

Abstract
Background and Objective:
Adult age is a sensitive period of human life and paying attention to the issues and needs of this stage is a social necessity. Regarding the specific needs of this period, considering the empowerment, dignity, and self-efficacy in the elders is very important too, which is frequently neglected. This study aims to determine the effect of family-based interventions on the elders’ empowerment with emphasis on self-efficacy, self-esteem, perceive threat, and quality of life of the elders in Isfahan.
Materials and Methods:
In this semi-experimental study, 64 elderly people with the ability to perform routine and daily tasks without dependence on others and without systemic and restrictive diseases were chosen by available sampling method and were divided into two intervention and control groups. In intervention group, the model of family-based empowerment was trained and conducted in ten 45-minute sessions. The level of perceived threat, self-esteem, self-efficacy, and life quality in both groups were evaluated before and after intervention through a questionnaire. Chi Square, paired and independent t-test were used for statistical analysis.
Results:
Statistical test of paired t-test indicated that family-based empowerment model significantly increased the quality of life in intervention group compared with the control group (P < 0.01). Statistical test of independent t-test showed a significant difference in intervention and control groups after conducting the program in the score of the self-esteem (P < 0.001). Regarding self-efficiency, independent t-test did not show any significant difference between the two groups before intervention. Despite the increase of self-efficacy score after intervention, this difference was not significant (P = 0.076).
Conclusion:
Regarding the findings of this research, we can conclude that it is possible to increase the level of self-efficacy, self-esteem, perceived threat, and finally quality of life of the elders and facilitate the way for healthy aging and being healthy in this period using family-based empowerment model regularly and consistently.
Keywords: Elder, family-based empowerment model, quality of life, self-efficacy, self-esteem
INTRODUCTION
Adult age is a sensitive period of human life and paying attention to the issues and needs of this stage is a social necessity. Regarding special needs of this period, paying attention to health-promoting behaviors is an important issue which is frequently neglected.[1] Healthy aging is the right of all human beings and this issue increases the importance of adult age phenomenon and the prevention of its problems.[2] More than half (59%) of the elders’ population live in developing countries now and it is estimated that this rate will reach 71% by 2030.[3] The elders allocate themselves to about 60% of health care costs, 35% of hospital releasing, and 47% of hospitalization days in the hospital. Regarding the rapid increase of the number of elders, the issue of health and ensuring their comfort and welfare in the community, finds new and broader dimensions every day.[4]
What is considered by modern knowledge is not only prolonging life period, but rather it should also be addressed that the extra years of life be spent with comfort and physical and mental health and if such situation is not meet, scientific progresses for longer life will be useless and risky.[5] With aging, person's dependence on family for doing daily tasks increases due to disorders in different systems of body, especially due to motion limitations. These factors can have many negative effects on the feeling of being good and also on the person's quality of life.[6]
Paying attention to quality of life and the effects of different psychological considerations and modifying lifestyle can increase the efficiency and independence of the elders to a large extent, and help them in controlling various complications of aging and its different treatments.[7,8,9,10,11]
Family-based care as a philosophy of care recognize the importance of family as the main focus point in all health care supervisions, and is a way which controls the elders and families through mutual useful partnerships between supervisors.[9,12,13,14] Family empowerment means helping the family so that it can achieve the ability of change. Sometimes family's role is the role of group which tries to shape its members in different situations of life in a way that it wants them to be. In order to help the family to achieve success, we should guide them to be able to change their own lives, which include every family member.[15] Implementing an empowerment program to increase knowledge, motivation, self-esteem, and self-efficacy leading to behavioral self-control and adoption of preventive behaviors is necessary to promote health and improve quality of life.[16,17,18,19]
The aim of interventions in family-based care is promoting the ability of family members in certain areas to overcome the barriers in health fields, because without promoting their capabilities, they will not be able to overcome the barriers.[20] As longevity of people increases, the importance of health promoting behaviors becomes more apparent daily regarding maintaining the function and independence of individuals and increasing their self-efficacy. Bandura expresses that self-efficacy is the main and important requirement in changing behavior, including health behaviors.[21,22] Lack of health and incidence of chronic diseases limit the elder's activities with aging. In order to prevent dependence and crippling, empowerment programs are needed.[23] Protests and aging complications strongly affect the elder's perception of their self and have very detrimental effects on the elder's self-esteem.[24] Self-esteem is a basic requirement. Neglecting this need causes feelings such as inferiority, weakness, and helplessness and this feeling causes basic disappointment and despair by itself.[24,25]
Nakao et al.[26] investigated needs of the elders under daily nursing care at home, this study showed that physical performance parameters, routine daily activities, and exercise capacity should be considered in supportive programs. They showed that the elders’ empowerment should be considered in different grounds.
Paswan in a study titled citizens’ empowerment for retirement life showed that the elders’ empowerment improves their physical and mental capacities through talking about their needs. He showed that it is not only economic problems that hurt them, but also lack of success in social situations, not having a happy life and not living good endanger their lives. So the elders’ empowerment programs should consider these categories.[27]
Siu-Ching LO also showed about four categories of empowerment, which include mental knowledge, participation, knowledge, and learning. He believed that community-based care should consider supportive services in these areas for the elders over 60 years so that it leads to well-being and improvement of their quality of life and promotes self-esteem and having a useful and productive activity in the community.[28] Considering the above studies conducting family-based programs have left a positive effect. The families have definitely special importance in diseases and health problems, and as a patron support their clients. Regarding resulting physiological changes and special sensitivities of this period, the elders have special mentality and self-esteem, which if not considered and honored by family members, will certainly lead to acute problems challenging self-efficacy and self-esteem of the elder in the process of life. Therefore, plans considering the elders’ performance using family-based and effective approach have special importance and should be considered. Hence the researcher decided to evaluate the effect of family-based approach in the elders’ empowerment.
MATERIALS AND METHODS
The presented research is a semi-experimental study done with the participation of 64 elders aged over 55 years according to related studies[29] and resident of Isfahan in 2011. Participants were physically active and able to perform routine and daily tasks without dependence on others. The excluding criteria were neurologic deficiencies (stroke, Parkinson disease, and paralysis), cardiovascular disorders (acute myocardial infarction, acute heart failure, and uncontrolled hypertension), chronic unstable diseases (diabetes and malignancies), severe congenital deficiencies, and limiting musculoskeletal disorders.
The researcher started sampling by receiving a letter of introduction from Isfahan University of Medical Science and obtaining written permission from the elders residing in District 12 of Isfahan attending in the Gardens of damask rose, Mellat, Ghalamestan, and Fadak. After selecting qualified samples, individuals were randomly divided to control group (32 cases) and intervention group (32 cases).
Data collection tools in this study included a form of demographic characteristics, questionnaire of perceived threat measurement, Cooper Smith self-efficacy and self-esteem, and the check list of self-report recording. Content validity method was used to determine the questionnaire's validity. To determine its reliability, test–retest was used. In the questionnaire of perceived threat, which is a verified questionnaire and is scored by 5-point-option Likert instrument, experts’ opinions were applied to determine content validity. The questionnaire was given to 20 elders to be completed and its reliability was calculated by Cronbach alpha (α = 0.75). The questionnaire of Cooper Smith self-efficacy, self-esteem, and quality of life (Sf- 36) are standard tools,[17,19,20,30] which their reliabilities were calculated (α = 0.83), (α = 0.79) and (α = 0.71), respectively.
(SPSS Inc, Chicago, Illinois). Statistical Software under Windows version 18 and parametric, Mann–Whitney and Chi Square tests were used to statistically analyze data.
This study was done with the philosophy of respecting dignity of the elders and their families with the aim of empowering family-based elders. In order to implement family-based empowerment model step by step and make it applicable according to the model's concepts, four stages were designed and determined. These stages had their own continuity and consistency and were as follows: threat perception, problem solving, educational participation, and evaluation.
The first step in family-based empowerment model was the increase of perceived threat of capable factor, that is, family system including the elder person and the family. Hence one of the major tasks of the capable factor was informing and increasing capable factor's knowledge about aging. Problem solving method in this model was group discussion method in which the person practically encountered the problem and solving process and participated in offering solutions and choosing the best solution. The third stage was educational participation affected by systematic view and systematic theory. With this approach obtaining the necessary effectiveness program by family participation, the program was implemented by family participation since one of the problems of the elders and the family was lack of awareness and knowledge. After data analysis and educational needs determination, the perceived severity in these elders was increased by improving their knowledge about the aging process and the severity of complications and the aging process. One of the goals of training sessions (especially the first session) was to promote the perceived severity in research samples. This stage was performed in two training sessions, each lasted 45 minutes. In the second step, group discussion sessions were held in four 45-minute sessions in eight-member groups for the elders and their families, and they encountered actually their problems and problem-solving process and discussed with each other under the researcher's supervision by expressing objective examples of their status and the actions they have taken to improve the problem similar to others.
In the third step, discussed subjects in group discussion sessions were transferred to other family members by the elder in two 45-minute sessions, and also educational pamphlets were given to them. In the fourth step being pattern evaluation, knowledge, self-efficacy of the elders and their families after intervention were investigated in two 45-minute sessions. Evaluation was done by question and answer and group discussion in each session and the questions and ambiguities were answered. Total sum up of the meetings was done at the end of the tenth session and then a quarterly respite was given to the elders and their families to use the concepts of family-based empowerment model. In the control group, after completing questionnaires after 3 month follow-up, training program in one session along with the pamphlet was given to this group [Figure 1].
Figure 1.
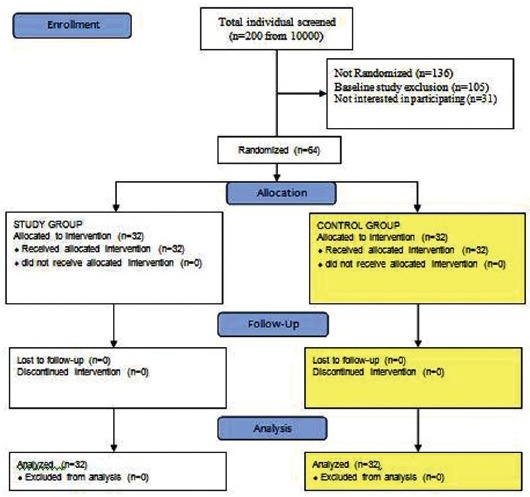
Field of study, the number of participants in the study
RESULTS
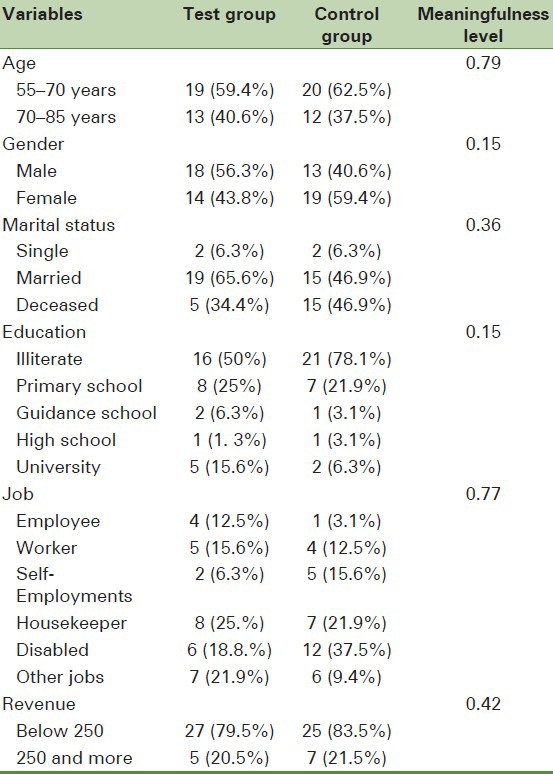
Chi Square and Mann–Whitney test did not show a meaningful difference between intervention and control groups regarding demographic data; in other words, these two groups were homogenous (P > 0.05) [Table 1].
Table 1.
Demographic information of two study groups
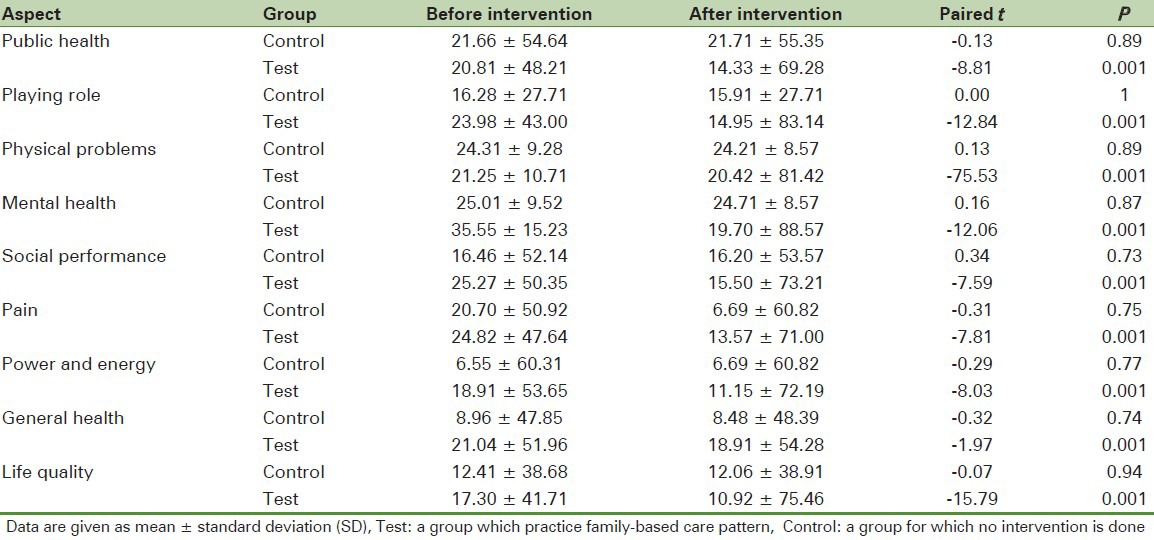
Research Findings indicate that the average difference of quality of life level between both groups did not have a significant difference before implementing family-based empowerment model; but three months after the intervention, this difference became significant so that the average of quality of life score in intervention group is increasing and is not changing in control group [Table 2]. Independent t- test showed a significant difference in two intervention and control groups after implementing the program in all aspects (P < 0.001), While this difference was not significant before intervention.
Table 2.
Average difference of life quality aspects before and after intervention in control and test group (paired t)
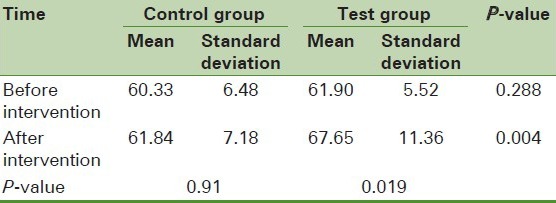
Independent t- test indicated the similarity of average score of perceived threat before training in both groups. But after educational intervention, a significant difference was found between the average score of perceived threat in both groups (P = 0.001). Paired t- test also showed a significant difference in the average score of perceived threat before and after intervention in intervention group (P = 0.027), but no significant change was found in control group [Table 3]. Before training, the average score of self-esteem was similar in both groups and independent t-test showed no significant differences between the two groups. After educational intervention, independent t-test showed a significant difference between the average score of intervention group's self-esteem (P = 0.004), [Table 4].
Table 3.
Average score of perceived threat before and after intervention
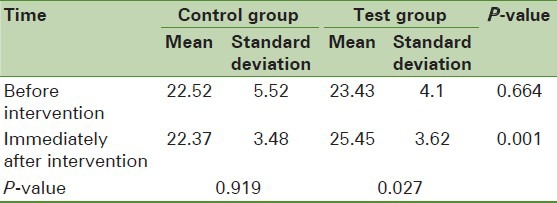
Table 4.
Average score of self-esteem before and after intervention
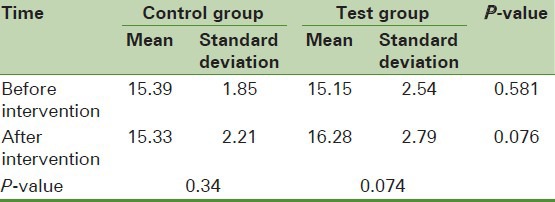
Regarding self-efficacy, there was not any significant difference between both groups before intervention. Level of self-efficiency in intervention and control groups was (15.39) and (15.15), respectively [Table 5]. But after training, independent t-test did not show any significant difference in intervention group despite the increase of self-efficacy score in this group (P = 0.076).
Table 5.
Average score of self-efficacy before and after intervention
DISCUSSION
Regarding the results of this study, implementation of family-based empowerment model has increased perceived threat, self-esteem, and finally quality of life of the elders. Regarding self-efficacy, despite the increase of the elders’ self-efficacy in this study, this difference was not significant. In, general it can be concluded that using family-based empowerment model, we can increase different aspects of quality of life, self-esteem, and perceived threat in the person and help successful aging process and pave the way for improving the elders’ quality of life so as to use the elders’ valuable experiences for promoting the community in different dimensions. Studies have shown that implementing family-based care creates positive feelings in health care personnel and reports increasing satisfaction of the elders and families. As families’ understanding and participation in care of the elders improves in these measures, their anxiety decreases.[31]
Power and control in the family is a vital issue, hence regarding the power factor in the family by which empowerment issue is affected as well as the factor of interactional communications effect which knows the individual's change as effective on the family system, it can be expected that empowerment of one family member affects the empowerment of family system for accessibility to health.[30]
Nakao et al.[26] study titled the threshold of physical activity needs for life and self-care program for elderly women with the aim of investigating the neediness of the elders under daily nursing care at home showed that physical performance parameters, routine daily activities and exercise capacity should be considered in supportive programs based on the family. They showed that the elders who follow the mentioned programs in a self-care way have better muscle power, walking capability, balance and muscle mass, and strength compared with other elders who are dependent on others in the family environment. In this research, Nakao et al. relied on family-based self-care programs for rehabilitation programs so that the elders with powerful and efficient muscles could use physical activities, daily works, and exercise in their plan to improve their quality of life. Findings of this study also confirm the study results of Nakao et al. so that programs based on the principle of self-care and family base lead the elder’ to the required capability and encourage him to continue life with a high quality.
In 2005, Paswan in a study titled citizens’ empowerment for retirement life showed that 120 participants of this study suffer meaningfully from depression, decreased ability in social and economic situations in adult age period. He showed that the general health of elderly women is better than elderly men. He noted that the elders’ empowerment improves their physical and mental capacities through talking about their needs. He showed that it is not economic problems that hurt them, but also lack of success in social situations, not having a happy life and, not living good endanger their lives. Hence the elders’ empowerment programs should consider these categories.[27]
In a study titled the elders’ voluntarily empowerment in Hong Kong 2006, Siu-Ching LO showed that community-based care should consider supportive services in mental, participation, awareness and knowledge areas so that it leads to well-being and improvement of their quality of life and promotes self-esteem and having a useful and productive activity in the community.[28] Considering the above studies along with the present study shows that conducting family-based programs have left a positive effect. The families have definitely special importance in diseases and health problems, and as a patron support their clients. Regarding resulting physiological changes and special sensitivities of this period, the elders have special mentality and self-esteem which if are not considered and honored by family members, will certainly lead to acute problems challenging self-efficacy of the elder in the process of life. Therefore, plans considering the elders’ performance using family-based and effective approach have special importance and should be considered.
Resnick et al.,[32] in the United States, in a research titled investigation of sport projects for self-efficacy of the elders residing in the city with participation of 166 elders with average age of 73 years showed that empowerment programs including physical activities and family-based and community-based programs help the elders’ empowerment meaningfully. They designed and implemented a 12-week program. After implementing the program, the elders’ hope increased significantly with P = 0.02. The study results are consistent with the findings of the present research. A program based on family and empowerment pattern will certainly bring positive results and considering family principle in planning and care programs should be considered.
Wallace et al.,[33] in the United States, in a research titled the application and the effect of community-based health promotion program on the elders showed that health promotion programs should be considered as one of the priorities and applicable principles in treatment centers. Preventive cares should be considered in supportive and preventive centers. In this research, 100 elders were monitored at home under sport and nutritional programs and safety reviews over 6 months. The study results showed that 7 to 8 scales of questionnaire sf-36 increased meaningfully in the intervention group. They suggested that empowerment programs in health centers should be emphasized, because these programs in these centers have high influence and choose the elders of these centers with high interest and pursue their plans. Findings of the present research also showed that implementation of family-based pattern leads to the improvement of all aspects of the elders’ quality of life using questionnaire sf-36.
Anderson et al.,[34] in Sweden, in a research titled the elders under welfare cares and their experiences about the last years of life with the aim of determining the elders’ experiences under welfare supports regarding quality of life in last years of life showed that the physical limitations of the elders over 75 years old receiving welfare empowerment programs and supports decrease and they feel better and higher self-esteem because they have been introverted and very sensitive in these years. They showed that the implementation of such programs promotes the elders’ respect and self-esteem and they feel more valuable. In this research, the elders’ attendants are recommended to respect family and community principle in planning on the elders’ caring to preserve the respect and value of adult age. Implementing the study within the family's framework and its effect on the elders’ empowerment are strengths points of this study and sampling is its limitation. Due to the problem of easy access to the elders, easy sampling was used. The results of this research while emphasizing the use of family foundation being also specially considered in Islam religion show that the efforts of community health officials regarding the elders’ welfare and health will produce results when empowerment programs and patterns be formed within the family's framework and with the help of all their members. Carers should also consider that useful and effective care of the elder should be done within the family's framework to promote the elders’ self-esteem and empowerment, and finally improve their life quality.
It is hoped that this research and its results could be used by researchers for improving the elders’ living conditions and doing more researches and interventions.
Since the fundamental implementation of family-based empowerment model with emphasis on the elder and all family members can enhance self-efficacy, self-esteem, perceived threat and finally quality of life, this approach is the suitable method for care programs and the sweetness of life in adult age can be multiplied based on it.
ACKNOWLEDGEMENTS
The present research is the approved plan with number 290080 of Research assistant of School of Health of Isfahan University of Medical Science. We thank this assistant for financial support and appreciate honored members of the department of Health Education and Health Promotion for their moral support and valuable advice as well as all the elders of Isfahan and their respected families and all those who helped the researcher for performing this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Simonetti JP, Ferreira JC. Coping strategies caregivers of elderly with chronic diseases develop. Rev Esc Enferm USP. 2008;42:19–25. doi: 10.1590/s0080-62342008000100003. [DOI] [PubMed] [Google Scholar]
- 2.Löfmark U, Hammarström A. Education-related differences in case fatality among elderly with stroke. Neuroepidemiology. 2008;31:21–7. doi: 10.1159/000136647. [DOI] [PubMed] [Google Scholar]
- 3.Schneider G, Driesch G, Kruse A, Wachter M, Nehen HG, Heuft G. What influences self-perception of health in the elderly? The role of objective health condition, subjective well-being and sense of coherence. Arch Gerontol Geriatr. 2004;39:227–37. doi: 10.1016/j.archger.2004.03.005. [DOI] [PubMed] [Google Scholar]
- 4.Kozaki K, Murata H, Kikuchi R, Sugiyama Y, Hasegawa H, Igata A, et al. “Activity scale for the elderly” as a measurement for the QOL of local elderly individuals and the assessment of the influence of age and exercise. Nihon Ronen Igakkai Zasshi. 2008;45:188–95. doi: 10.3143/geriatrics.45.188. [DOI] [PubMed] [Google Scholar]
- 5.Von Wichert P. The importance of atmospheric heat waves for health service in already altered people. Med Klin (Munich) 2008;103:75–9. doi: 10.1007/s00063-008-1017-z. [DOI] [PubMed] [Google Scholar]
- 6.Newsom JT, Schulz R. Social support as a mediator in the relation between functional status and quality of life in older adults. Psychol Aging. 1996;11:34–44. doi: 10.1037/0882-7974.11.1.34. [DOI] [PubMed] [Google Scholar]
- 7.Wood R, Alvarez R, Maraya B, Sanderas C. Physical fitness, cognitive function and health-related quality of life in older adults. Aging Phys Act. 2001;7:217–30. [Google Scholar]
- 8.Rowe M, Leachan E, Youg D. Evaluating the efficacy of physical activity for influencing quality of life out comes in older adults. Ann Beh Med. 1999;251:718–25. [Google Scholar]
- 9.Institute for Family –centered car. Family –centered car: Questions & Answers. 2005. [Last accessed on 2009 Aug 25]. Available from: http://www.Family centeredcare.org .
- 10.Cott CA, Falter LB, Gignac M, Badley E. Helping networks in community home care for the elderly: Types of team. Can J Nurs Res. 2008;40:19–37. [PubMed] [Google Scholar]
- 11.Mellor D, Davison T, McCabe M, George K. The management of depressed elderly care recipients: Family perspectives on the skills of professional carers. J Community Health Nurs. 2008;25:44–61. doi: 10.1080/07370010701836401. [DOI] [PubMed] [Google Scholar]
- 12.Bowden VR, Greenberg CS. Philadelphia: Lippincott Co; 2003. Pediatric Nursing Procedures; pp. 1–3. [Google Scholar]
- 13.Dolmans DH, Wolfhagen IH, Scherpbier AJ, Vleuten CP. Relationship of tutors’ group-dynamics skills to their performance ratings in problem-based learning. Acad Med. 2001;76:473–6. doi: 10.1097/00001888-200105000-00020. [DOI] [PubMed] [Google Scholar]
- 14.Sampsel D, McNichols S, Kordash RD, Bonitati D. Information for integration. A senior services program spurs development of a multi-hospital integrated network. (50-1).Health Prog. 1994;75:40–3. [PubMed] [Google Scholar]
- 15.Huber D. 2nd ed. Philadelphia: W.B. Saunders Co; 2000. Leadership & Nursing Care Management; p. 196. [Google Scholar]
- 16.Friedman MM, Bowlen VR, Jones EG. 5th ed. United States: Pearson Education; 2003. Family Nursing Recearch and theory practic; pp. 202–3. [Google Scholar]
- 17.Alhani F. PhD Dissertation. Iran: Tehran Faculty of Medical Science Tarbiat Modares University; 2003. Evaluating of family center empowerment model on preventing iron deficiency anemia. [Google Scholar]
- 18.Bomar PJ. Applying family research and theory to nursing practic. 3rd ed. U.S.A: Sunders; 2004. Promoting health in familyies; p. 375. [Google Scholar]
- 19.Meyer C, Muhlfeld A, Drexhage C, Floege J, Goepel E, Schauerte P, et al. Clinical research for patient empowerment - A qualitative approach on the improvement of heart health promotion in chronic illness. Med Sci Monit. 2008;14:CR358–65. [PubMed] [Google Scholar]
- 20.Lefebvre H, Levert MJ, Pelchat D, Lepage JG. Nature, sources, and impact of information on the adjustment of family caregivers: A pilot project. Can J Nurs Res. 2008;40:143–60. [PubMed] [Google Scholar]
- 21.Bandura A, Adams NE. Analysis of self efficacy theory in behavior change. Cognit Ther Res. 2002;23:287–308. [Google Scholar]
- 22.Fraczak B, Stawska B. Pensioners’ quality of life in social care houses. Ann Acad Med Stetin. 2007;53:98–103. [PubMed] [Google Scholar]
- 23.Ben Natan M. Perceptions of nurses, families, and residents in nursing homes concerning residents’ needs. Int J Nurs Pract. 2008;14:195–9. doi: 10.1111/j.1440-172X.2008.00687.x. [DOI] [PubMed] [Google Scholar]
- 24.Altman DG. The size of clinical trial. In: Pocock SJ, editor. Clinical trial, a practical approach. NewYork: John Wiley and Sounds; 1990. pp. 144–54. [Google Scholar]
- 25.Nakao H, Yoshikawa T, Hara T, Wang L, Suzuki T, Fujimoto S. Thresholds of physical activities necessary for living a self-supporting life in elderly women. Osaka City Med J. 2007;53:53–61. [PubMed] [Google Scholar]
- 26.Paswan S, Punia S, Balda S. Empowerment of Senior Citizens for Retired Life. J Soc Sci. 2005;11:255–6. [Google Scholar]
- 27.Siu-Ching LO. Elderly Volunteering as Empowerment. Available from: http://www.volunteerlink.net.2006 .
- 28.Knussen C, Tolson D, Brogan CA, Swan IR, Stott DJ, Sullivan F. Family caregivers of older relatives: Ways of coping and change in distress. Psychol Health Med. 2008;13:274–90. doi: 10.1080/13548500701405483. [DOI] [PubMed] [Google Scholar]
- 29.Jeong SY, Higgins I, McMillan M. The essentials of Advance Care Planning for end-of-life care for older people. J Clin Nurs. 2010;19:389–97. doi: 10.1111/j.1365-2702.2009.03001.x. [DOI] [PubMed] [Google Scholar]
- 30.Heller K. Mcklindon D, Families as “faculty” parents educating caregivers a bout family-centered care. Pediatr Nurs. 1998;22:428–31. [PubMed] [Google Scholar]
- 31.Resnick B, Luisi D, Vogel A. Testing the Senior Exercise Self-efficacy Project (SESEP) for use with urban dwelling minority older adults. Public Health Nurs. 2008;25:221–34. doi: 10.1111/j.1525-1446.2008.00699.x. [DOI] [PubMed] [Google Scholar]
- 32.Wallace JI, Buchner DM, Grothaus L, Leveille S, Tyll L, LaCroix AZ, et al. Implementation and effectiveness of a community-based health promotion program for older adults. J Gerontol A Biol Sci Med Sci. 1998;53:M301–6. doi: 10.1093/gerona/53a.4.m301. [DOI] [PubMed] [Google Scholar]
- 33.Andersson M, Hallberg IR, Edberg AK. Old people receiving municipal care, their experiences of what constitutes a good life in the last phase of life: A qualitative study. Int J Nurs Stud. 2008;45:818–28. doi: 10.1016/j.ijnurstu.2007.04.003. [DOI] [PubMed] [Google Scholar]
- 34.Stanhope M, Lancost J. US: Mosby; 2004. Community and Public Health; p. 612. [Google Scholar]