

Abstract
Introduction:
Although hemodialysis is therapeutic, it causes numerous physical and psychological tensions, which affect the quality of life of patients. Assessing the quality of life helps to consider clients’ problems; basically, the relationship between depression and quality of life of patients has been observed in this study.
Materials and Methods:
This was an analytic–descriptive study in which the patients received hemodialysis in Chaharmahal and Bakhtiari province. They were monitored through census method. The data collection instrument was questionnaires consisting of demography, Beck Depression Inventory, and WHO Quality-of-Life Questionnaire. The obtained data was analyzed by SPSS (Version 15) and Mann–Whitney test, Chi-square test, and t-independent test.
Results:
Ninety-five men and 76 women (171 totally) receiving hemodialysis treatment participated in the study. Chi-square test showed a significant relationship between depression and quality of life of these patients (P < 0.05).
Discussion:
Considering the present study results, it is essential to take into account depression level and quality of life in planning their care programs.
Keywords: Depression, hemodialysis patients, quality of life
INTRODUCTION
Chronic renal failure is one of the chronic disorders that needs treatment for a long-term through hemodialysis or renal transplantation. Although the best treatment is the latter one, lacking enough number of kidneys for transplantation is the main problem in most countries. Hemodialysis is, at the present time, the most common treatment for progressive renal failure around the world.[1] This is a progressive and irreversible disorder, which leads to uremia.[2] In accordance with the US Renal Data System, about 90% of the patients suffering from chronic renal disease receive hemodialysis.[3] This treatment is preferable for more than 92% of them. The number of patients receiving hemodialysis has increased 15% in Iran annually.[4] As the statistical figures show, 120–1600 individuals are diagnosed[5] as cardiovascular patients every year in this country for which hemodialysis is selected as the replacement treatment.[6] These people face some mental problems, such as anxiety, depression, isolation, denial of illness, delusion, hallucination, and a number of physiologic changes. All these complications led them to a lower quality of life leading their own life conditions and their family's getting worse gradually.[7] Although hemodialysis survives them from death, it makes some significant limitations in their lives. Therefore, it is recommended to apply adaptive methods for hemodialysis patients.[8] In fact, hemodialysis is recognized as a stressful process, which is accompanied by mental pressure and different psychosocial problems.
The most common psychosocial disorder among hemodialysis is depression.[9,10] Since hemodialysis leads to some physical, economical, social, and emotional complications for them, their quality of life diminishes and is stressful as well. So, using adaptive strategies is crucial because diverse stress-making agents influence their quality of life irreversibly. Meanwhile, nurses’ plans have a key role in assessing and making their quality of life better.[6] The studies show that mental disorders and pressures prevalence, such as anxiety, depression, and limited social support, are more among these patients rather than other people. It, consequently, causes lower quality of life. This situation is itself an important factor in frequent hospitalization and increase in mortality rate.[11] Being treated by remedial procedures after some months, they feel their quality of life has dropped massively.[8] Morsch and others study shows more awful quality of life of these patients in comparison with healthy persons.[6]
As a result, this study was conducted to determine the relationship between depression and quality of life among these patients, so that medical team members, especially nurses find out deeply the important role of stressful factors in the decrease in quality of life.
MATERIALS AND METHODS
This was an analytic–descriptive study with 171 patients receiving hemodialysis from Chaharmahal and Bakhtiari, western Iranian province, in the year 2011. After achieving the accompanying orders from the University of Medical Sciences in Shahrekord City, the list of hemodialysis centers were provided and researchers referred to them for picking the samples through census. The inclusion criteria were having medical file in hemodialysis wards, receiving hemodialysis according to a weekly schedule, and also being conscious. The exclusion criteria were not caring for cooperation in this study and moving to other cities or provinces, or out of researchers’ access. The studied cases were assured that their information kept confidential. Moreover, a comprehensive description was given to them about the study's goals and its process. Data gathering method was by Beck Depression Inventory and WHO Quality-of-Life Questionnaires. The first questionnaire consisted of 20 questions and 4 options of Lickert scale. The grades range was from 0 to 3. Given grades were converted to 0 up to 100, and the cases between 0 to 25, 26 to 50, 51 to 75, and 76 to 100 were, in turn, considered as not depressed, mildly depressed, severely depressed, and very severely depressed persons. It means that the people getting more score were in worse condition and had more depression. WHO Quality-of-Life Questionnaire consisted of 26 questions with 5 options of Lickert scale. Zero and 4 degrees mean, in turn, negative—low and positive—high levels of perception.
After changing these scores into percent, the lowest one was 0 and the highest one was 100. Then, the final grades of the patients were categorized into 4 levels as follows: from 0 to 25, 26 to 50, 51 to 75, and 76 to 100 were considered, in turn, as very inappropriate, inappropriate, appropriate, and very appropriate quality of life. The reliability and validity of Beck Depression Inventory and WHO Quality-of-Life Questionnaires have been measured as standard ones in previous researches in Iran and other countries.[12,13] The data obtained were analyzed by descriptive and analytic statistical methods. Version 15 of SPSS was used for the purpose. Chi-square test was applied to find the relationship between depression and quality of life.
RESULTS
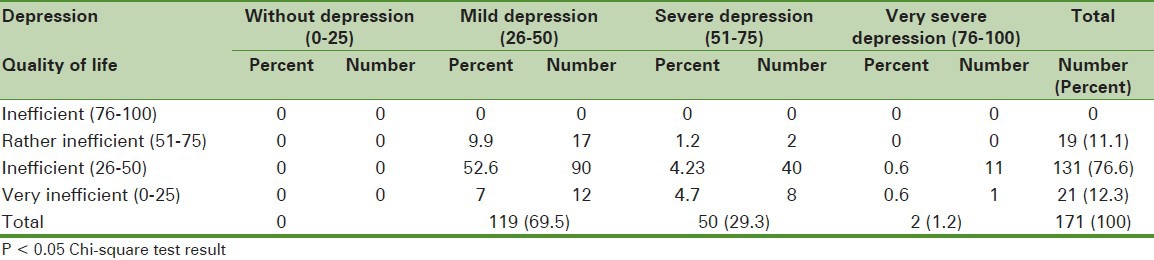
One hundred and seventy-one hemodialysis patients were studied in this research. Ninety-five of them (55.6%) were men and 76 were women (44.4%). The difference between age average in both genders was not significant as given in table 1. Most of the studied cases (55.6%) were illiterate, 31% and 69% of them were, in turn, employed and unemployed, respectively. The hemodialysis frequency of 145 cases (84.8%) was three times every week. Twenty-three (13.5%) and 3 (1.8%) of them also received hemodialysis, in turn, two times and one episode weekly. The least duration of receiving this treatment among studied cases was 1 month and the longest one was 180 months. The results showed that none of the studied patients had appropriate quality of life. Chi-square test also showed a significant relationship between depression and quality of life [Table 2].
Table 1.
Age frequency and average in men and women
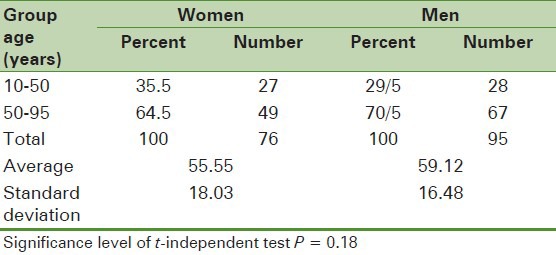
Table 2.
Frequency and correlation between depression and quality of life in patients receiving hemodyalysis
DISCUSSION
Quality of life is a valuable indicator, which is known and applied to assess health situation in public health researches. On the other hand, obtaining the data of quality of life can promote therapeutically, rehabilitation and care plans in addition to making treatments more efficient. The results derived from measuring quality of life of these patients can be used to evaluate financial and human labor costs, resulted from this disease, new plans and measures, medicine qualifications, and high technology devices impacts, psychological changes, and sociofunctional condition of these patients. As mentioned in various books and articles, quality of life measurement in clinical studies, causes to make intimate communication between patients and physicians and health care staffs, such as nurses. This leads to improve patients’ knowledge of their illness and health condition. It also makes them aware of Benefits and complications of diverse remedies to get involved this patient in selecting their therapeutic method. On the other hand, having access to health quality data can develop remedy, care-giving, and rehabilitation plans. Chronic diseases such as chronic renal failure change the quality of life tremendously during the years. The most significant factors that induce these changes are anxiety and depression among these patients. The present study is the first one that the relationship between depression and the quality of life were searched for. Most studied cases in this project were men as observed in Molahosseini and others’ research[14] and 55.6% of Sharif et al.'s cases were men.[15] This study showed that the patients quality of life was not efficient. Meanwhile, there is a direct relationship between depression and quality of life. Wu and others study results (2004) indicated more poor quality of life in hemodialysis patients physically and emotionally. The main cause of emotional distress was being treated by painfully persistent remedies. The most common emotional problems were also depression, anxiety, and suicide, which correlated with the duration of hemodialysis treatment.[16]
Diaz-Buxo patients study showed low quality of life of these patients. It implied direct correlation between their quality of life and stress. The most important agent causing trouble for them in their environment was hemodialysis procedure, which is so time-consuming for the clients.[17] Kimmel et al study results (2003) proved the positive relationship between hemodialysis and stressfulness; the longer hemodialysis history, the more stress the patients suffer from.[18] The same results were found in Tagi and others study (2007)[19]. They got this conclusion that quality of life and stages of renal failure in patients were drastically, in turn, lower and emotional and mental disorders higher than ordinary people. This affects their survival chance. At the same time, as their anxiety and depression levels go up, their quality of life became inefficient in the hemodialysis patients. Ginieri-Coccossis and others study showed that the quality life of hemodialysis patients receiving this kind of treatment for 4 years were inefficient in social, physical, and environmental dimensions. Hence, this inefficiency had direct relationship with stress, insomnia, and depression.[20]
Sayin and others (2007) found that adverse depression and anxiety had an influence on the quality of life of 75 hemodialysis clients (41 received peritoneal hemodialysis and 20 were transplantation cases). Their quality of life was the lowest one among any other studied group.[21] A 68% of hemodialysis patients were depressed as found by Cukor and others.[22]0 Sharif and others research showed a significant correlation between quality of life and mental health so that physical dimension of quality of life is significantly correlated to anxiety, functional disorder, and depression level.[15] Afshar and others found 70% of depression prevalence in hemodialysis patients among whom 28.7% were caught by severe depression. Moreover, the weekly frequencies of hemodialysis and its efficiency is significantly correlated to depression.[22] Finkelstein study results showed depression in hemodialysis patients.[24]
CONCLUSION
Evaluating quality of life and the factors leading to stress helps patients to achieve positive attitude toward life and health. As a result, it is necessary that the nurses, as the main care givers, let patients have access to this kind of information.
ACKNOWLEDGMENT
The writers of this article are much obliged to research assistance of ShahreKord University of medical sciences for providing the budget for the present research.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kimmel PL, Rolf AP. Depression in end-stage renal disease patients treated with hemodialysis: Tools, correlates, outcomes and needs. Semin Dial. 2005;18:91–7. doi: 10.1111/j.1525-139X.2005.18209.x. [DOI] [PubMed] [Google Scholar]
- 2.Smeltzer SC, Bare BG. 11th ed. Philadelphia: Lippincott William and Wilkins; 2008. Brunner and Suddarth's textbook of medical surgical nursing. [Google Scholar]
- 3.Jablonski A. The multidimensional characteristics of symptoms reported by patient on hemodialysis. Nephrol Nurs J. 2007;34:29–38. [PubMed] [Google Scholar]
- 4.Baraz SH, Mohammadi E, Boroumand B. The effect of selfcare teaching on physical problems and quality of life in dialysis patients. J Nurs Midwifery. 2005;11:51–62. [Google Scholar]
- 5.Zamanzadeh V, Heidarzadeh M, Shvandi KH. Relationship between quality of life and social support in hemodialysis patients in Imam Khomeini and Sina Educational. J Tabriz Univ Med Sci. 2007;29:49–54. [Google Scholar]
- 6.Morsch CM, Goncalves LF, Barros E. Health-related quality of life among haemodialysis patients relationship with clinical indicators, morbidity and mortality. J Clin Nurs. 2006;15:498–504. doi: 10.1111/j.1365-2702.2006.01349.x. [DOI] [PubMed] [Google Scholar]
- 7.Högl B, Kiechl S, Willeit J, Saletu M, Frauscher B, Seppi K, et al. Restless legs syndrome: A community-based study of prevalence, severity, and risk factors. Neurology. 2005;64:1920–4. doi: 10.1212/01.WNL.0000163996.64461.A3. [DOI] [PubMed] [Google Scholar]
- 8.Tagay S, Kribben A, Hohenstein A, Mewes R, Senf W. Posttraumatic stress disorder in hemodialysis patients. Am J Kidney Dis. 2007;50:594–601. doi: 10.1053/j.ajkd.2007.06.018. [DOI] [PubMed] [Google Scholar]
- 9.Daugirdas JT, Blake PG, Ing TS. 4th ed. Vol. 27. Boston: Lippincott Williams and Wilkins; 2007. Hand book of dialysis; pp. 455–6. [Google Scholar]
- 10.Fukunishi I, Kitaoka T, Shirai T, Kino K, Kanematsu E, Sato Y. Psychiatric disorders among patients undergoing hemodialysis therapy. Nephron. 2002;91:344–7. doi: 10.1159/000058418. [DOI] [PubMed] [Google Scholar]
- 11.Smeltzer SC, Bare BG. 10th ed. Philadelphia: Lippincott William and Wilkins; 2004. Brunner and Suddarth's textbook of medical surgical nursing. [Google Scholar]
- 12.Jahanlou SH. Sobhani, A comparison of two standard quality of life questionnaires for evaluation of the relationship between personality characteristics and glycemic control in diabetic patients. Arak Med Univ J. 2010;13:28–34. [Google Scholar]
- 13.Sajjadi M, Akbari A, Kianmehr M, Atarodi AR. The relationship between self-care and depression in patients undergoing hemodialysis. Ofogh-e-Danesh, J Gonabad Univ Med Sci Health Serv. 2008;14:13–8. [Google Scholar]
- 14.Molahosseini SH, Mohammadzadeh SH. Frequency of sleep disorder and restless legs syndrome in patients referring to hemodialysis units. Tehran Univ Med Sci. 2003;8:27–30. [Google Scholar]
- 15.Sharif F, Vedad F. The Relationship Between Mental Health and Quality of Life of Hemodialysis Patients Referred to Hospitals Affiliated to Shiraz University of Medical Sciences. Iran J Nurs. 2007;20:61–9. [Google Scholar]
- 16.Wu AW, Fink NE, Marsh-Manzi JV, Meyer KB. Changes in quality of life during haemodialysis and peritoneal dialysis treatment: Generic and disease specific measures. J Am Soc Nephrol. 2004;15:743–53. doi: 10.1097/01.asn.0000113315.81448.ca. [DOI] [PubMed] [Google Scholar]
- 17.Diaz-Buxo JA, Lowrie EG, Lew NL, Zhang H, Lazarus JM. Quality-of-life evaluation using Short Form 36: Comparison in haemodialysis and peritoneal dialysis patients. Am J Kidney Dis. 2000;35:293–300. doi: 10.1016/s0272-6386(00)70339-8. [DOI] [PubMed] [Google Scholar]
- 18.Kimmel PL, Seth LE, Newmann JM, Danko H, Moss AH. ESRD patient quality of life: Symptoms, spiritual beliefs, psychosocial factors and ethnicity. Am J Kidney Dis. 2003;42:713–21. doi: 10.1016/s0272-6386(03)00907-7. [DOI] [PubMed] [Google Scholar]
- 19.American journal of kidney diseases : the official journal of the National Kidney Foundation. “Am J Kidney Dis. Posttraumatic stress disorder in hemodialysis patients. 2007;50(4):594–601. doi: 10.1053/j.ajkd.2007.06.018. [DOI] [PubMed] [Google Scholar]
- 20.Ginieri-Coccossis M, Theofilou P, Synodinou C. Quality of life, mental health and health beliefs in haemodialysis and peritoneal dialysis patients: Investigating differences in early and later years of current treatment. BMC Nephrol. 2008;9:1–9. doi: 10.1186/1471-2369-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sayin A, Mutluay R, Sindel S. Quality of life in hemodialysis, peritoneal dialysis and transplantation patients. Transplant Proc. 2007;10:3047–53. doi: 10.1016/j.transproceed.2007.09.030. [DOI] [PubMed] [Google Scholar]
- 22.Cukor D, Coplan J, Brown C, Peterson RA, Kimmel PL. Course of depression and anxiety diagnosis in patients treated with hemodialysis: A 16-month follow-up. Clin J Am Soc Nephrol. 2008;3:1752–8. doi: 10.2215/CJN.01120308. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Afshar R, Ghaedi G, Sanavi S, Davati A, Rajabpour A. Depression and related factors in patients undergoing conventional maintenance hemodialysis. J of Daneshvar medicine shahed University of medical sincese. 2010;17:59–66. [Google Scholar]
- 24.Susan H, Finkelstein Depression in chronic dialysis patients: assessment and treatment. Nephrol.Dial.Transplant. 2000;15(12):1911–1913. doi: 10.1093/ndt/15.12.1911. [DOI] [PubMed] [Google Scholar]