

Abstract
Background:
Health education for the school age child is a specialized field within the broad discipline of education. Oral health education program are educational aspects of any curative, preventive and promotional health activity.
Aim:
The study has been undertaken to evaluate the impact of oral health education on the status of plaque, gingival health and dental caries among 12 and 15 years old children attending government school in Shimla city.
Materials and Methods:
Two hundred and seventy six school children participated in the study. The study was conducted over a period of 4 months from May 2010 to August 2010 in Government Senior Secondary School, Sanjauli. Plaque, gingival and caries status was assessed by using Silness and Loe plaque index, Loe and Silness gingival index and WHO modified DMFT index, respectively. Data was analyzed using the software SPSS version 15. Paired t-test and Wilcoxon signed rank sum test were used appropriately for statistical comparisons. P value ≤0.05 was considered statistically significant.
Results:
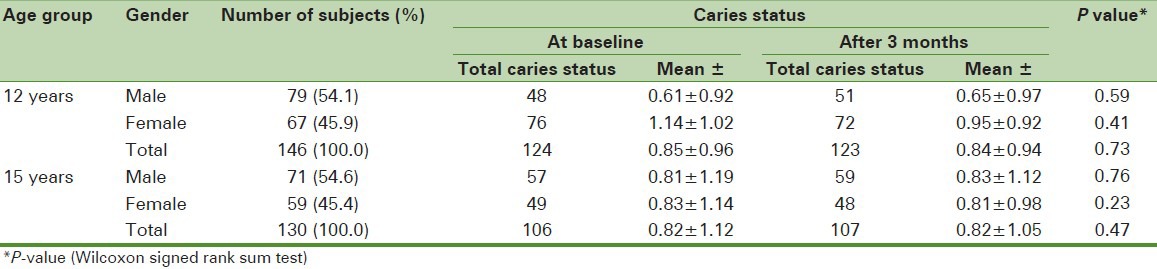
Overall mean plaque score and gingival score decreased significantly after oral health education irrespective of gender. However, decrease in plaque score among 15 years old female children and gingival scores among 12 and 15 years old female subjects was not significant. Difference in mean caries status was statistically insignificant among all the subjects.
Conclusion:
Short term oral health education program may be useful in improving oral hygiene and gingival health. Coordinating efforts should be enhanced between school personnel, parents and health professionals to ensure long-term benefits of such program.
Keywords: Dental caries, gingival status, oral health education, plaque, school children
INTRODUCTION
Health is a common theme in most cultures and is a fundamental human right without distinction of race, religion, and political belief, economic and social condition.[1] Oral health is a standard of health of the oral and related tissues that enables an individual to eat, speak and socialize without active disease, discomfort or embarrassment and contributes to the general well being. It is concerned with maintaining the health of craniofacial complex, the teeth and gums, as well as the tissue of the face and head that surrounds the mouth.[2] Oral health is an integral part of general health.[3] Oral diseases are major health problem, especially in children, owing to their high prevalence and incidence in all the regions of the world. At the global level, prevalence rates and pattern of oral disease have changed considerably over the past two decades.[4,5] Increasing levels of dental caries among children are observed in some developing countries, especially for those countries where community and school based preventive oral care programs are not established.[6] Health education is an important tool of public health and an effective primary preventive method. Efficient dental health education should incorporate oral health instructions and methods to eliminate plaque. Research has revealed the efficacy of health education in controlling plaque and thereby dental diseases.[7,8,9] Health education programs are not isolated events but educational aspects of any curative, preventive and promotional health activity.[10] Health education for the school age child is a specialized field within the broad discipline of education. No evaluation study of oral health education program for school children have been reported till date in Himachal Pradesh. Hence, the present study has been undertaken to evaluate the impact of oral health education on the status of plaque, dental caries and gingival health among 12 and 15 years old children attending government school in Shimla city.
MATERIALS AND METHODS
A total of 306 children of both genders studying at Government Senior Secondary School Sanjauli, Shimla aged 12 and 15 years were examined on the first visit. The study was conducted over a period of 4 months from May 2010 to August 2010. Prior to the conduct of the study, the purpose was clearly explained to the school authorities and written permission was obtained. Consent was obtained from the parents and teachers of the students. A one time verbal consent was taken from each study subject in the presence of class teacher. This study was approved by the institutional ethical committee. Only 276 children were available for the examination after 3 months. Inclusion Criteria: All the children aged 12 and 15 years who were present in the school on the day of examination and were willing to participate in the study. Exclusion Criteria: Those children under antibiotic therapy within 30 days of the initial examination, undergone oral prophylaxis and those who were absent on the day of examination were excluded from the study. At the initial visit, each subject was interviewed using a specially designed questionnaire and examined for plaque, gingival and caries status by using Silness and Loe plaque index,[11] Loe and Silness gingival index[12] and WHO modified DMFT index.[13] The questionnaire collected information regarding oral health habits and visit to the dentist. The data was collected by the investigator himself. A trained recorder was made to sit close to the examiner so that instructions could be heard easily. The examiner was calibrated in the college O.P.D. and kappa statistics showed higher degree conformity with the observations (Kappa co-efficient = 0.9).
After collecting the base line data, oral health education was imparted to children, which included instructions on the importance of maintenance of oral hygiene, use of appropriate oral hygiene aids and demonstration of the method of tooth brushing. Bass method of tooth brushing was taught as it is the easiest and most effective technique for the children to learn.[14] Information regarding common oral diseases and their prevention was also provided. Oral health education was supplemented with the use of teaching resources such as chalk and blackboards, models, posters and charts. Daily, twice tooth brushing was emphasized for prevention of bad breath and tooth decay. To evaluate the effectiveness of the educational program, the presence of plaque, gingivitis and dental caries was assessed at the end of 3 months.
The data was analyzed using the software SPSS version 15 (SPSS Inc., Chicago) to find out the differences between plaque scores, gingival and caries status before and after the education program. Paired t-test was used to evaluate the changes in the plaque and gingival status at baseline and after 3 months. Wilcoxon signed rank sum test was used to find the difference in mean caries status (DT) of the subjects before and after dental health education. P value ≤0.05 was considered statistically significant.
RESULTS
A total of 306 school children were examined at the baselines and 276 were examined after 3 month period at the time of follow-up. Attrition in the study was 30 children (9.8%). In the age group 12 years, 146 school children were examined out of which 79 (54.1%) were males and 67 (45.9%) were females. Among 130, 15 years old children 71 (54.6%) and 59 (45.4%) were males and females, respectively. Questionnaire was analyzed according to their responses. Majority of school children 257 (93.1%) were using toothbrush, with once a day history of tooth brushing 220 (79.7%). Majority of 248 (89.8%) were using tooth paste. Two hundred and thirty six (91.8%) practiced a faulty horizontal pattern of cleansing with brush, whereas 21 (8.2%) employed the vertical method of tooth brushing [Table 1]. Significant reduction was observed for plaque and gingival score (P > 0.05) among 12 and 15 years subjects irrespective of gender [Tables 2 and 3]. However, difference in mean caries status was statistically insignificant [Table 4].
Table 1.
Distribution of study subjects according to different variables
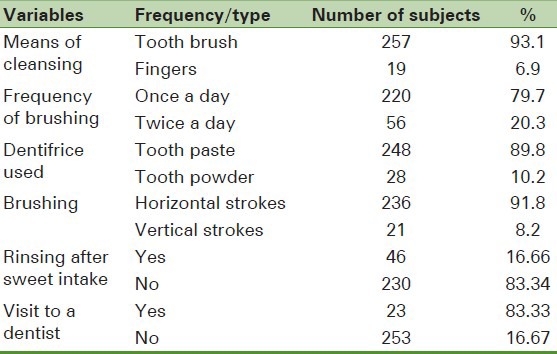
Table 2.
Plaque score of the study subjects at baseline and 3 months after oral health education
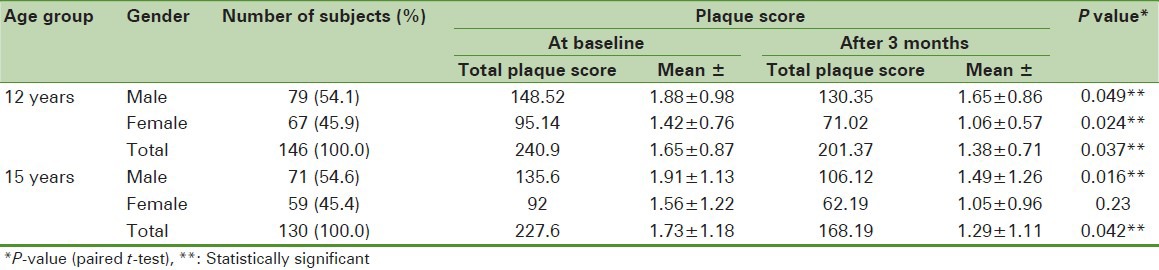
Table 3.
Mean gingival score of study subjects at baseline and 3 months after oral health education
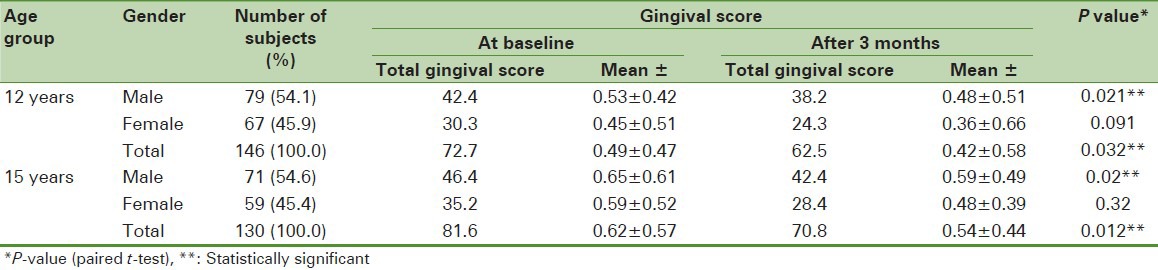
Table 4.
Mean caries status of study subjects at baseline and 3 months after oral health education
DISCUSSION
The present study was targeted at school going children because of the ease of accessibility. School forms an environment that provides considerable number of individuals of the same age and strata. Pretest questionnaire was used to access the oral hygiene practices and visit to a dentist. Since the analysis of the questionnaire revealed poor dental attendance and inadequate oral hygiene habits, the oral health education emphasizing on proper method of tooth brushing, the importance of oral hygiene and regular dental checkup was provided. In 15 years age group, no significant difference was found among female study subjects, whereas the reduction in the plaque scores was significant among male subjects. Reason for the less improvement of oral hygiene among 12 years old study subjects may be because of failure of younger study subjects in complying with the instruction given during oral health education program.[15] Reduction in plaque and gingival scores may be due to change in tooth brushing frequency and adoption of appropriate tooth-brushing technique after oral health education.[16] Older study subjects, particularly female subjects showed better understanding of oral health education program. Rayner JA,[17] Ivanovic, et al.[18] and Ajith Krishnan, et al.[9] have found similar significant reduction in mean plaque scores after oral health education in their studies.
Similar results were obtained in the studies,[19,20] which revealed an improvement in Silness and Loe index, which has been used in the present study also. However, contrary to the results of this study, Franklin, et al.[21] and Helderman, et al.[22] found no significant reduction in plaque scores. Gingival bleeding is commonly used to evaluate the status of oral hygiene of children. Significant reduction in the gingival scores was observed in the study depicting the transient improvement of gingival health. Similar results were observed in the study conducted by Shenoy, et al.[23] and Petersen, et al.[24] No significant reduction in the gingival scores were found in the studies.[9,19] Reduction in the mean caries status of the study subjects was insignificant, which is in agreement with the results of the studies.[9,18,19,22]
CONCLUSION
The study revealed that short term oral health education program may be useful in improving oral hygiene and gingival health but not effective in improving caries status. Reinforced oral health education may improve oral hygiene and gingival health to a significant extent, but may prove inadequate in the long run if low cost oral hygiene aids are not made available to the general population, which is an uphill task. Such programs should be conducted annually in the schools with the provision of oral hygiene aids at concessional rates. In the present study, parental participation was not included, which is otherwise essential for the achievement of long term benefits of the enhancement of the program for implementation during their stay at home. Long term value of the improvement need to be confirmed by further studies because improved oral hygiene in children may exist only during the program or a short period thereafter. School personnels and teachers should be involved. A chapter on importance of oro-dental health should be included in the syllabus. Coordinating efforts should be made between school personnel, health professionals and parents to ensure long-term benefits of such programs.
ACKNOWLEDGMENT
I thank all the children who agreed to take part in this study, their parents, teachers, Principal of Government Senior Secondary school Sanjauli and administration of Government Dental College and Hospital Shimla.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Park K. Park's text book of preventive and social medicine. 20th ed. Jabalpur India: M/S Banarsidas Bhanot publishers; 2009. Man and medicine: Towards health for all; pp. 1–11. [Google Scholar]
- 2.Yewe-Dyer M. The definition of oral health. Br Dent J. 1993;174:224–5. doi: 10.1038/sj.bdj.4808131. [DOI] [PubMed] [Google Scholar]
- 3.Dunning JM. 4th ed. Cambridge: Harvard University Press; 1986. Principles of dental Public Health. [Google Scholar]
- 4.Lundstrom F. Systematic plaque control in children undergoing long-term orthodontic treatment. Eur J Orthod. 1980;2:27–39. [PubMed] [Google Scholar]
- 5.Taani DQ. Relationship of socioeconomic background to oral hygiene, gingival status, and dental caries in children. Quintessence Int. 2002;33:195–8. [PubMed] [Google Scholar]
- 6.Rao A, Sequeira SP, Peter S. Prevalence of dental caries among school children of Modibidri. J Indian Soc Pedod Prev Dent. 1999;17:45–8. [PubMed] [Google Scholar]
- 7.Wang NJ, Kalletstal C, Petersen PE, Arnadottir IB. Caries preventive services for children and adolescents in Denmark, Iceland, Norway and Sweden: Strategies and resource allocation. Community Dent Oral Epidemiol. 1998;26:263–71. doi: 10.1111/j.1600-0528.1998.tb01960.x. [DOI] [PubMed] [Google Scholar]
- 8.Hartono SW, Lambri SE, van Palenstein Helderman WH. Effectiveness of primary school-based oral health education in West Java, Indonesia. Int Dent J. 2002;52:137–43. doi: 10.1111/j.1875-595x.2002.tb00618.x. [DOI] [PubMed] [Google Scholar]
- 9.Ajithkrishnan CG, Thanveer K, Sudheer H, Abhishek S. Impact of oral health education on oral health of 12 and 15 years old school children of Vadodara city, Gujarat state. Journal of International Oral Health. 2010;2:15–21. [Google Scholar]
- 10.Jong AW. 3rd ed. Bombay: Varghese Publishing House; 1994. Community Dental Health; p. 197. [Google Scholar]
- 11.Silness J, Loe H. Periodontal disease in Pregnancy. II. Correlation between oral hygiene and periodontal condtion. Acta Odontol Scand. 1964;22:121–35. doi: 10.3109/00016356408993968. [DOI] [PubMed] [Google Scholar]
- 12.Beck JD, Arbes SJ. Epidemiology of gingival and periodontal disease. In: Newman MG, Takei HH, Carranza FA, editors. Carranza's Clinical Periodontology. 9th ed. Philadelphia: Saunders; 2003. pp. 74–94. [Google Scholar]
- 13.Marya CM. 1st ed. New Delhi: Jay Pee Brothers Medical Publishers (P) Ltd; 2011. Text book of public health dentistry; pp. 204–5. [Google Scholar]
- 14.Tandon S, Roy RK, Kapoor DN, Mathur RM. Comparative evaluation of brushing techniques on children. J Indian Dent Assoc. 1977;46:291–5. [Google Scholar]
- 15.Makuch A, Reschke K, Rupf S. Effective teaching of tooth-brushing to preschool children. J Dent Child (Chic) 2011;78:9–12. [PubMed] [Google Scholar]
- 16.Tsamtsouris A, White GE, Clark ER. The effect of instruction and supervised toothbrushing on the reduction of dental plaque in kindergarten children. ASDC J Dent Child. 1979;46:204–9. [PubMed] [Google Scholar]
- 17.Rayner JA. A dental health education programme, including home visits, for nursery school children. Br Dent J. 1992;172:57–62. doi: 10.1038/sj.bdj.4807770. [DOI] [PubMed] [Google Scholar]
- 18.Ivanovic M, Lekic P. Transient effect of a short-term educational programme without prophylaxis on control of plaque and gingival inflammation in school children. J Clin Periodontol. 1996;23:750–7. doi: 10.1111/j.1600-051x.1996.tb00605.x. [DOI] [PubMed] [Google Scholar]
- 19.Worthington HV, Hill KB, Mooney J, Hamilton FA, Blinkhorn AS. A cluster randomized controlled trail of dental health education programme for 10 years old children. J Public Health Dent. 2002;61:22–7. doi: 10.1111/j.1752-7325.2001.tb03351.x. [DOI] [PubMed] [Google Scholar]
- 20.Vanobbergen J, Declerck D, Mwalili S, Martens L. The effectiveness of a 6 year oral health education programme for primary school children. Community Dent Oral Epidemiol. 2004;32:173–82. doi: 10.1111/j.1600-0528.2004.00151.x. [DOI] [PubMed] [Google Scholar]
- 21.Frencken JE, Borsum-Andersson K, Makoni F, Moyana F, Mwashaenyi S, Mudler J. Effectiveness of oral health education programme in primary schools in Zimbabwe after 3.5 years. Community Dent Oral Epidemiol. 2001;29:253–9. doi: 10.1034/j.1600-0528.2001.290403.x. [DOI] [PubMed] [Google Scholar]
- 22.van Palenstein Helderman WH, Munck L, Mushendwa S, Van't Hof MA, Mrema FG. Effect evaluation of oral health education program in primary school in Tanzania. Community Dent Oral Epidemiol. 1997;25:296–300. doi: 10.1111/j.1600-0528.1997.tb00943.x. [DOI] [PubMed] [Google Scholar]
- 23.Shenoy RP, Sequeira PS. Effectiveness of a school dental education program in improving oral health knowledge and oral hygiene practices and status of 12-to 13-year-old school children. Indian J Dent Res. 2010;21:253–9. doi: 10.4103/0970-9290.66652. [DOI] [PubMed] [Google Scholar]
- 24.Petersen PE, Peng B, Tai B, Bian Z, Fan M. Effect of school-based oral health education programme in Wuhan City, Peoples Republic of China. Int Dent J. 2004;54:33–41. doi: 10.1111/j.1875-595x.2004.tb00250.x. [DOI] [PubMed] [Google Scholar]