7.Sigurdardóttir AK, Jonsdóttir H. Empowerment in diabetes care: Towards measuring empowerment. Scand J Caring Sci. 2008;22:284–91. doi: 10.1111/j.1471-6712.2007.00506.x. [DOI] [PubMed] [Google Scholar]
- 8.Funnell MM, Tang Ts, Anderson R. From DSME to DSMS: Developing empowerment-based diabetes self-management support. Diabetes Spectr. 2007;20:221–6. [Google Scholar]
- 9.Kim HS, Oh JA. Adherence to diabetes control recommendation: Impact of nurse telephone calls. J Adv Nurs. 2003;44:256–61. doi: 10.1046/j.1365-2648.2003.02800.x. [DOI] [PubMed] [Google Scholar]
- 10.Wong FK, Mok MP, Chan T, Tsang MW. Nurse follow up of patients with diabetes: Randomized controlled trial. J Adv Nurs. 2004;50:391–402. doi: 10.1111/j.1365-2648.2005.03404.x. [DOI] [PubMed] [Google Scholar]
- 11.Rakhshandero S, Ghafari M, Heidarnia AR, Rajab A. Effectiveness of educational intervention on metabolic control in diabetic patients attending Iranian Diabetes association. Iran J Diab Lipid Disorder. 2008;2:57–64. [Google Scholar]
- 12.Song MS, Kim HS. Intensive management program to improve glycosylated hemoglobin levels and adherence to patients with type 2 diabetes. Appl Nurs Res. 2009;22:42–7. doi: 10.1016/j.apnr.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 13.Nesari M, Zakerimoghadam M, Rajab A, Rajabzadeh S, Basampour SH, Rahmani M. Study of nurse-telephone follow up effect on blood and lipids control of type 2 diabetic patients. Iran J Diab Lipid Disorder. 2008;8:115–22. [Google Scholar]
- 14.Piette JD, Weinberger M, McPhee SJ, Mah CA, Kraemer FB, Crapo LM. Do automated calls with nurse follow-up improve self-care and glycemic control among vulnerable patient with diabetes. AM J Med. 2000;108:20–7. doi: 10.1016/s0002-9343(99)00298-3. [DOI] [PubMed] [Google Scholar]