

Abstract
Background:
Postoperative shivering is very common and followed by many problems such as increasing oxygen consumption, blood pressure, intracranial and intraocular pressure, and postoperative pain. Therefore, prevention of shivering is important, especially in elderly and ischemic heart disease patients. The goal of this study was to compare the effect of pethidine (meperidine), dexamethasone, and placebo on prevention of shivering.
Methods:
This double-blind clinical trial study was carried out on 120 patients who were candidates for surgery under general anesthesia. The patients were randomly divided into three groups. Induction and maintenance of anesthesia for all patients were similar. Temperature of patients was measured every 5 min interval. After induction, saline 0.9%, dexamethasone and pethidine were injected to groups a, b, and c, respectively. In recovery, patients were controlled for visible shivering. All data were statistically analyzed by analysis of variance (ANOVA) and Chi-square tests.
Results:
There were no significant differences among three mentioned groups regarding gender, age, duration of surgery and anesthesia, extubation time, duration of recovery, and basic clinical characteristics. Nineteen cases (47.5%) of placebo group had postoperative shivering, whereas in dexamethasone group only four cases (10%) had shivering and the difference between the two groups was significant. Also in pethidine group, 15 cases (37.5%) had shivering and the difference with placebo group was significant (P value = 0.001).
Conclusion:
The present study showed that pethidine and dexamethasone are effective drugs for prevention of postoperative shivering in elective surgery and the effect of dexamethasone in preventing the postoperative shivering is better than pethidine.
Keywords: Dexamethasone, general anesthesia, shivering, surgery, pethidine
INTRODUCTION
Human body core temperature is one of the most important and stable parameters to maintain physiology of the body, and any disorder in it including the hypothermia during surgery leads to problems such as shivering after surgery, coagulation disorders, disorders of body nitrogen balance, and changes in drug effects on the body.[1]
In the previous studies, mild hypothermia has also increased the risk of shivering three times after heart surgery, then even avoidance from mild hypothermia should be considered important.[2]
Postoperative shivering is the most common complications after surgeries, which is seen among 6.3-65% of patients and include involuntary movements of one or more groups of muscles.[3]
Shivering can cause many side effects such as increased oxygen consumption, carbon dioxide production, heart rate, and blood pressure, resulting in exacerbation of ischemic heart disease, as well as increased intracranial pressure, intraocular pressure, pain at the surgical site, and also a sense of discomfort to the patient.
General anesthesia facilitates redistribution of the temperature from the central tissues to the peripheral tissues. Due to anesthesia, core temperature regulation responses like the vasoconstriction threshold are controlled, and most anesthetic drugs cause peripheral vasodilatation.[4]
Shivering could be the result of hypothermia during surgery, readjustment of body core temperature, or because of fever and shivering, which could lead to activation of the inflammatory response and cytokine release.[5] There are two methods to reduce the shivering, including medical and nonmedical methods. Nonmedical method involves the use of moisturizers, preventing hypothermia using warm blankets, and warm and moist oxygen inhalation. The medical method shows its influence with reducing the shivering temperature threshold.[3]
Drugs such as dexamethasone reduce the gradient between skin and body core temperature. It could reduce shivering by regulating immune responses.[5] Some medications such as meperidine (pethidine) have known effective at all doses.[3] However, there is some debate over the question: “Which treatment method is more suitable for patients after surgery? Therefore, we wanted to compare routine dose of pethidine (25 g) with dexamethasone (0.1 mg/kg) to response to this question. The aim of this project is to compare two drugs of pethidine and dexamethasone in terms of reducing this complication.
METHODS
The present study is a double-blind randomized clinical trial with control group. Patients who were hospitalized in Ardabil Imam Khomeini Hospital, for surgery (general, orthopedic, and ENT surgeries) with general anesthesia were included in the research with their written consent. Of course, they had no prohibition to enter the study.
In terms of physiological class, the patients were in groups of ASA I and II, while none of the patients had taken medication before surgery.
Exclusion criteria were history of drug abuse, neuromuscular disease (because of disturbing of evaluation of shivering grading in these patients), any previous records of sensitivity to these drugs, evidence of grade 3 or 4 heart failure, fever (more than 37.8 oral degrees), and a history of taking alpha-2 blocker drugs. The sample size was calculated based on similar studies and reducing about 30% of shivering rate using both drugs, with an alpha level equal to 5% and the study power equal 80% and using the following formula about 40 samples in each group and the total 120 samples.

In this study, patients, who were hospitalized with general anesthesia in Ardabil Imam Khomeini Hospital due to surgery necessity (general, orthopedic, and ENT surgeries), were enrolled after the agreement with the University Medical Ethics Committee and submitting their written consent and registering in the Clinical Trials System of the Ministry of Health and Medical Education. Before induction of anesthesia, the patients were given 7 ml/kg of a normal saline serum. To maintain the integrity of results, none of the patients received preanesthetic medication. Patients were randomly blocked [block size of 6 is chosen, possible balanced combinations with 2 P (pethidin) and 2 NS (normal saline) and 2 D (dexamethasone) subjects are calculated as 6 and blocks are randomly chosen to determine the assignment of all 120 participants] into three groups of normal saline (10 ml), pethidine (25 mg, the volume of which is brought to 10 ml),[6] and dexamethasone (0.1 mg/kg the volume of which is brought to 10 ml).[7] All three drugs were prepared in the same 10 cc syringes and the anesthesiologist responsible for the control and registration of the clinical symptoms was blinded to the study drugs.
Induction of anesthesia started with the same way in three groups by injecting fentanyl 1 μg/kg, sodium thiopental 5 mg/kg, and atracurium 0.5 mg/kg. After intubation, anesthesia was kept on with 100 μg/kg/m propofol infusion, along with the inspiratory gas mixture (50% oxygen and 50% N2O). To maintain muscle relaxation during surgery, 0.5 mg/kg atracurium was injected and the patients were mechanically ventilated during surgery.
Each drug was administered after induction of anesthesia. For all patients, the core temperature was measured and recorded through tympanic and the skin temperature through forehead skin by digital thermometer every 5 min interval in operating room and recovery and values at baseline, after induction of anesthesia, end of surgery, in arrival to recovery, and exit from recovery room were used for analysis.
In addition, the systolic and diastolic blood pressure and the patients’ heart rate were recorded, and the mentioned cases were remeasured and recorded immediately after induction of anesthesia at the end of surgery after the patient entrance into and before his/her exit from recovery room.
Operation room temperature was recorded by a wall thermometer and maintained during the surgery between 20 and 22°C and intravenous fluids were kept in this temperature.
The trachea was extubated when the patient became fully awake. Anesthetic time was defined from the start of induction to the time when the anesthetic, including nitrous oxide, was discontinued. The subsequent period until the patient responded to verbal command was recorded as the recovery time.
If the systolic blood pressure were dropped to 20% less than baseline values, ringer-lactate serum and if necessary 10 mg of ephedrine was administered.
In whole the recovery phase, the patients were monitored by a trained anesthesia nurse responsible for the recovery and he recorded shivering as soon as it happens. This nurse, who was not informed about the kind of prescribed medication, registered shivering occurrence and its severity.
The shivering was graded using a five-point scale [Table. 1].
Table 1.
Classification of shivering
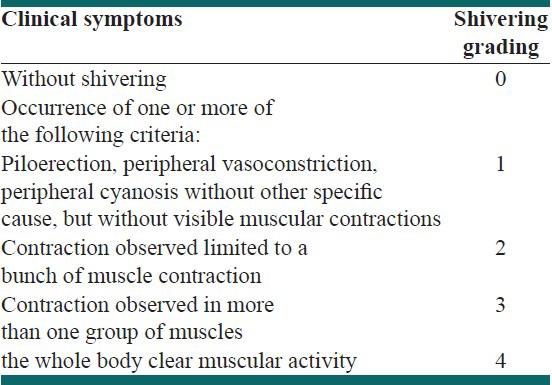
In addition to, nausea or vomiting in patients was also being registered during recovery. We treated the intense shivering (3 and 4 grades) after operation with 25 mg pethidine and postoperative nausea and vomiting with 10 mg metoclopramide. Continuous variables, including demographic data and temperature values over time within groups, were analyzed by using repeated measures analysis of variance. One-way analysis of variance was used to analyze differences among the groups. Incidence of shivering was analyzed by using Chi-square test. Data were expressed as mean ± SD, with P < 0.05 being considered significant.
RESULTS
During the study, no patients were excluded. In terms of age, gender, type of surgery, duration of surgery, duration of anesthesia, extubation time, duration of recovery, and basic clinical characteristics (core temperature, skin temperature, systolic and diastolic blood pressure, and heart rate), there was no significant difference between the patients in three groups (P > 0.05) [Tables 2 and 3].
Table 2.
Comparison of three groups of patients by age, gender, duration of surgery, anesthesia, extubation and recovery, and the surgery type. values have been expressed as mean±SD
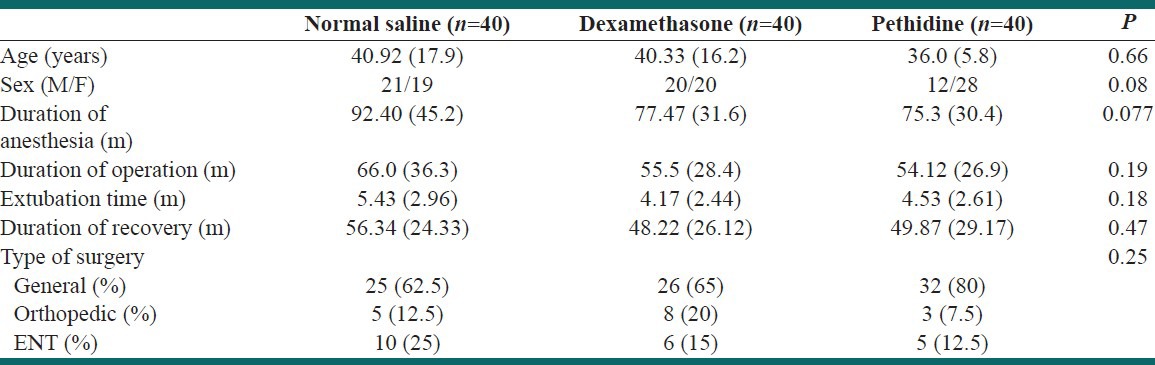
Table 3.
Comparison of three groups patients in terms of basic clinical characteristics. values have been expressed asmean±SD

The trend of core body and skin temperature changes in the patient has been shown in chart numbers 1 and 2. We found that the core body temperature reduction was recorded in all four stages, comparing the basic values was higher in control group than the other two groups (P < 0.05). In dexamethasone group compared to pethidine group, the core body temperature reduction in recovery was lower, but this difference was not significant (P > 0.05) [Figure 1]. Regarding the skin temperature in all three groups, the temperature drop compared to baseline values was observed in all stages. This dropping in control group was more severe than the two other groups (P < 0.05). In dexamethasone group compared to pethidine group, the core temperature drop in recovery was lower, but this difference is not significant (P < 0.05) [Figure 2]. Systolic and diastolic blood pressure of patients has increased in three groups after induction of anesthesia (in average 2.11 mmgh in placebo, 8.05 mmgh in dexamethasone, and 6.65 mmgh in pethidine groups for systolic and 6.88 mmgh in placebo, 8.63 mmgh in dexamethasone, and 6.63 mmgh in pethidine groups for diastolic blood pressure). It has had a declining trend during the surgery process (in average 12.65 mmgh in placebo, 14.62 mmgh in dexamethasone, and 15.3 mmgh in pethidine groups for systolic and 10.6 mmgh in placebo,10.75 mmgh in dexamethasone, and 12.55 mmgh in pethidine groups for diastolic blood pressure) and during recovery, it has shown a relative stability (123.55 ± 16.21 mmgh in placebo, 122.35 ± 15.43 mmgh in dexamethasone, and 122.45 ± 17.48 mmgh in pethidine groups for systolic and 77.01 ± 10.78 mmgh in placebo, 77.75 ± 9.65 mmgh in dexamethasone, and 76.95 ± 10.91 mmgh in pethidine groups for diastolic blood pressure). The patients’ heart rate has slightly increased immediately after induction of anesthesia in all three groups (in average 8.11 b/m in placebo, 5.98 b/m in dexamethasone, and 9.05 b/m in pethidine groups) and then during surgery and recovery process it has been declining (in average 18.3 b/m in placebo, 15.51 b/m in dexamethasone, and 18.05 b/m in pethidine groups). Changes in systolic and diastolic blood pressure values and heart rate during anesthesia and recovery process in the three groups were not significantly different (P > 0.05).
Figure 1.
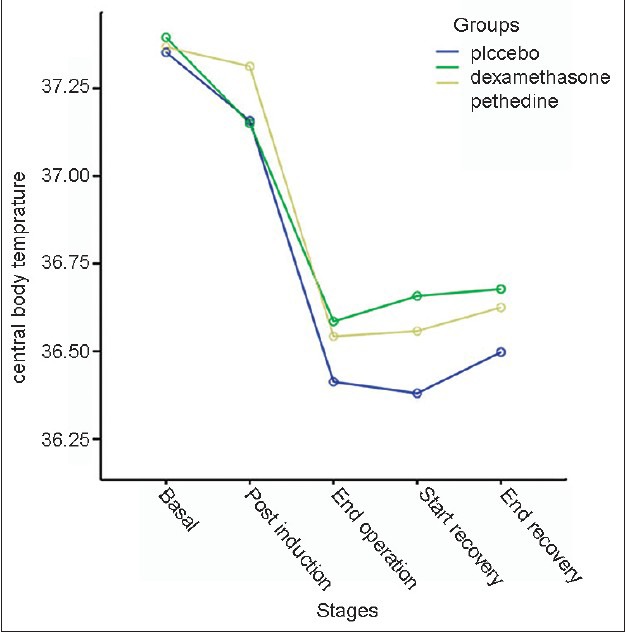
Measured core body temperature in three groups during anesthesia and recovery procedures
Figure 2.
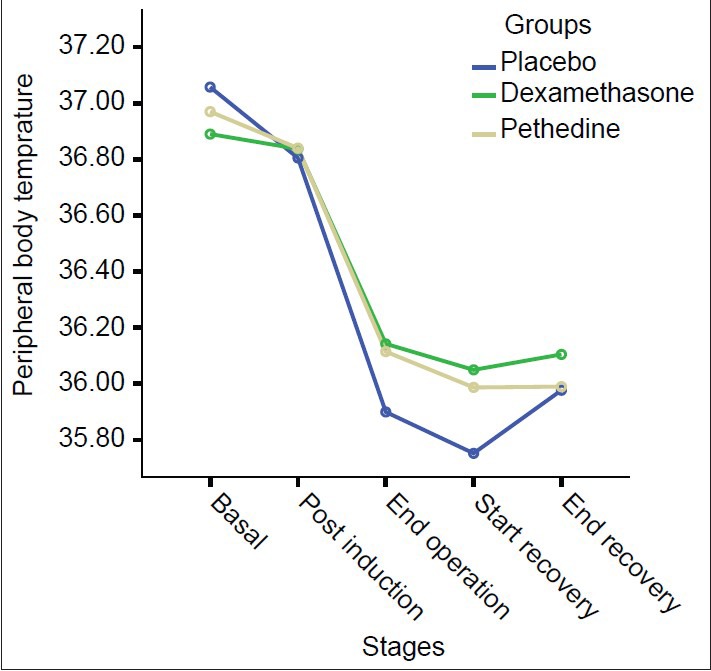
Measured skin temperature in three groups during anesthesia and recovery procedures
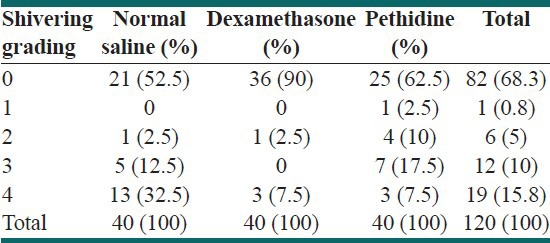
In terms of the incidence of postoperative shivering, in the dexamethasone group, four patients (10%) had shivering in the recovery process. This rate compared with the incidence of postoperative shivering in 19 patients (47.5%) of control group and 15 patients (37.5%) of pethidine group shows a significant difference (P = 0.001) [Table 4]. Intensity of shivering in three groups in recovery room has been shown in Table 5.
Table 4.
Comparison of the incidence of shivering, nausea, and vomiting in three groups of patients
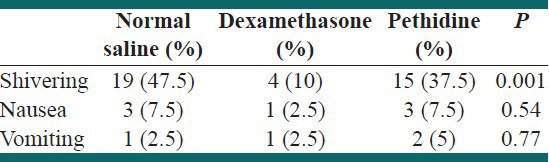
Table 5.
Shivering intensity score in three groups in recovery
Only three patients in two groups of “pethidine and control” and one patient in dexamethasone group were afflicted with postoperative nausea, which had no statistically significant difference with each other (P = 0.54). Moreover, the postoperative vomiting in two patients (5%) of pethidine and one patient (2.5%) of control and dexamethasone groups was observed. The incidence of postoperative vomiting was also not significant between the groups (P = 0.77) [Table 4]. During the operation, one of the patients in control group and the other in pethidine group was injected with 10 mg ephedrine because of hypotension.
DISCUSSION
Prevention and treatment of postoperative shivering form an important part of patient care after surgery. Since, it may cause sympathetic stimulation, increased oxygen consumption, or increased production of carbon dioxide, and hereby hurt the patient severely.
In this study which done on patients undergoing elective surgery under general anesthesia, the drugs of pethidine, dexamethasone, and placebo were used and their effects on the prevention and control of postoperative shivering were evaluated. Although mechanism of pethidine is not completely understood, it probably acts directly on the thermoregulatory center or via opioid receptors.[6] Dexamethasone can decrease the temperature gradient between core and skin via its anti-inflammatory action and inhibition of the release of vasoconstrictors and pyrogenic cytokines.[8]
The shivering incidence rate in the control group was 47.5%. While in the dexamethasone group this rate was reduced to 10% and in the pethidine group to 37.5%.
Therefore, it can be concluded that the use of pethidine before the end of surgery, compared with the control group, significantly reduces the incidence of shivering. In addition, the use of dexamethasone can also reduce the incidence of shivering, even more than pethidine. Statistically, there was a significant difference between the groups of dexamethasone and pethidine.
In a study in 1998, it was concluded that administering 0.6 mg/kg dexamethasone before induction of anesthesia can significantly reduce the incidence of shivering (13.1% compared with 33.3% of control group).[5] In a study in 2003, performed on patients undergoing heart valve replacement surgery,[9] it became clear that pretreatment with 100 mg of dexamethasone would lead to the reduction of postoperative shivering incidence. In this case, the recovery period after surgery would be shortened.
In the present study, using very low doses of this drug, similar results were obtained. This fact confirms that using the dose of 0.1 mg/kg dexamethasone could reduce the shivering incidence, in the meantime it could prevent from its side effects at higher doses. In a study conducted by Entezariasl and colleagues,[10] 4 mg ondansetron, 0.4 mg/kg pethidine, and 2 cc of normal saline solution were administered for three groups. In 13.3% (4 patients) of ondansetron and 20% (6 patients) of pethidine groups, postoperative shivering was observed. This rate was significantly reduced compared with the control group in which 50% (15 patients) were afflicted with shivering.
In a study conducted in 1997, the influence of pethidine (0.3 mg/kg) and clonidine (2 μg/kg) on the postoperative shivering in vertebral disc resection was compared with control group. In this study, the incidence of postoperative shivering in the clonidine group was 5% and in the pethidine group 25%. This rate was significantly lower than the control group (55%).[11] Pethidine effectiveness in reducing postoperative shivering has also been observed in the present study.
In a double-blind clinical trial study conducted by Farzi[12] on 250 patients aged 20 to 60 years old (men and women) in ASA class I and II, before elective surgery, the patients were randomly assigned to two groups: the dexamethasone group (0.25 mg/kg dexamethasone before induction of anesthesia) and placebo group.
Compared with placebo, dexamethasone reduced the incidence of postoperative shivering (40 % compared with 16.7 %) (P < 0.001).
In conclusion, this study showed that administering dexamethasone before induction of anesthesia was effective and reduced shivering during the recovery. Moreover, in Norouznia's study,[13] a double-blind clinical trial, 100 patients with physical status of I and II in the age range of 20-50 years old, who were candidates for cholecystectomy surgery under general anesthesia, before induction of anesthesia were randomly divided into two study groups (intravenous dexamethasone 15 μg/kg) and control group (placebo). The incidence of shivering was significantly lower in the dexamethasone group than the placebo group. (18.7% vs. 36% and P = 0.009). The influence of dexamethasone in reducing postoperative shivering compared with placebo is also observed in the present study. In a study conducted by Khoshrang, the incidence of shivering in the control group was 47.4%, while in the dexamethasone group this rate was reduced to 18.4%, and in the pethidine group, it was declined to 7.9%.[14] Despite this fact, in the present study the effect of dexamethasone in reducing postoperative shivering has been much better than pethidine and control group. Perhaps, cause of this issue, short duration of surgery and less degree of hypothermia in our patients because of keeping warm operating room environment and intravenous fluids.
In similar studies, other drugs have been used to reduce postoperative shivering, most of which cause different problems for patients.
Although the amounts of pethidine administered in the prevention or treatment of postoperative shivering rarely has a significant cardiovascular effect, this drug and other narcotic drugs have potentially high risk of respiratory disorders in patients, especially if they are administered during surgery.[15]
There are a few limitations to this investigation. First, the optimal dose of dexamethasone required to prevention of postoperative shivering has not been established. A dose of 0.1 mg/kg was selected for the current investigation based on data that this is the optimal effective dose in the prevention of postoperative shivering.[7] Future dose-response studies will be required to establish the most appropriate dosing regimen of dexamethasone for optimal prevention of postoperative shivering. Second, we observed no complications directly attributable to steroid therapy. However, our study was likely underpowered to detect uncommon adverse clinical outcomes potentially related to steroids (e.g., impaired wound healing, postoperative infection). Finally, our study limited to recovery period so this study could not compare the long-term effects of groups and length of stay in hospital between three groups.
CONCLUSION
Considering the fact that injection of dexamethasone after induction of anesthesia has been able to reduce the postoperative shivering from 47.5% to 10%, and regarding the absence of hemodynamic effects and reduction of postoperative nausea and vomiting in the use of the drug, dexamethasone can be administered after induction of anesthesia as an alternative to administration of pethidine (as a common method of prevention and treatment of postoperative shivering) particularly in patients with hemodynamic instability.
Footnotes
Source of Support: Ardabil University of Medical Sciences
Conflict of Interest: None declared
REFERENCES
- 1.Kurz A. Physiology of thermoregulation. Best Pract Res Clin Anaesthesiol. 2008;22:627–44. doi: 10.1016/j.bpa.2008.06.004. [DOI] [PubMed] [Google Scholar]
- 2.Reynolds L, Beckmann J, Kurz A. Perioperative complications of hypothermia. Best Pract Res Clin Anaesthesiol. 2008;22:645–57. doi: 10.1016/j.bpa.2008.07.005. [DOI] [PubMed] [Google Scholar]
- 3.Hoseinkhan Z, Behzadi M. Pethidine and Fentanyl in post-operative shivering control: A randomized clinical trial. Tehran Univ Med J (TUMJ) 2007;64:57–63. [Google Scholar]
- 4.Alfonsi P. Postanaesthetic shivering. Epidemiology, pathophysiology and approaches to prevention and management. Minerva Anestesiol. 2003;69:438–42. [PubMed] [Google Scholar]
- 5.Yared JP, Starr NJ, Hoffmann-Hogg L, Bashour CA, Insler SR, O’Connor M, et al. Dexamethasone Decreases the Incidence of Shivering After +Cardiac Surgery: A Randomized, Double-Blind, Placebo-Controlled Study. Anesth Analg. 1998;87:795–9. doi: 10.1097/00000539-199810000-00010. [DOI] [PubMed] [Google Scholar]
- 6.Iqbal A, Ahmed A, Rudra A, Wankhede RG, Sengupta S, Das T, et al. Prophylactic Granisetron Vs Pethidine for the Prevention of Postoperative Shivering: A Randomized Control Trial. Indian J Anaesth. 2009;53:330–4. [PMC free article] [PubMed] [Google Scholar]
- 7.Murphy GS, Sherwani SS, Szokol JW, Avram MJ, Greenberg SB, Patel KM, et al. Small-Dose Dexamethasone Improves Quality of Recovery Scores After Elective Cardiac Surgery: A Randomized, Double-Blind, Placebo-Controlled Study. J Cardiothorac Vasc Anesth. 2011;25:950–60. doi: 10.1053/j.jvca.2011.03.002. [DOI] [PubMed] [Google Scholar]
- 8.Khosravi A, Moinvaziri MT, Esmaili MH, Farbood AR, Nik-Khoo H, Yarmohammadi H. Treatment of postoperative shivering with dexamethasone: A prospective randomized clinical trial. Iran J Med Sci. 2002;27:15–7. [Google Scholar]
- 9.Essam E, Hakeem AE, Zareh ZE. Effected of Dexamethasone on the incidence of shivering and recovery in patients undergoing valve replacement surgery. J Anesth. 2003;19:361–70. [Google Scholar]
- 10.Entezariasl M, Isazadefar Kh, Mohammadian A, Khoshbaten M. Ondansetron and meperidine prevent postoperative shivering after general anesthesia. Middle East J Anesthesiol. 2011;21:67–70. [PubMed] [Google Scholar]
- 11.Grundmann U, Berg K, Stamminger U, Juckenhöfel S, Wilhelm W. Comparative study of pethidine and clonidine for prevention of postoperative shivering. A prospective, randomized, placebo-controlled double-blind study. Anasthesiol Intensivmed Notfallmed Schmerzther. 1997;32:36–42. doi: 10.1055/s-2007-995005. [DOI] [PubMed] [Google Scholar]
- 12.Farzi F, Sobhani A, Keshtkar A. Effect of Dexamethasone before induction of anesthesia on postoperative shivering. J Med Fac Guilan Univ Med Sci. 2001;39:32–6. [Google Scholar]
- 13.Norouzinia H, Heshmati F, Agdashy M, Mahouri A, Hassani E, Arshad A. The effectiveness of Dexamethasone on the prevention of postoperative shivering after general anesthesia. Urmia Med J. 2009;20:62–6. [Google Scholar]
- 14.Khoshrang H, Parvizi A, Haddadi S, Heidarzadeh A. Comparing the Effect of Pethedine, Dexamethasone and Placebo on Preventing Post-operation. Zahedan J Res Med Sci. 2007;9:9–15. [Google Scholar]
- 15.Alfonsi P, Sessler Dl, Du Manoir B, Levron JC, Le Moing JP, Chauvin M. The effects of meperidine and sufentanil on the shivering threshold in postoperative patients. Anesthesiology. 1998;89:43–8. doi: 10.1097/00000542-199807000-00009. [DOI] [PubMed] [Google Scholar]