

Abstract
Background
Benign osteoblastoma is a rare tumor of bone representing less than 1% of all tumors of the maxillofacial region. There is a slight predilection for the mandible. More frequent sites for this tumor are the vertebral column, sacrum, long bones, and calvarium. A small predilection in males exists. The age of occurrence ranges from 5 to 37 years, with an average of 16.5. Clinically, patients have pain and swelling. The tumor contains a well-vascularized, osteoblastic connective tissue stroma. Osteoclasts may also be present. Osteoid with varying degrees of calcification, as well as immature bone, is noted.
Case report
Very few cases of osteoblastomas occurring in the jaws have been reported in the literature. This is one such a rare case report of OB occurring in a 45 year old female patient with a swelling in right lower back region since 5 years.
Summary and conclusion
Osteoblastoma has to be differentiated from other bone lesions for correct diagnosis. Many bone producing lesions possess some overlapping clinical, radiographic or histopathological findings similar to osteoblastoma. Understanding and correlating all these features is of utmost importance. This helps in correctly diagnosing and helps in adequate management of this rare entity, giving a good prognosis.
Keywords: Osteobalstoma, Osteoid osteoma, Retromolar region, Gnathic
Introduction
Osteoblastoma is a benign tumor of bone characterized by osteoid and bone formation with the presence of numerous osteoblasts. [1] This tumor was first described by Jaffe and Mayer in 1932 [2]. The current term ‘Benign osteoblastoma (OB)’ was proposed by Jaffe [3] and Lichtenstein [4] in two separate reports in 1956. Osteoblastoma constitutes about 1% of all primary bone tumors. In approximately 15% of cases it is found in the maxillofacial skeleton, with a greater frequency occurring in the mandible [5, 6]. Borello and Sedano reported the first case of osteoblastoma involving the jaws [7]. Very few cases of osteoblastomas occurring in the jaws have been reported in the literature. To the best of our knowledge, till date fewer than 100 cases of osteoblastoma of the jaws have been reported, including our cases [8–10]. Here we report such a rare case of OB occurring in a 45 year old female patient with a swelling in right lower back region since 5 years.
Case Report
A 45 year old female patient referred to Department of Oral and Maxillofacial Surgery, for swelling in right lower back region since 5 years. The swelling gradually increased to the present size. Past medical history revealed that patient underwent hospitalization for pleural effusion and treatment for the same was taken from the physician. On extraoral examination, submandibular lymphnodes were tender and palpable without any facial symmetry. Introral examination showed an elliptical, hard, non-tender swelling measuring about 5 × 3.5 cm2, extending from mandibular second molar anteriorly to the ascending ramus of mandible posteriorly. Right lower buccal and lingual vestibular obliteration was present. A provisional diagnosis of ossifying fibroma and benign odontogenic tumor was given. Incisional biopsy was taken from the centre of the lesion and the diagnosis of benign bone tumor was given. Excisional biopsy confirmed the diagnosis of Osteoblastoma.
Discussion
The benign osteoblastoma is a rare bone tumor recognized as separate entity and was distinguished from osteoid osteoma. Though Osteoblastoma is considered as a benign neoplasm of the bone, the true nature of this lesion is unknown [2]. Jaffe7 and Lichtenstein suggested that this lesion is a true neoplasm of osteoblastic derivation [3, 4]. Other investigators suggested that it occurs as a result of trauma or inflammation [11, 12]. Smith et al., have regarded this entity as an abnormal local response of the tissues to injury, or even possibly as a localized alteration in bone physiology, rather than as a true neoplasm [13].
OB seldom involves the jaws and very few cases in the literature have been reported to occur in the jaws which chiefly involve either medullary or periosteal sites [14]. The mandible is affected more often than the maxilla with most mandibular lesions occurring in the body [15].
Gordon et al. have showed that 59% of osteoblastomas occur in men and 41% in women [16]. Mandible is affected more often than maxilla and most of the mandibular lesions tend to occur in the body region [15]. Age range varies between 5 and 60 years. However, the most affected age group remains between 5 and 30 years [10].
Since the original description by Jaffe and Mayer in 1932, less than 100 well documented examples of osteoblastoma arising in the maxilla or mandible have been reported in the English literature. Figures 1, 2, 3, 4, and 5.
Fig. 1.

Photograph showing non-tender swelling in lower right retro-molar area
Fig. 2.

CT scan showing the extension of the lesion
Fig. 3.

Photograph showing operative area after the excision of the lesion
Fig. 4.
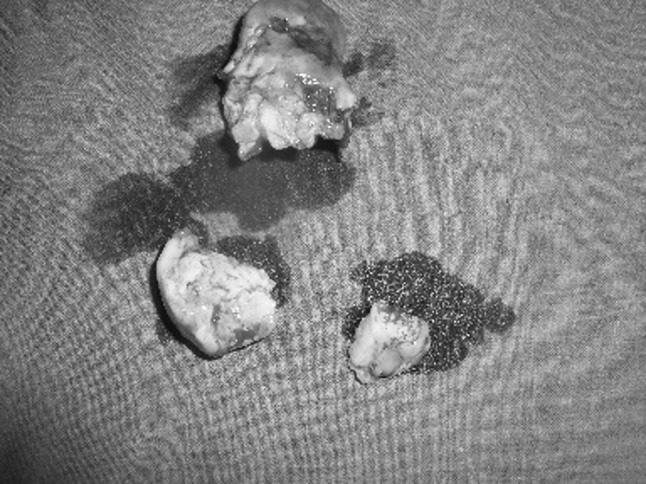
Photograph showing the excised surgical specimen
Fig. 5.
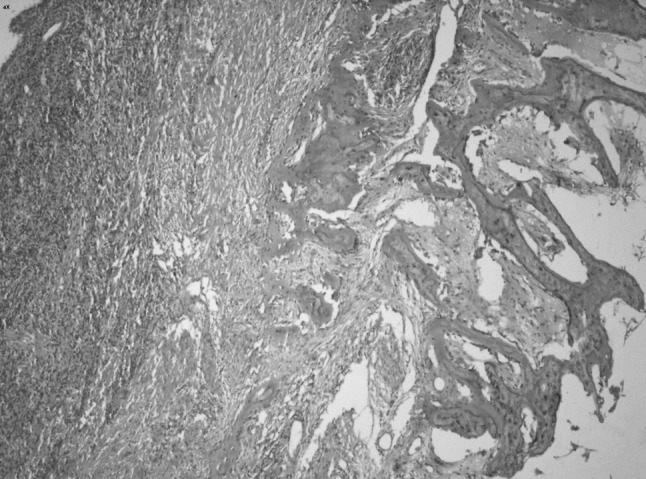
Histopathological picture showing the lesion and confirmed ‘Osteoblastoma’
Smith et al., have compared the osteoblastoma in gnathic and extragnathic sites, concluding that the lesion has similar clinical, radiologic and histologic features in both instances [13]. Osteoblastomas of the jaws are treated by curettage or local excision. En bloc resection is not commonly employed. Radiation should be considered only if surgical removal is not possible and there is evidence of continued aggressive behavior or multiple recurrences [13]. Most tumors are curetted, and bone grafts are inserted in some cases.
Overall the prognosis of osteoblastoma is good. OB has to be differentiated from other bone producing lesions such as osteoid osteoma, osteosarcoma, cementoblastoma, ossifying fibroma etc., [17].
Yang C and Qiu WL have reported 24 new cases of osteoblastoma in the maxilla and mandible. Their results suggested that osteoblastomas are more common in females than previously reported. So, the overall percentage of osteoblastoma in females increased from 47.2 to 58.4% [18].
Summary and Conclusion
Osteoblastoma has to be differentiated from other similar bone producing lesions like osteoid osteoma, osteosarcoma, cementoblastoma, ossifying fibroma etc. for correct diagnosis. Complete surgical excision is only treatment available for osteoblastoma with an overall good prognosis.
A correct diagnosis helps in proper treatment planning. Many bone producing lesions possess some clinical, radiographic or histopathological similarity to osteoblastoma. Understanding and correlating all these features is of utmost importance. This helps in correctly diagnosing and helps in adequate management of this rare entity, giving a good prognosis.
References
- 1.Jaffe HL. Tumors and tumorous conditions of the bone and joints. 3. Philadelphia: Lea and Febiger; 1961. [Google Scholar]
- 2.Jaffe HL, Mayer L. An osteoblastic-osteoid-tissue-forming tumor of a metacarpal bone. Arch Surg. 1967;24:550. doi: 10.1001/archsurg.1932.01160160022002. [DOI] [Google Scholar]
- 3.Jaffe HL. Benign osteoblastoma. Bull Hosp Joint Dis. 1956;17:141. [PubMed] [Google Scholar]
- 4.Lichtenstein L. Benign osteoblasma: a category of osteoid and bone forming tumors other than classical osteoid osteoma, which may be mistaken for giant cell tumor or osteogenic sarcoma. Cancer. 1956;9:1044–1050. doi: 10.1002/1097-0142(195609/10)9:5<1044::AID-CNCR2820090523>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- 5.Huvos AG. Bone tumors: diagnosis, treatment and prognosis. Philadelphia and London: Saunders; 1979. pp. 33–46. [Google Scholar]
- 6.Neville BW, Damm DD, Allen CM, Bouquot JE. Oral and maxillofacial pathology. Philadelphia: WB Saunders Co.; 1995. pp. 475–476. [Google Scholar]
- 7.Borello ED, Sedapo HO. Giant osteoid osteoma of the maxilla. Oral Surg. 1967;23:563. doi: 10.1016/0030-4220(67)90334-9. [DOI] [PubMed] [Google Scholar]
- 8.Rawal YB, Angiero F, Allen CM, Kalmar JR, Sedghizadeh PP, Steinhilber AM. Gnathic osteoblastoma: clinicopathologic review of seven cases with long-term follow-up. Oral Oncol. 2005;12:120–124. doi: 10.1016/j.oraloncology.2005.04.016. [DOI] [PubMed] [Google Scholar]
- 9.Jones AC, Prihoda TJ, Kacher JE, Odingo NA, Freedman PD. Osteoblastoma of the maxilla and mandible: a report of 24 cases, review of the literature, and discussion of its relationship to osteoid osteoma of the jaws. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102(5):639–650. doi: 10.1016/j.tripleo.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 10.Alvares Capelozza AL, Gião Dezotti MS, Casati Alvares L, Negrão Fleury R, Sant’Ana E. Osteoblastoma of the mandible: systematic review of the literature and report of a case. Dentomaxillofac Radiol. 2005;34(1):1–8. doi: 10.1259/dmfr/24385194. [DOI] [PubMed] [Google Scholar]
- 11.Miller AS, Rambo HM, Bowser MW, et al. Benign osteoblastoma of the jaws: report of three cases. J Oral Surg. 1980;38:694. [PubMed] [Google Scholar]
- 12.Smith NHH. Benign osteoblastoma of the mandible: report of a case. J Oral Surg. 1972;30:288. [PubMed] [Google Scholar]
- 13.Smith RA, Hansen LS, Resnick D, Chan W. Comparison of the osteoblastoma in gnathic and extragnathic sites. Oral Surg Oral Med Oral Pathol. 1982;54:285–298. doi: 10.1016/0030-4220(82)90098-6. [DOI] [PubMed] [Google Scholar]
- 14.Stewart JCB. Benign nonodontogenic tumors. In: Regezi JA, Sciubba JJ, Jordan RCK, editors. Oral pathology: clinical pathologic correlations. 4. St.Louis: Saunder; 2003. pp. 295–296. [Google Scholar]
- 15.Weinberg S, Katsikeris N, Pharoah M. Osteoblastoma of the mandibular condyle: review of the literature and report of a case. J Oral Maxillofac Surg. 1987;45:350–355. doi: 10.1016/0278-2391(87)90359-4. [DOI] [PubMed] [Google Scholar]
- 16.Gordon SC, MacIntosh RB, Wesley RK. A review of osteoblastoma and a case report of metachronous osteoblastoma and unicystic ameloblastoma. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001;91:570–575. doi: 10.1067/moe.2001.113349. [DOI] [PubMed] [Google Scholar]
- 17.Peters TE, Oliver DR, McDonald JS. Benign osteoblastoma of the mandible: report of a case. J Oral Maxillofac Surg. 1995;53:1347–1349. doi: 10.1016/0278-2391(95)90599-5. [DOI] [PubMed] [Google Scholar]
- 18.Yang C, Qiu WL. Osteoid osteoma of the eminence of the temperomandibular joint. Br J Oral Maxillofac Surg. 2001;39:404–406. doi: 10.1054/bjom.2001.0660. [DOI] [PubMed] [Google Scholar]