

Abstract
Introduction:
This study estimated the nutritional as well as the severe thinness status (according to the World Health Organization [WHO]) of a low-income family's adolescent girl and also their early age of life in both urban and rural adolescent girls in Bangladesh.
Materials and Methods:
This cross-sectional study measured the height, weight and muac by standard procedure for calculating the body mass index according to the WHO reference. A 2-days, 24-h food recall and food frequency questionnaire was used to estimate the food frequency, energy intake, protein and carbohydrate. A multistage, multiphase stratified cluster sampling was used to select the study population from two locations in Bangladesh: Dhaka city and the east region of Trishal (district of Mymensingh). The study subjects were low-income families’ adolescent girls (n = 214) aged 14–17 years. The two groups contained an equal number of respondents (n=107/group).
Results:
Results revealed that economic status had a significant effect on nutritional status. Nutritional status of low-income families’ adolescent were low both in urban and rural adolescents, but severe thinness rate according to the WHO of urban (22.4%) adolescents was much higher than rural (10.3%) adolescents (chi-square = 4.9 and P-value = 0.01), and was also higher at an earlier age of their life. In food intake distribution and food consumption status, the same results were seen. The percentage of never eat meat and fish of low-income families adolescent girls were (29.7%, 11.4%) in urban group and (24.4%, 6.8%) in rural group. The main food rice consumption of urban adolescents was also about half that of rural adolescents per day. The study also shows that intake of energy, protein, carbohydrate and fat were significantly different between urban and rural girls. Only 53% energy was covered of the recommended daily energy intake in urban adolescents.
Conclusion:
Based on the food recall and anthropometric results, we conclude that malnutrition is common in low-income family's adolescents, and the severe thinness rate is much higher in urban than in rural adolescents, as also their early age of life in both low-income family's adolescents girls in Bangladesh.
Keywords: Adolescents, girls, food recall, food frequency, nutrition, severe thinness (BMI < 16.00), World Health Organization (WHO), Bangladesh
INTRODUCTION
The world's adolescent population in about 1200 million persons at the age of 10–19 years and about 19% of the total population of the world faces a series of serious nutritional challenges in developing country.[1]
Bangladesh is one of the poorest countries, with over a 150 million population and densely populated countries of the world (881/sq km), and about 60 million people (40%) live below the poverty line[2] and 34.6% currently lives in urban area.[3] whereas 60.4% of the population lives in the urban area of Iran.[4] There are about 27.7 million adolescents aged 10-19 years of age in Bangladesh and about 13.7 million girls, which makes up about one-fifth of the total population,[5] and, in Iran, with a population of 15 million people, 21.90% are adolescents aged 10–19 years.[4] Sixty-seven percent and over of the adolescent girls are married. This includes 48% girls aged 15–19 years. About 50% of the pregnancies occur by the age of 18 years.[6]
Adolescence is a crucial part of their life. During this period, adolescents gain up to 50% of their adult weight, 20% or more than that of their adult height and 50% of their adult skeletal mass. Requirements of calories and protein are maximal, as also requirements of other nutrients, e.g. iron, calcium and vitamins, which increase.[7] One US study showed that female adolescents generally did not tend to increase energy intake with increasing age.[8]
Nutrition is one of the most important factors influencing the quality of human life. Nutritional status is also an important health indicator to assess a country's health status and morbidity pattern. Studies of nutrition status are very important in the adolescent of child bearing age because of low to moderate prevalence of possible deficiency.[9]
A large number of adolescent girls are suffering from malnutrition both in urban and rural areas of Bangladesh. The prevalence of malnutrition is found to be alarmingly higher among female adolescents in Bangladesh. Adolescence stunting is 36% and body mass index (BMI) is 50%.[10] Rate of anemia of adolescent girls is 25–27% (hemoglobin <12 g/ dL)[11,12] and iron deficiency in the age group of 14–18 years is 30% (serum transferring saturation <15%).[13,14] Vitamin A deficiency id prevalent in about half (47–54%) of school going children, and zinc deficiency in adolescence is unknown.[10] Pregnant and lactating women have about 60% or over insufficient caloric intake, which can produce malnourished babies.[15] The average per-capital energy intake by rural adolescent girls in Bangladesh is 81% of the recommended dietary allowance (RDA) for age.[16,17] Protein, iron and calcium are also important for growth spurt and skeletal development in adolescence. Sixty percent and more of school girls aged 10–16 years in Dhaka city consume protein, iron and calcium less than 75% of the RDA for age.[14] The quality of the next generation is directly linked to the high prevalence of chronic energy and micronutrient deficiencies of todays generation.[10]
However, little published data exits on dietary intake, anthropometric measurement and energy intake of Bangladeshi low-income family's adolescent girls in the urban and rural groups. This study is therefore helpful in evaluating the nutritional status and severe thinness (according to WHO reference of BMI) based on dietary intake and anthropometric variables of adolescents of different physiological status in the two same economic status in both urban and rural groups. This study may further provide certain information of their nutritional status of their earlier age of life.
MATERIALS AND METHODS
This cross-sectional study was conducted in two different districts, Dhaka and Mymensing. The required subjects included 214 adolescent girls (aged 14–17 years) of two same economic groups (urban, N = 107 and rural, N = 107) from the Dhaka city slum and east central parts of Bangladesh. The families of Dhaka city area were selected to represent low-income families from the urban group and families of Mymensing area were selected to represent low-income families from the rural group. A multistage, multiphase, stratified cluster sampling was used for selecting 214 low-income families’ adolescent girls in both groups. The study was conducted to estimate the levels and differentials in nutritional status, food frequency, BMI status and current health of low-income family member's adolescent girls in the urban and rural areas of Bangladesh. We used a written informed consent form to obtain consent from all participants in this study. Female interviewers, trained by social scientists and nutritionists, first visited adolescent girls at their homes with a structured questionnaire and consent form to obtain consent of the parents and to collect data on their education, occupation, dietary knowledge, 7-day food frequency, intake of daily food, muac, weight and height and their current health and, similarly, a second visit was done on Day 7 after the first visit. Field supervisors checked work of the field interviewers daily to ensure the quality of data collected in the field.
To assess their dietary knowledge, a checklist of food items (rice/wheat, potato, pulses, meat, fish, milk, eggs, vegetables and fruits, etc.) was used. Despite the possibility of recall bias, the girls were asked about their 7-day food frequency questions to assess eating patterns of energy, protein, fat and vitamin- and mineral-rich food items. A checklist was used for recording general morbidity symptoms they had experienced in the preceding 2 weeks. The checklist included fever, cough/cold, diarrhea/dysentery, stomachache, respiratory problems, ear and eye problems, skin problems and others.
Weight, height and mid-upper arm circumference (MUAC) of the girls were measured by Uniscales, locally made height scales and Teaching Aid at low cost (TALC) tape, respectively. Body weight was measured to the nearest 0.5 kg, wearing no shoes, with light clothing, on a portable weighting scale. Standing height was measured using a locally made height scale. Weight and height were used for computing BMI (weight [kg]/height [m2]) according to the reference of WHO. BMI below 18.5 was referred to as underweight and, among them, BMI under 16.00 was referred to as severe thinness, 16.00–16.99 as moderate thinness, 17.00–18.49 as mild thinness, 18.50–24.99 as normal range and over 25.00 as overweight. Mothers were inquired about age or date of birth of their daughters and household possessions of durable items. A local calendar was used for determining age or date of birth accurately.
Information regarding energy intake was collected over one day (24-h recall basis). Subjects were asked to maintain their normal dietary practice. The food recall information was collected by the female field worker. The amount of food was measured using measuring reference cups and glasses. The food was coded by food item and weight item in grams using the food code list and the food quantities manual, respectively, of the Institute of Nutrition and Food Science, University of Dhaka. The average intake of energy over one day was calculated for each individual using the computing version of the Bangladesh Food Composition Database promoted by the Institute of Nutrition and Food Science, University of Dhaka, RSDA and USDA (U.S. Department of Agriculture).
ANALYSIS OF DATA
Analysis was performed using EPI-Info and SPSS 16 windows version. Analysis of data univariate and multivariate techniques were used for estimating the differentials. The statistical analysis was carried out using χ2 test, odds ratio and Fisher test. Bivariant differentials are shown in terms of prevalence (in %) and percentage of 7-day food intake. The significance of difference was tested (chi-squared test, Fisher-F test, odds ratio) with the 5% level of confident interval, test statistic and its variance for categorical variables.
CHARACTERISTICS OF ADOLESCENT GIRLS
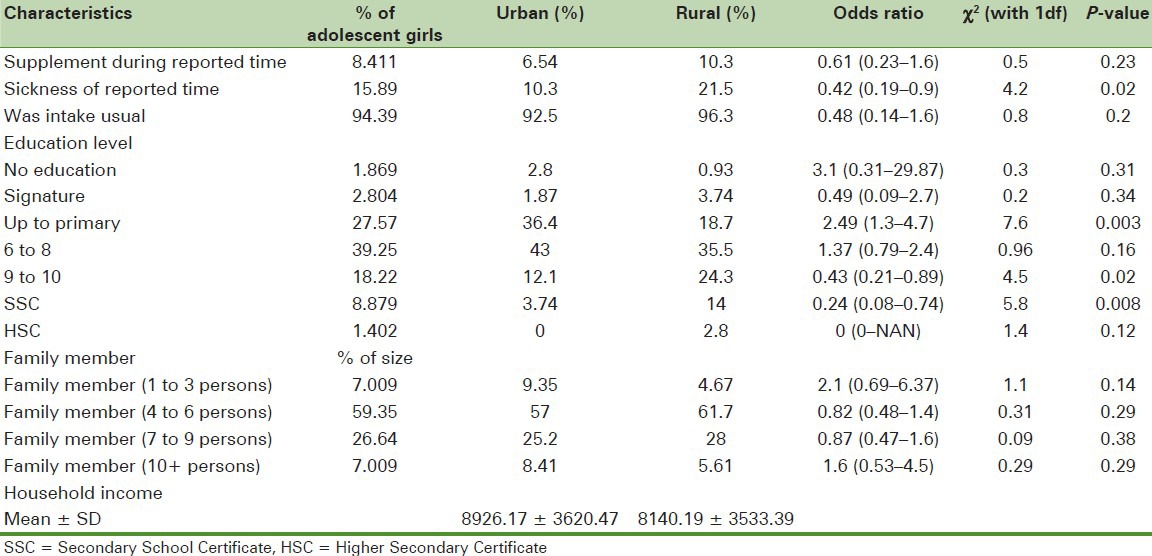
The sampled girls were young because their age limits were 14–17 years old. Very few, 1.87%, had never attended schools, and 2.8% could just sign their names; 27.57% had education up to primary school (odds ratio 2.5), 39.25% had education up to 6–8 grade, 18.22% had education up to 9–10 grade and 8.88% had completed the secondary school certification.
8.41% adolescents took supplements, 15.89% were sick at the reported time and 94.39% reported that their intake was usual at the time of reporting [Table 1].
Table 1.
Sickness, educational and economic status of low-income families’ adolescent girl
NUTRITIONAL STATUS
Nutritional status was measured with BMI-for-weight for height. BMI is a simple index of weight-for-height that is commonly used to classify underweight, overweight and obesity in adults. It is defined as the weight in kilograms divided by the square of the height in meters (kg/m2).
The following table is the International Classification of Adults as underweight, overweight and obesity according to BMI:
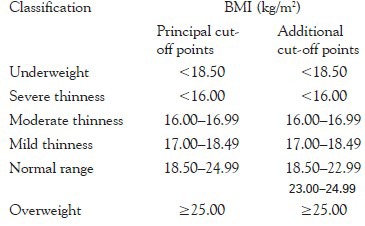
Source: Adapted from WHO, 1995, WHO, 2000 and WHO 2004.
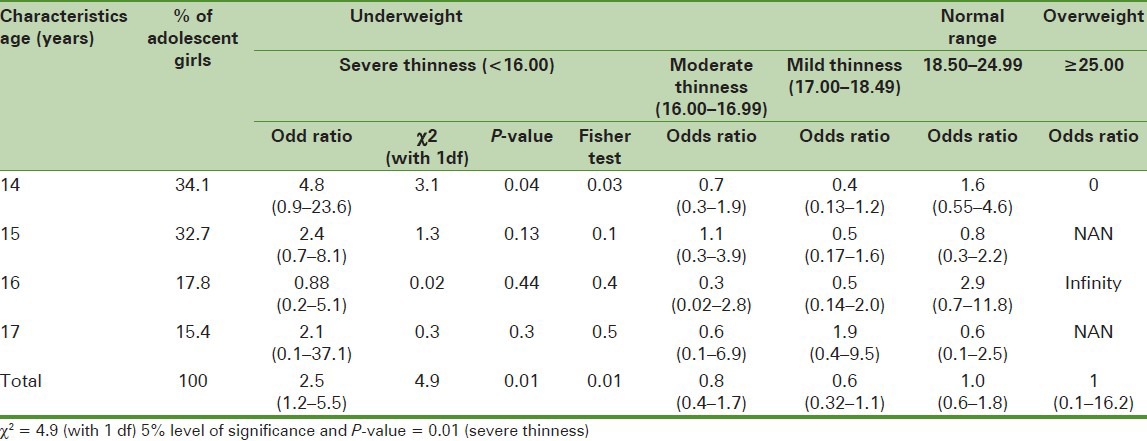
The prevalence of severe thinness was very high in the urban area at 14–17 years of age as compared with the rural area (22.43% of severe thinness in urban area whereas 10.28% of severe thinness in rural area with Chi-Square is 4.9, with a P-value of 0.01 at the 5% level of significance) [Tables 2 and 3]. In the early age of adolescent girls in the urban area, the prevalence rate of severe thinness was higher (25.6% at the age of 14 years, and fell to 9.09% at the age of 17 years), whereas it was 6.7% in the rural area at age 14 years, with odd ratios and confidence interval 4.8 (0.98–23.9). The prevalence of severe thinness was decreased with increase in age of adolescence girls in the urban area.
Table 2.
Body mass index and differentials in prevalence (%) of low-income family adolescent girls aged 14–17 years (N = 214 female adolescent girls)
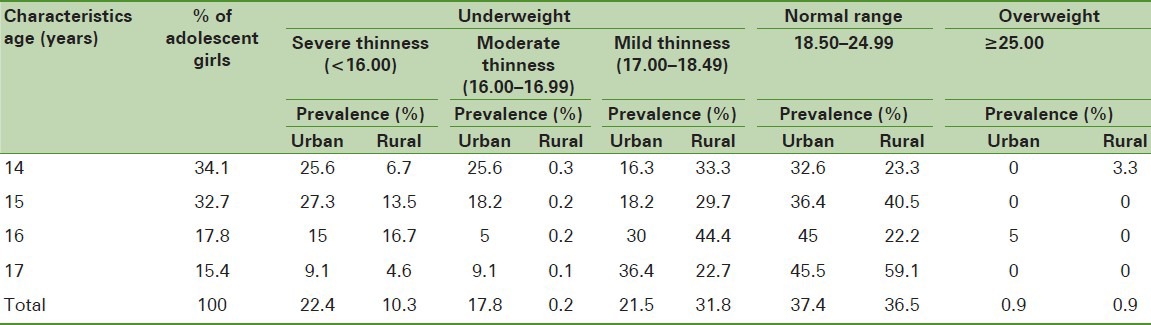
Table 3.
Differentials in odds ratio, chi square test, Fisher exact test of severe, moderate, normal and overweight among low-income family adolescent girls
The prevalence rate of mid thinness, moderate thinness, normal range and overweight of adolescent girls was likely to be similar in low-income family adolescent girls in both urban and rural areas.
SEVEN-DAY FOOD FREQUENCY
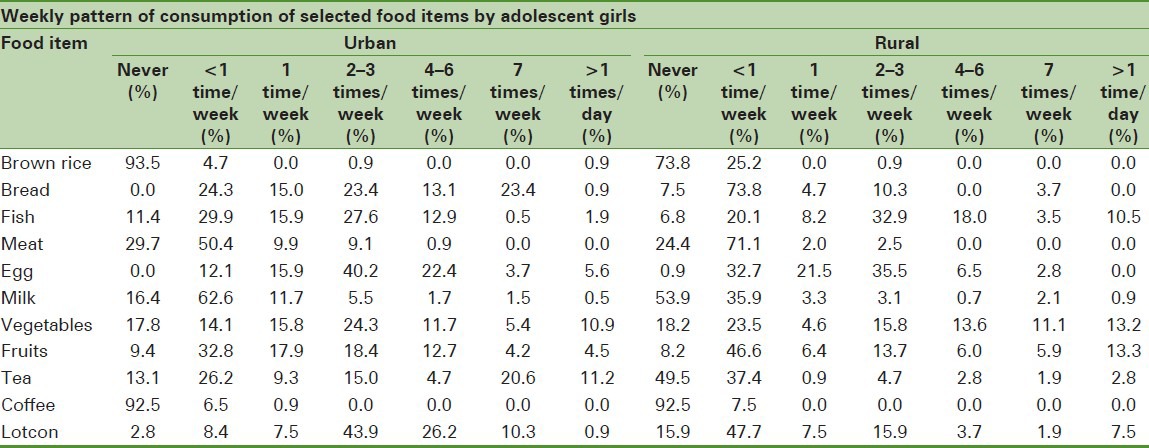
Consumption of staple food (rice, brown rice) in the last 7 days and also consumption of non-staple food (meat, eggs, lentils, fruits and leafy vegetables) were not frequent in low-income family adolescent girls in the urban and rural areas [Table 4]. 29.7% of the adolescent girls of low-income families in the urban area never eat meat, whereas 24.4% in the rural area and 71.1% of the rural adolescence girls eat meat less than one time per week (50.4% in urban area). 11.4% of adolescence girls in the urban area never eat fish (6.8% in rural area) and 10.5% of the adolescence girls in the rural area eat fish more than one time per day (only 1.9% in the urban area). The availability and consumption of fruits is quite seasonal in rural Bangladesh. 13.3% of adolescent girls eat different types of fruits more than one time per day in rural areas, whereas only 4.5% do so in the urban area. Consumption of vegetable four to six times and seven times per week and more than one time per day was 13.6%, 11.1% and 13.2% in the rural area, whereas it was 11.7%, 5.4% and 10.9% in the urban area. The percentage of consumption of egg and milk two to three times, four to six times and seven times per week was 40.2, 22.4, 3.7 and 5.5, 1.7, 1.5] in urban and [35.5, 6.5, 2.8 and 3.1, 0.7, 2.1] in rural low-income family adolescent girls of Bangladesh.
Table 4.
Percentage of weekly pattern of consumption of selected food items by adolescent girls between the urban and the rural areas
The average daily intake for energy, carbohydrates, fat and protein for adolescent girls according to the rural and urban areas is presented in Table 5.[18] Energy intake was significantly different in both the urban as well as the rural adolescent girls. There was a higher percentage of rural adolescents than urban adolescents; significant differences in energy intake were calculated for each area separately. Regarding calorie intake, it was observed that the overall calorie intake was quiet poor compared with the recommended values between the urban and the rural area. The mean calorie intake of adolescent girls in the rural area was 2004.51±177.3, which was 85% of the recommended daily calorie intake and 1253.23±92.7 in the urban area, which was only 53% of the recommended daily calorie intake. The protein and fat intake from food were also poor for urban adolescent girls compared with the rural adolescent girls.
Table 5.
Consumption of calories, protein, carbohydrate and fate of urban and rural adolescent girls

CONCLUSION
Malnutrition is a common problem in Bangladesh.[19] Malnutrition early in life of adolescent girls has long-lasting effects and affects negatively the overall growth, morbidity, cognitive development, educational attainment and adult productivity.[20] No such study has so far ever assessed and determined that low-income families’ female adolescent girls in urban areas have more severe thinness than rural adolescent girls, and are also more severe in their early age of life.[21] There was a study show that severe thinness was 9% in rural female adolescent lower than 17% in urban female adolescent found at aged 14-19 years in Bangladesh.[10,22] Based on the food recall, food intake and anthropometric results, the study revealed that malnutrition is a common feature among low-income rural and urban adolescent girls in Bangladesh,[9] but severe thinness (BMI < 16.00) of low-income families’ adolescents was very high, with more severe thinness in their early age of life in urban than in rural Bangladeshi adolescent girls according to the reference of the WHO. The study showed that the prevalence rate of severe thinness of low-income families’ adolescent girls in urban areas was 22.4% (and 13.9% in Iran,[23] whereas in rural areas it was 10.3%, and chi-square and P-values were 4.9 and 0.01 at the 5% level of significance. The prevalence rate decreases with increase of age (25.6–9.1% in urban adolescents). The same result was show in Iranian adolescent girls.[23] This could be due to a number of reasons. These differentials of nutritional status of urban Bangladesh might be accounted for by differential access to health care, or to food, or both.[17] In urban areas, different kinds of factors may also be associated with severe thinness of low-income family adolescents. These are: poor household economic condition, market price of food, food availability, periodic food shortage, not to purchase sufficient food for their needs, marker of household income-poverty, market availability, age, geographical location and cultural practices, burden of disease, poor knowledge about long-term consequences of undernutrition of adolescents, quantity and quality of food and access to health and nutrition services. Education and periodic food shortage may also associate with inadequate dietary intake in Bangladesh,[10] which might have led to undernutrition.
In Table 4, the 7-day food frequency data showed that the food consumption behavior of the urban and rural areas was also different. In the urban area, 29.7% and 11.4% of the adolescent girls of low-income families never ate meat and fish and 4.5% ate different types of fruit only once per day (24.4%, 16.8% and 13.6 in rural areas). The major cereal crops and rice consumption of the urban area was also about half that of the consumption of rural adolescent girls per day. This could be due to food availability (because of their self agricultural land) in rural areas. This study also shows that intake of energy, protein, carbohydrate and fate were also significantly difference between the urban and the rural areas of Bangladesh [Table 5]. The recommended amount of energy is 2368/day for adolescents at the age of 14–17 years, but only 53% energy is covered of the recommended daily energy intake in urban adolescent girls and 71% is covered of the recommended daily energy intake in Iranian adolescent girls.[24]
Education and economic condition was not associated with nutritional status of the low-income family's adolescent girls in both urban and rural Bangladesh. Sickness (Chi square = 4.2 with P-value = 0.02 at the 5% level of significance) was significantly associated with the risk of being severely thin.
Low-income family adolescent girls in urban areas were more severely thin because adolescent girls were not the sole decision makers; therefore, their nutritional status depended on their family. Low income and market prize of food could increase the severity in urban Bangladesh. Nutritional service and economic development could improve the overall health and decrease severity of adolescent girls in urban and rural Bangladesh. Basically, there is no such study proving that urban adolescent girls are more severely thin than rural adolescent girls in Bangladesh. More studies are needed to confirm the study findings and to protect severe thinness of the urban adolescent girls in Bangladesh.
Limitation of the study
The limitation of our study was that it was cross-sectional and therefore causality cannot be determined. The study population included adolescent urbans and rurals from low-income families’ adolescent girls; therefore, it may not be representative of all low-income families’ adolescents. Small sample size and seasonal variation of food were also major limitations of the study.
ACKNOWLEDGMENTS
The authors would like to express their sincere gratitude to the International Centre for Diarrhea Disease Research, Bangladesh (ICDDR, B) for conducting the survey and also Dr. Maleka Arjumand Jamil and Juliana Haber who were the investigators of the survey. They also want to thank Most Sharmina and Most Farida Parvin who helped in data collection and data preparation, and all those who volunteered to participate in this study.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kotecha PV, Patel S, Baxi RK, Mazumdar VS, Misra S, Modi E, et al. Reproductive health awareness among rural school going adolescents of Vadodara district. Indian J Sex Transm Dis. 2009;30:94–9. doi: 10.4103/2589-0557.62765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.HEALTH POLICY OF BANGLADESH, Ministry of Health and Family Welfare, Government of the People's Republic of Bangladesh. [Last accessed on 2012 Jan 30]. Available from: http://www.nasmis.dghs.gov.bd/mohfw/index.php?option=com_contentandtask=viewandid=388andItemid=483 .
- 3.Country health profile, world health organization Bangladesh. [Last accessed on 2012 Jan 30]. Available from: http://www.who.int/countries/bgd/en .
- 4.A paper for UNICEF-GPIA, International Conference; 2010. Adolescent Girls in Iran: Becoming a Citizen of the islamic state at the intersection of gender and youth Sepideh Yousefzadeh, Mahsa Shekarloo, April 2010. [Google Scholar]
- 5.Committee on the Rights of the Child Session on Bangladesh Second Periodic Report Geneva, Switzerland. [Last accessed on 2012 Jan 30]. Available from: http://www.ohchr.org/EN/HRBodies/CRC/Documents/statement/ds-bangladesh-2.pdf .
- 6.Unicef Bangladesh. [Last accessed on 2012 Jan 30]. Available from: http://www.unicef.org/bangladesh/children_356.htm .
- 7.Adolescent nutrition: a neglected dimension. [Last accessed on 2012 Jan 30]. Available from: http://www.searo.who.int/LinkFiles/Nutrition_for_Health_and_Development_5- Nutritional_Needs_During_Adolescence.pdf .
- 8.Wellington, New Zealand: Ministry of Health; 1998. Food and Nutrition Guidelines for Healthy Adolescents, A Background Paper - online version; pp. 2–6. [Google Scholar]
- 9.Islam MZ, Akhtaruzzaman M, Lamberg-Allardt C. Nutritional status of women in Bangladesh: Comparison of energy intake and nutritional status of a low income rural group with a high income urban group. Asia Pac J Clin Nutr. 2004;13:61–8. [PubMed] [Google Scholar]
- 10.Alam N, Roy SK, Ahmed T, Ahmed AM. Nutritional status, dietary intake and relevant knowledge of adolescent girls in rural Bangladesh. J Health Popul Nutr. 2010;28:86–94. doi: 10.3329/jhpn.v28i1.4527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ahmed T, Roy SK, Alam N, Ahmed AM, Ara G, Bhuiya AU, et al. In: Baseline survey 2004 of the National Nutritional Programme: report. Shamsul Islam Khan M, Ahmed Tahmeed, Roy Dhaka SK., editors. Bangladesh: International Centre for Diarrhoeal Disease Research; 2005. p. 319. ICDDR, B special publication no. 124. [Google Scholar]
- 12.Ahmed F, Khan MR, Islam M, Kabir I, Fuchs GJ. Anaemia and iron deficiency among adolescent schoolgirls in peri-urban Bangladesh. Eur J Clin Nutr. 2000;54:678–83. doi: 10.1038/sj.ejcn.1601073. [DOI] [PubMed] [Google Scholar]
- 13.Dhaka: Bangladesh: Helen Keller International; 1999. Helen Keller International, Bangladesh Vitamin A status throughout the lifecycle in rural Bangladesh: National vitamin A survey, 1997–98; p. 20. [Google Scholar]
- 14.Ahmed F, Zareen M, Khan MR, Banu CP, Haq MN, Jackson AA. Dietary pattern, nutrient intake and growth of adolescent school girls in urban Bangladesh. Public Health Nutr. 1998;1:83–92. doi: 10.1079/phn19980014. [DOI] [PubMed] [Google Scholar]
- 15.Food Security at a Glance, Bangladesh Poverty Map 2005 (Percent below the Lower Poverty Line) [Last accessed on 2005]. Available from: http://foodsecurityatlas.org/bgd/country/food-security-at-a-glance .
- 16.Abdullah M, Wheeler EF. Seasonal variations and the intra-household distribution of food in a Bangladeshi village. Am J Clin Nutr. 1985;41:1305–13. doi: 10.1093/ajcn/41.6.1305. [DOI] [PubMed] [Google Scholar]
- 17.Ahmad K, Hassan N. Dhaka: Institute of Nutrition and Food Science. Dhaka, Bangladesh: University of Dhaka; 1983. Nutrition survey of rural Bangladesh, 1981–82; p. 262. [Google Scholar]
- 18.Dhaka, Bangladesh: Institute of Nutrition and Food Science, University of Dhaka, INFS Dhaka University; 1992. Sources: Comprehensive listing of reference values used for planning and assessing nutrient intake. Includes information on specific nutrients and history of DRI development by United State Department of Agriculture (USDA) and INFS. Desiya Khadya Drabber Pustiman. (Nutritive Value of Indegenous Food Stuffs) [Google Scholar]
- 19.Ali abbas Mohammad Md, Masud Rana, Sabina Khan, Alamgir Azad TM, Jamila Begum, Md, Aminul Haque Bhuyan. Dietary Intake, Physical Activities and Nutritional Status of Adolescent girl in an urban population of Bangladesh. Ibrahim Med Coll J. 2010;4:78–82. [Google Scholar]
- 20.Viteri FE, Gonzalez H. Adverse outcomes of poor micronutrient status in childhood and adolescence. Nutr Rev. 2002;60(Suppl):S77–83. doi: 10.1301/00296640260130795. [DOI] [PubMed] [Google Scholar]
- 21.Kurz KM, Johnson-Welch C. Washington, DC: International Center for Research on Women; 1994. The nutrition and lives of girls in developing countries: findings from the nutrition of adolescent girls research program. [Google Scholar]
- 22.Khan MR, Ahmed F. Physical status, nutrient intake and dietary pattern of adolescent female factory workers in urban Bangladesh. Asia Pac J Clin Nutr. 2005;14:19–26. [PubMed] [Google Scholar]
- 23.Rahmani-Nia F, Rahnama N, Bambaeichi E. Prevalence of Overweight and Underweight among Iranian High-school Students. Int J Sports Sci Eng. 2008;2:101–6. [Google Scholar]
- 24.Bidad K, Anari Sh, Tavasoli S, Nazemi L, Gholami N, Zadhush S, Moayeri H. Dietary Intakes of Adolescent Girls in Relation to Weight Status. Iranian J Publ Health. 2008;37:114–8. [Google Scholar]