

Abstract
Background:
Occupational exposures to workplace hazards in health-care workers can affect on their health including the reproductive system. Some exposures cause reproductive system disorders. Objective of this study was to compare reproductive system disorders between hospital personnel who work in clinical and administrative setting.
Methods:
This is a historical cohort study on clinical and administrative workers of hospitals. The study tool was flexible interview and questionnaire. Pregnant personnel had been followed until the end of pregnancy. Frequency of reproductive disorders was compared between two groups. Data were analyzed with SPSS 16, t-test, and χ2 were calculated considering P < 0.05 as significant level. Odds ratio had been calculated with a confidence interval 95%.
Results:
Frequency of menses disorders in clinical personnel especially, personnel of emergency departments were the highest and showed a significant difference between two groups (P = 0.042). The odds ratio for menses disorders in clinical personnel was 1.362 (1.008-1.84) and in administrative personnel was 0.653 (0.368-1.159).
Conclusions:
Clinical personnel are at higher risk for menses disorders compared with administrative personnel. Assessing the health of these personnel may help to improve future generation's health.
Keywords: Administrative personnel, emergency department personnel, reproductive system disorders
INTRODUCTION
The number of women who are employed has been increased for example it has been doubled in 20 years.[1,2]
At least more than 50% of employed women get pregnant in their active years and more than 40% of them have a normal pregnancy with the healthy babies[1] while others, may experience some reproductive disorders.[3,4,5,6,7,8,9,10] Presently 45% of workers are young women that 83% of them will be pregnant at some point during their employment.[3] About 50% of employers of ministry of health are women,[11] many of them are working in operation rooms and other hospital departments.[12] Occupational risk factors for them include physical risks such as ionizing radiations, and chemical risks such as anesthetic gases, chemotherapy agents, Ethylene oxide and solvents. These risk factors can affect women reproductive system and their pregnancies. Therefore, it is very important to pay attention to workers health and work place risk factors. In the 2006 Iranian census, Iran population had been reported 70 million that nearly 50% of them are women. In 1996 census, Iran had 60.1 million population, which 29.5 million of them were women (49.76%), from that 10.325 million work out of homes, many of them in hospitals and schools.[11,12]
Many studies had been performed about occupational risk factors that affect the reproductive system.[13,14,15,16,17,18,19,20,21] Nielsen in his 2005 study had been shown that anesthetic gases had unsuitable effect on the reproductive system,[6] these gases include, Nitrous Oxide, Halothane, Enflurane, Isoflurane, Desflurane, Sevoflurane, Methoxiflurane, and Fluroxene.[1]
Ladou in 2004 announced that chemotherapy drugs might affect nurses’ pregnancies outcomes and induce spontaneous abortion and fetal defects. These results indicated the need for perfect ventilation.[2]
Ethylene oxide, an agent used for sterilizing hospital devices and clothes has influence on reproductive systems.[2]
Heavy physical work during pregnancy may cause preterm delivery and low birth weight. Environmental tobacco smoke (ETS) in indoor spaces may also cause low birth weight.[1,2,3,4,5] Many studies had been shown the effects of solvents on pregnancies outcomes.[2] Some other studies had been reported the relative risk of spontaneous abortion in occupational exposure to anesthetic gases as 1.48.[10,13] Weisman et al. in 1967, Harwald in 1970, Cohen et al. in 1971 had studied operation rooms nurses, which all of them had been reported undesirable effects from their occupations. In 1972, Kill-Jones had studied anesthetic specialists, and in 1973 Kirves and Rosenburg studied anesthetic nurses, they both confirmed the relation between occupational exposures and reproductive disorders. Parouh et al. studied dental residents, in 1984 Heidem, studied dentists, in 1986 Mc Donald studied operation room nurses, and in 1995, Roland studied dental residents, all of them had not found any relation between occupational exposures and reproductive outcome.[14,15,16,17] The hazardous agents for the reproductive system that had been introduced in the scientific literature include, anesthetic gases, antineoplastic drugs, carbon monoxide, electromagnetic fields (EMF), ethylene oxide, mercury, physical stress, ionizing radiation, organic solvent, ETS, and video display terminal (VDT).[18,19,20,21]
Mercury can cause menses disorders, spontaneous abortion, low birth weight, and central nervous system defect in fetus. Carbon monoxide can cause spontaneous abortion and low birth weight. ETS is a carcinogen and can cause fetal death and low birth weight. Ethylene oxide can cause spontaneous abortion, respiratory irritation, skin disorder, and central nervous system problems. Ionizing radiation is a carcinogen and mutagen, and can cause infertility, menses disorders, spontaneous abortion, congenital defects, and so on.
Antineoplastic drugs can cause spontaneous abortion, fetal defects, and other disorders including liver disorders and nervous system problems. EMF, which is produce by electric devices, can cause spontaneous abortion and cancer in children. Solvent, cause menses disorders, spontaneous abortion and fetal defects. Physical stress such as heavy working can cause preterm delivery, low birth weight and probably spontaneous abortion.[22,23]
The objectives of the present study was to evaluate and compare women reproductive disorders such as spontaneous abortion, fetal defects, low birth weight, detachment, premature rupture of membrane, preterm delivery, infertility, menses disorders, between those who work in administrative, and clinical setting.
METHODS
Study setting
Hospitals of Mashhad University of Medical Sciences that is located in Mashhad.
Study design and target population
This was a historical cohort study, conducted on women who were employed in clinical and administrative parts of hospitals of Mashhad University of Medical sciences, about reproductive disorders. Study population was clinical and administrative workers of 10 hospitals. Pregnant participants have been followed until the end of the pregnancy. Simple random sampling method was used according to references 1 to 3.[1,2,3] With α = 0.05, β = 0.80, P1= 30% and P2= 20% study population were calculated 285 for each group (clinical and administrative). Inclusion criteria were personnel of clinical or administrative parts of hospitals with at least 4 years work experience. Exclusion criteria were any previous history of spontaneous abortion, fetal defects, low birth weight, detachment, premature rupture of membrane, pre-term delivery, infertility, and menses disorders before entering their present occupation.
Participants had been evaluated and observed for age, number of pregnancy, and body mass index.
Questionnaire design
The study method was interview using a questionnaire. The questionnaire validity and reliability was check with professors’ opinions and also through a pilot study with a correlation coefficient 85%.
This questionnaire includes, questions regarding spontaneous abortion, fetal defects, low birth weight, detachment, premature rupture of membrane, preterm delivery, infertility, and menses disorders.
Questionnaires also include questions about non occupational and occupational risk factors for reproductive disorders. Non occupational risks were age, endocrine disorders, family history, psychological stress, and occupational risks were work stress; physical or mental, exposures to chemical and physical factors, shift work, and working length.
Statistical analysis
Data were analyzed with SPSS 11.5. Frequency tables, mean, and t-test were used to compare quantitative variables, and χ2 for qualitative variables. P < 0.05 was considered significant and odds ratio had been calculated with a confidence interval 95%.
Ethical consideration
The study protocol had been approved by the Ethical Committee of Mashhad University of Medical Sciences upon participants’ oral consent.
RESULTS
In this study, 285 participants from clinical and 285 participants from administrative personnel of the hospital were participated. Clinical personnel had a mean age of 42.29 ± 5.01 years old and mean length of 19.57 ± 3.95 of years’ work experience. The mean age of administrative personnel was 44.06 ± 3.96 years old and the mean length of work experience was 22.33 ± 3.68 years. The body mass index was 22.83 ± 1.34 kg/m2 in the clinical group and 23.62 ± 1.49 kg/m2 in administrative group, the difference between two groups for body mass index were not significant (P < 0.05).
Table 1 shows the frequency of reproductive disorders and their comparison between two groups based on work experience (P < 0.05).
Table 1.
Frequency of reproductive disorders and their comparison between clinical and administrative groups according to work experience (P<0.05)
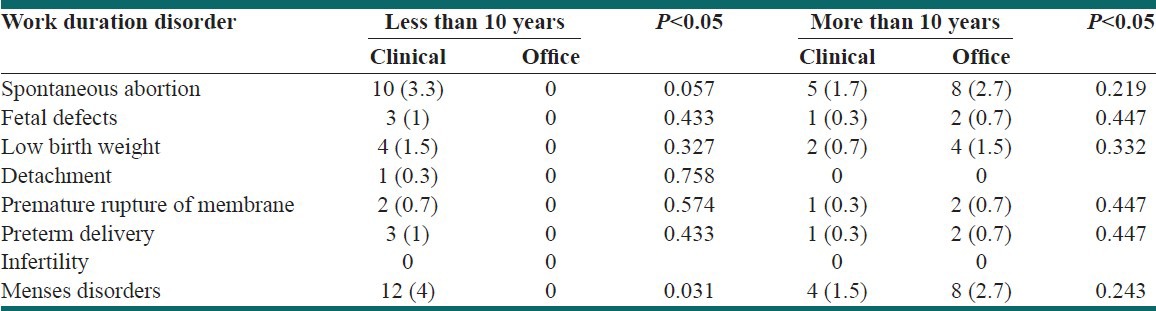
Menses disorders were significantly higher in clinical personals with less than 10 years work experience compared with administrative personnel (P = 0.031). The difference between two groups for spontaneous abortion, fetal defects, low birth weight, detachment, and premature rupture of membrane, pre-term delivery, and infertility was not significant.
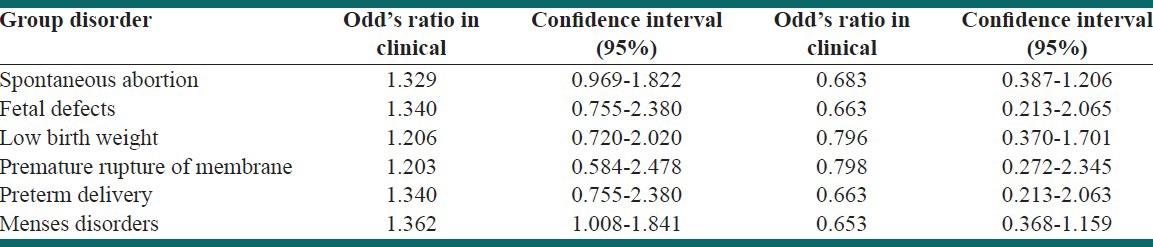
Table 2 demonstrates the comparison of odds ratio of reproductive disorders between two groups. The odds ratio for menses disorders in clinical personnel was 1.362 (1.008-1.84) and in administrative personnel was 0.653 (0.368-1.159).
Table 2.
Comparison of odds ratio of reproductive disorders between clinical and administrative personnel
Regarding the relation between work experience and reproductive disorders we did not find any significant difference between two groups. the longest related work experience belongs to administrative personnel, for example in administrative personnel the mean years of work experience before spontaneous abortion was 1.56 ± 2.75 years and in clinical personnel was 1.44 ± 2.05 years with t = −0.494 and P = 0.621.
The mean years of work experience in office personnel before having a baby with low birth weight was 1.08 ± 0.54 years and it was 1.16 ± 1.27 years for Clinical personnel, with t = −0.870 and P = 0.063.
Clinical personnel were recruited from general, radiology, emergency departments, Cardiac Unit Care, Intensive Unit Care, chemotherapy, and other hospital departments.
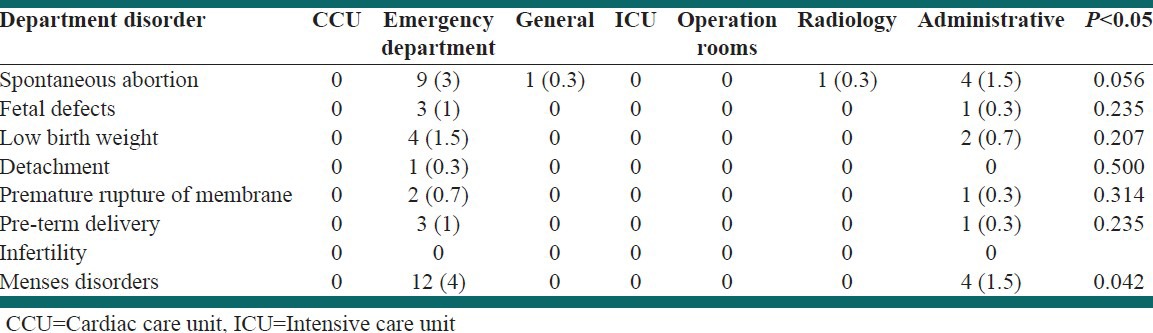
Table 3 shows the comparison of the reproductive system disorders based on different departments (P < 0.05). Emergency department personnel had significantly more menses disorders compared with others (P = 0.042).
Table 3.
Comparison of reproductive disorders in different departments with P < 0.05
DISCUSSION
The frequency of menses disorders in clinical personnel especially, those from emergency departments was high and showed a significant difference between two groups (P = 0.042). The length of work experience before disorder emerges was higher in administrative group, but the difference was not significant difference.
In the study of Nielsen in 2005 had been shown that clinical work had unsuitable effect on the reproductive system.[6] Ladou in 2004 had been reported that clinical work can affect nurses’ pregnancies outcomes and reproductive system, these results illustrated the need for perfect ventilation.[2]
Heavy physical working in pregnant women can cause reproductive disorders.[1,2,3,4,5] the effects of solvents on the reproductive system have been shown in many studies.[2] Other studies found the relation between reproductive disorders and being a healthcare worker.[10,13]
Clinical personnel with less than 10 year work experience had more reproductive disorders. The difference between two groups for menses disorders was significant (P = 0.031) and administrative personnel with more than 10 year work experience had more reproductive disorders, but the difference was not significant. It means that early reproductive system disorders are related to work type as a health-care worker or clinical setting [Table 1].
Scientific literature have been introduced the work place hazards for reproductive systems such as anesthetic gases, antineoplastic drugs, carbon monoxide,[24] EMF, ethylene oxide, mercury, physical stress, ergonomic factors,[25] ionizing radiation, organic solvent, ETS, VDT that can cause reproductive disorders.[18,19,20,21]
Reproductive system disorders have different causes.[22,23] In this study, we tried to exclude the non-occupational causes using the personnel memory about their previous medical history. According to Table 2 odds ratio for menses disorders in the clinical group was 1.362 (1.008-1.84) and in administrative personnel was 0.653 (0.368-1.159), it means that clinical environment is a risk factor for menses disorders.
Working in the emergency department can cause physical and mental stress, some chemical and drugs, radiation and also anesthetic gases for emergency's operations are among work hazards in the emergency department. According to our results working in the emergency department can be harmful for personnel's health [Table 3].
Clinical jobs had exposure to chemicals, solvents, physicals, and mental risk factors.
In this study, we did not perform exact job analysis and data were gathered from personnel's memory. Unfortunately, the number of personnel, who were able to participate in the study after considering exclusion criteria, was low. It seems that complementary study can be helpful.
Based on our study, we propose that job analysis and determination of occupational risk factors for clinical personnel is necessary.
CONCLUSIONS
Author found that frequency of menses disorders in personnel of emergency departments were higher than others, and the difference was significant. Clinical personnel are at higher risk for menses disorders compared with administrative personnel. Assessing the health of these personnel may help to improve future generation's health.
ACKNOWLEDGMENT
The author appreciated the supports of vice chancellor of research of Mashhad University of Medical Sciences.
Footnotes
Source of Support: Vice chancellor of research of Mashhad University of Medical Sciences, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Zena C, Bruce DO, Horvath JR. Vol. 3. Missouri: Mosby; 1994. Reproductive Toxicology and Occupational Exposure Occupational Medicine; pp. 836–69. [Google Scholar]
- 2.Windham GC, Osorio AM. Female reproductive toxicology. In: LaDou J, editor. Current Occupational and Environmental Medicine. Vol. 3. New York: McGraw-Hill Companies; 2004. pp. 397–413. [Google Scholar]
- 3.Pal BR, Hussein NR, Howlett A, Harun YE, Rajaratnam R. Protective medical legislation deficient knowledge of maternity (health and safety) rights for work-adjustment exists amongst flexible trainee doctors: Is there a risk to maternal and foetal health? Eur J Obstet Gynecol Reprod Biol. 2006;127:79–87. doi: 10.1016/j.ejogrb.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 4.Paul M. Occupational reproductive hazards. Biomed Ref Collec. 1997;349:62–90. doi: 10.1016/S0140-6736(96)07217-0. [DOI] [PubMed] [Google Scholar]
- 5.Gauger VT, Voepel-Lewis T, Rubin P, Kostrzewa A, Tait AR. A survey of obstetric complications and pregnancy outcomes in paediatric and nonpaediatric anaesthesiologists. Paediatr Anaesth. 2003;13:490–5. doi: 10.1046/j.1460-9592.2003.01079.x. [DOI] [PubMed] [Google Scholar]
- 6.Nilsson R, Björdal C, Andersson M, Björdal J, Nyberg A, Welin B, et al. Health risks and occupational exposure to volatile anaesthetics – A review with a systematic approach. J Clin Nurs. 2005;14:173–86. doi: 10.1111/j.1365-2702.2004.01032.x. [DOI] [PubMed] [Google Scholar]
- 7.McGregor DG. Occupational exposure to trace concentrations of waste anesthetic gases. Mayo Clin Proc. 2000;75:273–7. doi: 10.4065/75.3.273. [DOI] [PubMed] [Google Scholar]
- 8.Gruber G, Lirk P, Amann A, Keller C, Schobersberger W, Hoffmann G, et al. Neopterin as a marker of immunostimulation: An investigation in anaesthetic workplaces. Anaesthesia. 2002;57:747–50. doi: 10.1046/j.1365-2044.2002.02694.x. [DOI] [PubMed] [Google Scholar]
- 9.Byhahn C, Wilke HJ, Westpphal K. Occupational exposure to volatile anaesthetics: Epidemiology and approaches to reducing the problem. CNS Drugs. 2001;15:197–215. doi: 10.2165/00023210-200115030-00004. [DOI] [PubMed] [Google Scholar]
- 10.Russi MB, Howarth MV. Occupational medicine in the healthcare industry. In: Rosentock L, Cullen MR, Brodkin CA, Redlich CA, editors. Textbook of Clinical Occupational and Environmental Medicine. Vol. 2. United States of America: Elsevier; 2005. pp. 245–92. [Google Scholar]
- 11.Activities Report, United Nations Fund of Population. 1996;1:1–30. [Google Scholar]
- 12.Bodaghabadi M. Relationship between occupational exposure to anaesthetic gases and spontaneous abortion. Gynecol Endocrinol. 2004;18:346. [Google Scholar]
- 13.Boivin JF. Risk of spontaneous abortion in women occupationally exposed to anaesthetic gases: A meta-analysis. Occup Environ Med. 1997;54:541–8. doi: 10.1136/oem.54.8.541. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ide C. Tomorrow's children. Saf Health Pract. 2004;22:11. [Google Scholar]
- 15.Stenqvist O, Husum B, Dale O. Nitrous oxide: An ageing gentleman. Acta Anaesthesiol Scand. 2001;45:135–7. [PubMed] [Google Scholar]
- 16.Shi L, Chia SE. A review of studies on maternal occupational exposures and birth defects, and the limitations associated with these studies. Occup Med (Lond) 2001;51:230–44. doi: 10.1093/occmed/51.4.230. [DOI] [PubMed] [Google Scholar]
- 17.Saurel-Cubizolles MJ, Zeitlin J, Lelong N, Papiernik E, Di Renzo GC, Bréart G, et al. Employment, working conditions, and preterm birth: Results from the Europop case-control survey. J Epidemiol Community Health. 2004;58:395–401. doi: 10.1136/jech.2003.008029. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Shuhaiber S, Einarson A, Radde IC, Sarkar M, Koren G. A prospective-controlled study of pregnant veterinary staff exposed to inhaled anesthetics and X-rays. Int J Occup Med Environ Health. 2002;15:363–73. [PubMed] [Google Scholar]
- 19.Aminian O, Sharifian SA, Mehrdad R, Khademi A, Assadi SN. Anesthetic gases and spontaneous abortion: A historical cohort study. Arch Iran Med. 2008;11:122–4. [Google Scholar]
- 20.Figà-Talamanca I. Reproductive problems among women health care workers: Epidemiologic evidence and preventive strategies. Epidemiol Rev. 2000;22:249–60. doi: 10.1093/oxfordjournals.epirev.a018037. [DOI] [PubMed] [Google Scholar]
- 21.Assadi SN. Recommendations in health protection and fitness for work for nuclear medicine specialists. Iran J Nucl Med. 2010;18:88–9. [Google Scholar]
- 22.De cherney AH. Translated and simplified: Habibinia A. Current obstetric and gynecologic diagnosis and treatment. Tchehr. 1998;8:69–96. [Google Scholar]
- 23.Danforth DN, Scott JR. Translated and simplified. In: Rajabi MB, Rajabi MT, editors. Danforth's Obstetric and Gynecology. Vol. 1. Tehran: Andishe Rafie; 2000. pp. 1–574. [Google Scholar]
- 24.Assadi SN, Esmaily H, Mostaan L. Comparison of sensory-neural hearing between fire fighters and office workers. Int J Prev Med. 2013;4:115–9. [PMC free article] [PubMed] [Google Scholar]
- 25.Assadi SN. Cardiovascular disorders risk factors in different industries of Iran. Int J Prev Med. 2013;4:728–33. [PMC free article] [PubMed] [Google Scholar]