

Abstract
It is a commonly held perception amongst biomechanists, sports medicine practitioners, baseball coaches and players, that an individual baseball player's style of throwing or pitching influences their performance and susceptibility to injury. With the results of a series of focus groups with baseball managers and pitching coaches in mind, the available scientific literature was reviewed regarding the contribution of individual aspects of pitching and throwing mechanics to potential for injury and performance. After a discussion of the limitations of kinematic and kinetic analyses, the individual aspects of pitching mechanics are discussed under arbitrary headings: Foot position at stride foot contact; Elbow flexion; Arm rotation; Arm horizontal abduction; Arm abduction; Lead knee position; Pelvic orientation; Deceleration-phase related issues; Curveballs; and Teaching throwing mechanics. In general, popular opinion of baseball coaching staff was found to be largely in concordance with the scientific investigations of biomechanists with several notable exceptions. Some difficulties are identified with the practical implementation of analyzing throwing mechanics in the field by pitching coaches, and with some unquantified aspects of scientific analyses.
Key points.
Biomechanical analyses including kinematic and kinetic analyses allow for estimation of pitching performance and potential for injury.
Some difficulties both theoretic and practical exist for the implementation and interpretation of such analyses.
Commonly held opinions of baseball pitching authorities are largely held to concur with biomechanical analyses.
Recommendations can be made regarding appropriate pitching and throwing technique in light of these investigations.
Key words: Baseball, pitching, throwing, injury, analysis, biomechanics
Introduction
Played worldwide for over a century, baseball is a game that involves periods of apparent inactivity punctuated by the highest recorded angular velocities of human movement. Whilst the game is a delicate balance of attack and defense, pitching performance is integral to success on the baseball field. The perceived importance of optimal pitching mechanics is reflected in the presence of pitching coaches at every level of baseball's organization. Despite the emphasis placed on preventive care and the increasing sophistication of medical management injury rates at the highest level of baseball would appear to be rising (Conte, et al., 2001; Hill, 1983). While some authorities have found no link between 'individual pitching traits' and presence of injury (Grana and Rashkin, 1980) many more (Albright et al., 1978; Alexander, 1994; Altchek and Hobbs, 2001; Andrews et al., 1985; Atwater, 1979; Azar, 2003; Burkhart and Morgan, 2001; Dillman et al., 1993; Duda, 1985; Escamilla et al., 2002; Feltner, 1989; Fleisig et al., 1996; Gainor et al., 1980; Lyman et al., 2002; Matsuo et al., 2002; Meister, 2000; Murata, 2001; Nadler, 2004; Pappas et al., 1985b; Sakurai et al., 1993; Tullos and King, 1973; Wilk et al., 2000) believe the mechanics of the throwing motion to be a significant contributor to likelihood of injury. Despite this apparently commonly held perception of a link between throwing mechanics and pitching performance and health, few authors are specific in their recommendations for the throwing athlete. This paper will attempt to describe the available literature regarding pitching and throwing mechanics as they relate to pitching performance and health.
In concert with a literature review a request was made of an internet biomechanics discussion group for any further unpublished or unindexed work with several papers and 'works in progress' arising. As background, many instructional resources were viewed, and focus groups were held with baseball and pitching coaches to identify generally held perceptions of 'correct' and 'incorrect' throwing mechanics, along with their perceptions as to the effects of these on performance and health. The literature search and focus group results displayed a large range of sophistication ranging from single case observations of an individual making a single throw to kinetic comparisons of groups of subjects making groups of throws.
The vast majority of peer-reviewed published research has been conducted into the pitching motion as opposed to throwing in general reflecting in part the perceived importance of pitching to ultimate success in baseball performance. In a study of 3328 throws made by 100 players during 7 collegiate games of baseball where throws were determined 'active' or 'inactive' as to whether the throw was made in an attempt to get a player out or not respectively (Barrett and Burton, 2002). This analysis gave a quantitative breakdown of the distances required of individual fielders, and showed that pitchers were indeed required to make the vast majority of their active throws over the pitching distance (1606 of 1667 throws made), and that throws made by pitchers accounted for more than half of the throws made in the game of baseball. This analysis also gave information regarding the number of throws made and distances for the other fielding positions. A summary of this data is presented in Figures 1 and 2.
Figure 1.
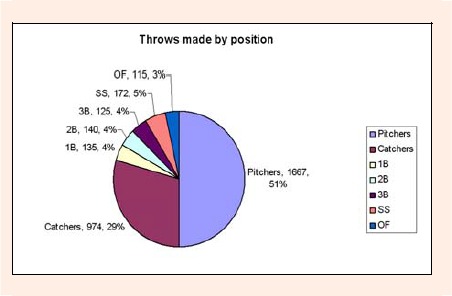
Total number of throws made as described by fielding position from data of Barrett and Burton (Research Quarterly for Exercise and Sport. 73(1), 19-27, 2002). 1B denotes first baseman; 2B': Second baseman; '3B': Third baseman; 'SS': Shortstop; 'OF': Outfielders.
Figure 2.
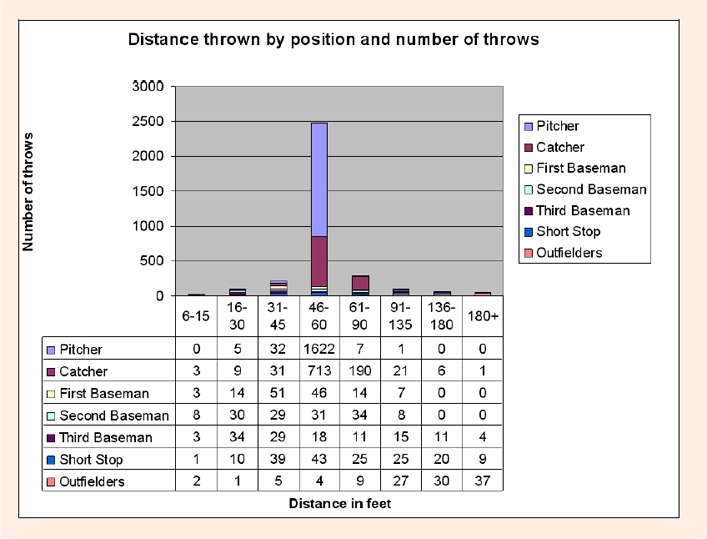
Distance thrown and position of player making the throw for the data described by Barrett and Burton (Research Quarterly for Exercise & Sport. 73(1), 19-27, 2002). Note that the vast majority of throws were made through the distance 46 to 60 feet, and that these throws were made principally by pitchers and catchers. Note also that almost all of the longest throws (180 feet and above) were made by outfielders.)
Whilst some authors have divided the throwing motion into three (Pappas et al., 1985a; 1985b), four (Xue and Masuda, 1997), and five (Andrews and Wilk, 1994; Braatz and Gogia, 1987; Walsh, 1989) stages, more commonly the throwing motion is described as comprising 6 stages (Dillman et al., 1996; 1993; Fleisig and Escamilla, 1996; Werner et al., 1993; Werner et al., 2002, Zheng et al., 1999). These stages are termed: wind-up, stride, arm cocking, arm acceleration, arm deceleration, and follow-through. A representation of these is shown in Figure 3.
Figure 3.
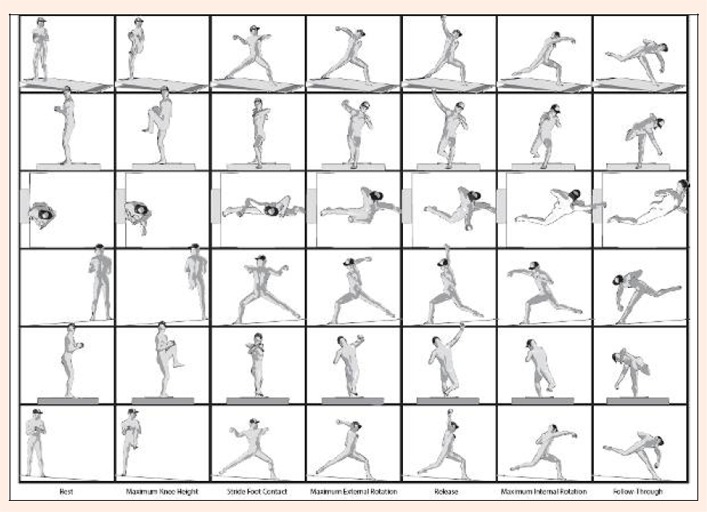
Delineations of the six stages of the pitching motion are displayed here, viewed from six perspectives. The top row shows a perspective view from the third base coaches box, the second row shows a view from home plate, the third row shows a view from above, the fourth row shows a view from the first base side, the fifth row from second base, and the bottom row shows a view from third base. The six stages of the pitching motion are windup, stride, arm cocking, acceleration, arm deceleration, and follow-through. The delineations of these stages are shown here, and are: Rest, maximum knee height, stride foot contact, maximum arm external rotation, release, maximum internal rotation, and follow-through
Limitations of investigations
Along with the perceived importance of pitching in baseball there is a perception of higher incidence of throwing arm injury in pitchers in comparison to other position players (McFarland and Wasik, 1998). Accordingly the majority of investigation into throwing mechanics has been performed on pitchers. Few reports are available comparing pitching to throwing from the field. Norkus, 2000 investigated the 3 dimensional kinematics of throwing sub-maximally over distances of 60, 90, and 120 feet, and throwing maximally over 120 feet. This investigation found very little kinematic similarity in the sub maximal trials and the maximum effort trials with only maximum elbow flexion angle remaining constant across trials. It remains to be shown if there are significant differences between these throwing forms which warrant further clinical investigation.
Several difficulties, theoretical and technological, have been encountered when quantifying the timing and forces involved in pitching. Initially, data for biomechanical models were captured from film at frame rates from 67 frames per second (fps) (Atwater, 1973) to 1500 fps (Atwater, 1979). The use of film analysis proved to be technically demanding requiring a significant delay for chemical development of the film, and therefore delayed identification of any problems with the cinematography. Increasingly high speed videotape analysis has replaced film analysis due to its lower cost, the availability of immediate feedback, the relative ease in synchronization of individual cameras, and the increasing sophistication and ease of computer digitization of the video analysis. The highest recorded angular velocities of any human motion have been displayed during a baseball pitch and this does present some problems for kinematic analysis. For example, during the acceleration phase of throwing, angular velocities in excess of 10,000 °/sec have been recorded (Werner et al., 2001). Standard NTSC videotape captures motion at a rate of 30 frames per second, at such high angular velocities very little information would be gleaned from such an analysis. Even at extremely high videotape rates of capture such as 500 frames per second, the arm would be moving through up to 20° between frames. This apparent limitation was addressed by Fleisig et al., 1996 who captured baseball pitchers performing the pitching motion and American football quarterbacks passing a football at 200 fps. Noting that the only published data available for comparison was captured at 60 fps (Rash and Shapiro, 1995). Fleisig et al., 1996 reanalysed their data for several trials by viewing only every third frame (an effective capture rate of approximately 67 fps) and compared this to their original data captured at 200 fps. They found that there was no difference in any of the parameters measured except for shoulder internal rotation angular velocity - the fastest recorded event. When analyzing the truncated data (using an effective capture rate of 67 fps) the measured angular velocities of arm internal rotation were reduced by approximately 25% in comparison to the original data captured at 200 fps for the same individuals. This difference in calculated velocity (and therefore forces) between the two methods using essentially the same data leads to speculation that different figures may be arrived at for capture rates higher than 200 fps.
Each of the modeling studies presented considers the shoulder to be a single multi-axial joint. This would appear to be at least in part due to the difficulty of obtaining accurate readings for the three dimensional position of the scapula and clavicle. To date, accurate measurement of scapular positioning has involved placement of subcutaneous bone pins into the scapula then recording their position via X-Ray analysis (McClure, et al. 2001). Such a technique whilst affording for accurate measurement of bony position is currently impossible in the context of analysis of maximal effort throwing mechanics. Accordingly, it needs to be remembered that whilst many studies refer to modeling and predicting forces at the 'shoulder', they are referring to the glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic joints as if they comprised a single joint. To date, there is little in the way of published data regarding forces at individual joints during the throwing motion.
Much of the work regarding kinetics during the throwing motion is used to predict potentially injurious behavior. For example, it is shown that during the throw, the amount of shoulder anterior force peaks at approximately 350N (Fleisig, 1994). Selecky et al., 2003 used a force of 10N to 20 N in their measurement of passive translation of the head of the humerus on the glenoid of cadaveric subjects as forces greater than 25N “…often led to marked joint subluxation and dislocation”. It is could be erroneously inferred that the anteriorly directed force during throwing is being borne entirely by the glenohumeral joint, and clinical and surgical decisions (such as the strength required of surgical repair to withstand the rigors of throwing) may be extrapolated from such mistaken assertions.
During motion capture, skin markers are routinely placed over bony prominences, and then the position of these markers is tracked and plotted in three dimensional spaces with an inference that the position of the markers is reflecting the position of the underlying bony prominences. The accuracy of such an inference has been called into question (Karduna et al., 2001). The data captured in these analyses is often used to create an inverse kinetic model from which estimations are then inferred regarding forces and torques at individual joints. Unfortunately, there would appear to be an inherent inaccuracy in these models which, may be by definition unquantifiable. With these limitations in mind, the reader should exercise caution in any interpretation of the results presented. Where available, estimations of the inherent errors are presented, unfortunately such data are not routinely available.
During competitive baseball pitchers are allowed to throw from the 'set' or 'windup' positions as they choose. In the set position, the throwing motion begins with the thrower standing with the ipsilateral (to the throwing arm) foot in contact with the pitching rubber, and striding toward home plate with the contralateral leg. The windup position allows for a short stride backwards or across (with the leg contralateral to the throwing arm) before striding toward home plate. Little work has been done in investigating differences between these two techniques, and it is rarely stated which technique was adopted during analysis of pitching despite a widely held belief that throwing from the windup position confers greater performance. An exception to this was the work of Grove et al., 1988 who documented an increased propensity to throw strikes in a game situation for pitchers choosing the set position (Grove et al., 1988). This group went on to analyze the kinematics of throwing from these two positions finding the set position usually involved a reduction in the amount of thigh rotation, and a more vertically oriented lower leg position. It was also noted that the direction of the stride showed less deviation when throwing a curveball from a set position. These workers suggested that pitchers may benefit by throwing from the set position more often than is usually the case when dictated by game situations (the set position is commonly used only to limit any base-stealing opportunities by the opposition).
This paper assumes knowledge of different pitch types (e.g. “fastball ”and “curveball”) and these will not be described further.
Kinematic factors of throwing related to injury and performance
The review of the literature relating throwing mechanics to health and performance uncovered work in many differing directions. This review is presented arbitrarily in the following order:
-
Mechanical aspects
-
1.1.
Foot position at Stride Foot Contact
-
1.2.
Elbow flexion during throwing
-
1.3.
Arm rotation during throwing
-
1.4.
Arm horizontal abduction during throwing
-
1.5.
Arm abduction during throwing
-
1.6.
Lead knee position during throwing
-
1.7.
Pelvic orientation during throwing
-
1.8.
Deceleration-phase related issues
-
1.1.
Curveballs
Teaching throwing mechanics
Mechanical Aspects
1.1. Foot position at stride foot contact
Fleisig, 1994 performed a kinematic analysis of the pitching technique of 72 baseballers and after consultation with pitching coaches considered eight proposed mechanisms of 'improper mechanics'. By accumulating this data, Fleisig was able to describe average or normative values for each individual parameter. The pitches of individuals were then compared to the accumulated means for each of these parameters, and the kinetics calculated to estimate variations associated with 'improper mechanics' or deviations from these means. Of the originally considered eight proposed mechanical faults, four were found to be associated with increased kinetics at certain phases of the pitching motion, including the positioning of the stride foot.
Fleisig, 1994 documented average stride foot placement to be 87% of body height (measuring estimated centre of the stride ankle joint back to the leading edge of the pitching rubber). This stride was directed toward the plate within 10cm in either direction in comparison to a line drawn from the centre of the trailing ankle to the centre of the home plate. The stride foot was found to be 'closed' or pointing toward the throwing arm side at an angle of 15° ± 10° with reference to this line. (see Figure 4 for an explanation of these terms).
Figure 4.
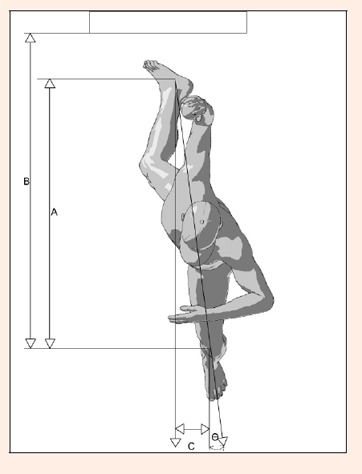
Calculation of stride length, stride offset, and lead foot angle at the moment of stride foot contact. Distance 'A' measures the length from centre of the trailing ankle to the centre of the lead ankle. Distance 'B' measures the distance from the leading edge of the pitching rubber to the centre of the lead ankle. Distance 'C' measures the offset of the centre of the lead ankle from a line drawn from the centre of the trailing ankle through to the centre of the target (home plate). Positive values being on the non-throwing arm, or 'open' side with our example showing a positive value. Angle Theta (Ө) measures the angle made between the long axis of the leading foot and a parallel line drawn from the centre of the trailing ankle to the centre of the pitching rubber. In this case Theta measures approximately 9° toward the 'open' side. Fleisig's (1994) PhD thesis gave normative values for each of these variables as follows: A: 75% of height, ± SD: 4%; B: 87% ± 5%; C: 0.4cm ± 8.3cm; Theta: 15° ± 10°.
Those pitchers who were found to deviate from these norms toward open foot position and alignment showed increased kinetics at the shoulder. For every extra centimeter the stride foot lands toward the 'open' side, an extra 3.0N of maximum shoulder anterior force was found during the arm cocking phase. Further, if the stride leg was placed at an open foot angle, this too increased the maximum shoulder anterior force during the cocking phase at a rate of 2.1N per degree of open foot placement.
To place this data into some context, the maximum shoulder anterior force found during the arm cocking phase was found to be on average 350N, so if a pitcher were to place their lead leg 10cm toward the open side and 10° further open, then this would be associated with a 51N (or approximately 15%) increase in shoulder anterior force during the arm cocking phase. Interestingly, those pitchers who landed in a more 'closed' position (in terms of foot angle, and placement) had no increase in stressful parameters demonstrated.
During the assessment of the injured throwing athlete, a routine finding is reported shoulder pain during the arm cocking phase of throwing (Andrews and Fleisig, 1998; Curtis and Deshmukh, 2003; Meister , 2000). This can be associated with a positive Relocation Sign (Jobe, et al., 1989), and it has been suggested that this is indicative of subtle anterior shoulder instability (Hamner et al., 2000). Matsen amongst others believe that the primary restraints to shoulder subluxation at extreme range of motion to be the ligamentous structures (Matsen et al., 1991). It would follow then that any increase in the amount of shoulder anterior force during the arm cocking phase could be directly associated with pathology at the ligamentous restraints such as increasing anterior shoulder instability.
Montgomery and Knudson, 2002 in an investigation of six professional baseball pitchers found that increasing the stride length to 85-90% of their body height to be associated with an increase in throwing velocity in four of them. Contrary to some pitching instruction, this was generally not associated with throwing the pitch higher in the strike zone as only one of the pitchers showed a weak trend (r = 0.54) towards doing so.
In a kinematic examination of 16 collegiate baseball pitchers throwing a variety of pitch types (fastball, curveball, slider, and changeup) Escamilla et al., 1998 found lead foot position to vary. This group found stride length to be slightly lower than that reported by Fleisig, 1994 at 84% ± 5% for the fastball in comparison to 82% ± 4% for the curveball. This is in distinction to the work of Elliot et al. (1986) who found no significant difference in their group of 8 International level pitchers throwing fastball and curveball pitches (82% ± 2% and 81% ± 6% for the different pitches respectively). Escamilla et al., 1998 also reported on the positioning of the lead foot angle for each of the pitch types. They found that there were significant differences during the fastball and curveball (0cm ± 10cm versus -3cm ± 9cm); and the changeup and curveball pitches (-3cm ± 9cm and -7cm ± 9cm). The position of the lead foot was not significantly different for the slider (0cm ± 9cm). Lead foot angle was not found to be statistically significantly different for any of the trials at -8°±12°, -7°±11°, -14°±14°, - 10°±11 for the fastball, changeup, curveball, and slider respectively.
1.2. Elbow flexion
Fleisig proposed that increased elbow flexion during the arm cocking and acceleration phases would be associated with an increase in kinetics, but his research did not bear out this finding (Fleisig and Escamilla, 1996). It would appear that this proposal is at least in part based on the commonly held belief amongst pitching coaches that “correct ”mechanics are associated with maintaining elbow flexion of less than 90° at the point of stride foot contact (Figure 5). It was indeed illuminating to then see the work of Werner who analyzed the kinetics of forty professional pitchers during Cactus League spring Training of 1998 (Werner et al., 2001; 2002). Werner et al. (2001; 2002) used three 120Hz cameras through at least 2 innings of pitching, choosing the best fastball in terms of '…location, velocity, and outcome' from this sample for analysis with an average displayed ball velocity of 89 mph.
Figure 5.
Depiction of elbow flexion at moment of Stride Foot Contact. Commonly pitching coaches will assert that the elbow shoulder remain at less than 90° of flexion (i.e. “straighter”) during the throw, however the results of several investigations reveal that this may need reappraisal in light of reduced stressful forces at both the shoulder and elbow where a higher amount of elbow flexion is displayed.
In one study Werner used shoulder joint distraction as a dependent variable (Werner et al., 2001) as it is proposed that longitudinal distraction of the glenohumeral joint can be associated with pathology commonly seen in the throwing athlete such as shoulder instability (Altchek and Hobb,s 2001), and traction injuries to the biceps anchor and superior labral complex (Andrews et al., 1985; Andrews et al., 1985). Thirteen kinematic and kinetic variables were chosen as independent variables for a step-wise regression analysis. A combination of five of these parameters explained 72% of the variance in shoulder distraction estimated during the throwing motion. These parameters included elbow flexion at stride foot contact and elbow flexion at ball release. This work infers that those pitchers who have a more flexed elbow at the point of stride foot contact and a more flexed elbow at the point of ball release will have a reduction in the amount of peak longitudinal distraction force at their shoulders during the throwing motion.
In a related study using similar materials and methods, Werner's group (Werner et al., 2002) performed a stepwise regression analysis with elbow valgus as the dependent variable. Excessive elbow joint valgus force during throwing is considered to be the primary cause of Valgus Extension Overload (Andrews, 1985; Andrews et al., 2001; Cain et al., 2003; Wilson et al., 1983) - a spectrum of disorders including (but not limited to) attenuation of the anterior band of the ulnar collateral ligament (UCL) of the elbow, osteochondral damage to the postero medial olecranon fossa, and osteochondral damage to the radio-capitellar joint. Valgus Extension Overload is considered to be the most common elbow injury suffered by skeletally mature throwing athletes (Azar, 2003; Joyce et al., 1995; Pincivero et al., 1994). This study (Werner et al., 2002) found 4 independent variables were able to explain over 97% of the variance in elbow valgus, including elbow flexion at the point of maximum valgus stress. Peak valgus stress at the elbow occurs late in the cocking phase and very early in the acceleration phase of throwing, and those who displayed a greater amount of elbow flexion at this point in the throw were associated with lower amounts of maximum elbow valgus force during the throw (Werner et al., 2002).
Whilst it would appear then that the commonly held pitching coach's maxim that the elbow should be flexed no more than 90° at the point of stride foot contact could bear re-examination, this notion needs to be tempered in light of the findings of Levin et al (Levin et al., 2004). This group investigated the amount of stress placed at the UCL during valgus stress after progressive sectioning of the posterior olecranon. Levin showed significantly more strain occurred in the UCL at 90° than at 70° of elbow flexion (Levin et al., 2004). The highest valgus stresses occur at late cocking and early acceleration phases and perhaps assessment of elbow flexion at this stage of the throw would be more appropriate.
In terms of pitching performance, one variable commonly sought after is higher throwing velocity. Matsuo et al., 2001 examined 12 kinematic and 9 temporal parameters in a group of 127 healthy college and professional pitchers (Matsuo et al., 2001). These players had an average throwing velocity of 36.1 m·s-1 ± 1.9 m·s-1 for the group (80.75 ± 4.2 mph). Matsuo et al. then compared the 12 kinematic and 9 temporal variables for the group who threw more than one standard deviation greater than average (> 38.0 m·s-1, >89 mph) with the group who threw less than one standard deviation slower then the average (< 34.2 m·s-1, <76.5 mph). One of the variables to show a statistically significant difference between these two sub groups was the timing of maximum elbow extension angular velocity during the throw. Matsuo's group considered the throw from stride foot contact until ball release, describing these two points as 0% and 100% of the throwing cycle respectively. Intuitively, one might expect the higher velocity group to display peak elbow extension angular velocity at or very close to the point of ball release. It was indeed surprising then to learn that the high velocity group displayed the peak elbow extension angular velocity to occur at 91.1% ± 1.9% of the throw duration, whilst the slower throwing group displayed this event slightly later at time = 93.0% ± 2.4% (Matsuo et al., 2001). Atwater, 1979 was amongst the first authors to propose a sequential summation of kinetic links as being critical in the production of velocity in the overhead thrower. She describes the sequential nature of the acceleration of body segments moving from the lower limbs through the trunk and then to the arm and hand. This movement pattern typically shows each segment initially lagging behind its preceding segment, and then accelerating to even higher angular speeds whilst the preceding segment lagged behind. This whip-like summation of angular velocities requires extraordinarily precise timing, and the data of Matsuo et al., 2001 would serve to underscore the delicacy of this balance. The throwing motion has been modeled using a double pendulum to estimate optimal conditions for throwing and striking (Alexander, 1991). Perhaps an alternate explanation for the seemingly counter-intuitive finding of peak elbow extension velocity can be found in this model. Whilst complex to describe mathematically, a double pendulum can be constructed simply where two solid struts (such as student's wooden rules) are connected at their end and swung back and forth from one end (Cross, 2004). From this it can be appreciated that maximum linear velocity of the distal end of the distal segment is not necessarily associated with maximal angular velocity of the proximal segment.
Werner correlated elbow joint position and elbow kinetics with an EMG analysis of the biceps brachii, triceps brachii, and anconeus muscles in an investigation of seven healthy college and minor league pitchers using a 2 camera 500 frames per second analysis (Werner et al., 1993). The mean ball velocity for the subjects was 36.4 m·sec-1, and the EMG data was captured using surface electrodes. Werner showed a sequential activity of biceps followed by triceps activity until the moment of maximal shoulder external rotation, and thence activity in the anconeus muscle as the elbow continued flexing during the first half of the acceleration phase (Werner et al., 1993). Active elbow extension is thought to be principally under the control of the triceps musculature, and secondarily by the anconeus muscle (Basmajian and Griffin, 1972). The subsequent rapid elbow extension was not associated with any appreciable increase in activity of either triceps brachii or anconeus. The elbow flexion seen during the acceleration phase was seen to be associated with a concurrent increase in the amount of predicted elbow compressive force which peaked at approximately 780N shortly before ball release (Werner et al., 1993). The rapid elbow extension seen during the throwing motion would therefore appear to be both a combination of active elbow extension, and the mechanical conversion of angular velocity of the more proximal segments (shoulder internal rotation and horizontal adduction) into elbow extension.
In an investigation of the role of the triceps musculature during throwing, Roberts reported on the preliminary work of Dobbins who performed a radial nerve block (thereby rendering the triceps brachii and wrist and finger extensors inactive) and compared the kinematics of the throws performed prior and subsequent (Roberts, 1971). Dobbins found that the timing of the onset of elbow extension was unchanged after the radial nerve block, however prior to extending the elbow 'collapsed' into a maximum elbow flexion of 145° (from the pre-nerve block maximum of 90°). On the sixth throwing trial after the nerve block was performed, the subject was able to throw in excess of 80% of his original velocity despite the absence of active triceps (and wrist extensor) contribution. This work would suggest that part of the role of the triceps musculature is to maintain elbow flexion such that the moment of inertia of the rotating upper arm is maximized (at 90° elbow flexion).
1.3. Arm rotation
Investigations into the timing, magnitude, and duration of arm rotation are shown to be related to performance and kinetics, and are discussed below. It should be recalled that the amount of arm rotation is usually being inferred from the positions of skin markers on the ulna, humerus, and trunk. Commonly this rotation (axial rotation of the humeral component in comparison to the trunk) is termed “shoulder rotation”, however the components of this total arm rotation which occur at the glenohumeral, scapulothoracic, acromioclavicular, and sternoclavicular joints can only be guessed at. Accordingly, for the purposes of this paper, this motion will be termed “arm rotation”.
1.3.1. Early external rotation
In Fleisig's (1994) initial investigation he found the average amount of arm rotation to be 53° ± 26° at the point of stride foot contact (Figure 6). Those who displayed an increase in the amount of arm external rotation at stride foot contact also displayed increased kinetics at the arm and elbow, and alterations in stride foot position.
Figure 6.
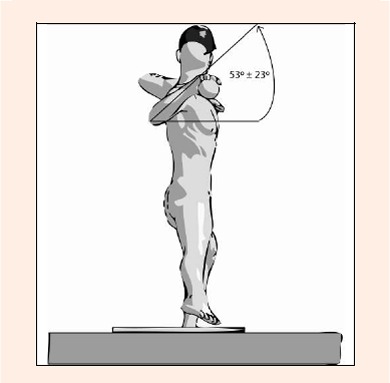
Arm external rotation at Stride Foot Contact. In the investigation of Fleisig (1994) Arm external rotation was found to be 53°±26°. An increase in the amount of displayed external rotation at this point in the throwing cycle is termed “Early External Rotation” and was shown to be associated with increased stressful forces at both the shoulder and elbow, whilst a reduction in external rotation is termed “Late External Rotation” and was shown to be associated with increased stressful forces at the elbow, but a reduction in potentially damaging forces at the elbow.
An increase in the amount of arm rotation was shown to be associated with increased shoulder anterior force during the arm cocking phase at a rate of 1.3N/° of arm rotation. The total shoulder anterior force during the arm cocking phase was 350N, so an increase of say 40° would be associated with an increase of 52N or almost 15%.
Increased arm external rotation at stride foot contact was also shown by Fleisig, 1994 to be associated with an increase in the amount of elbow medial force at a rate of 0.7N/°. Elbow medial force averaged a peak of 280N, so an increase of 40° of arm external rotation at stride foot contact would be associated with 28N, or 10% of the total medial elbow force. The passive restraints against valgus stress at the medial elbow include the UCL, principally its anterior band. During throwing, the load placed through this structure is thought to approach its ultimate tensile strength. Any further increases in the amount of valgus stress through increased arm external rotation at stride foot contact could place this structure at a heightened risk of tensile failure.
Escamilla et al., 2002 evaluated kinetic, kinematic, and temporal values of 11 American and 8 Korean healthy professional pitchers during trials of pitching a fastball including external rotation. In this study, the Korean pitchers displayed reduced kinetics, and approximately a 10% reduction in throwing velocity in comparison to the American pitchers (37.1 ± 1.9 m·sec-1 vs. 34.9 ± 1.0 m·sec-1). In contrast to the findings of Fleisig, 1994, one of the variables associated with reduced kinetics at the shoulder and elbow was an increase in the amount of arm external rotation displayed at lead foot contact.
1.3.2. Late external rotation
A decreased amount of arm external rotation at stride foot contact (beyond one standard deviation from the group mean) was shown by Fleisig, 1994 to be associated with an increase in the maximum longitudinal compressive force along the humerus during the cocking phase at a rate of 1.5 N/°. The average maximum compressive force along the humerus being 590N for the group, an increase of 40° then could be associated with an increase of 60N or over 10% of the total compressive force during the arm cocking phase. It is thought that increases of longitudinal compression during this phase could be associated with compression/rotation injuries to the glenoid labrum, much in the manner of proposed damage to the menisci of the knee during weight-bearing combined with rotation.
A reduction in the amount of arm external rotation at stride foot contact was associated with a reduction is stressful kinetics at the elbow (Fleisig, 1994). It was shown that the elbow medial force (and varus torque) was reduced at a rate of 0.8 N/° (0.2Nm varus torque) (Fleisig, 1994). In our previous example of a 40° reduction in the amount of arm external rotation at stride foot contact, this would be associated with a reduction of 32N (over 10% of the total valgus force).
1.3.3. Total arm external rotation range
Very high figures - up to 210° (Werner et al., 1993) are quoted for the total amount of arm external rotation displayed during throwing (Figure 7). Feltner and Dapena, 1986, and Kreighbaum and Barthels, 1985 hypothesized that the arm external rotation displayed during throwing with simultaneous EMG activity of the horizontal adductors and internal rotators was due to the inertial lag of the forearm as the proximal segments rotated toward the contralateral (to the throwing arm) side. It is not surprising then to learn of that there is no relation between the amount of active external rotation range at the shoulder horizontal abduction and adduction of the active arm external rotation range and throwing skill or speed (Clements et al., 2001). Clinically, a more useful finding is the amount of passive arm external rotation since it more closely reflects the nature of the movement displayed in the throwing motion. Whilst many authors (Baltaci et al., 2001; Bigliani et al., 1997; Brown et al., 1988; Crockett et al., 2002; Ellenbecker et al., 2002; Reagan et al., 2002) have described a difference in the total range of external and internal rotation in the dominant and non dominant arms of high level baseball players, there are occasional exceptions to this finding (Johnson, 1992).
Figure 7.
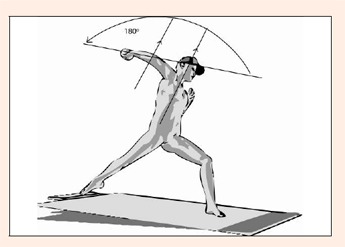
Maximum displayed Arm External Rotation. Maximum displayed figures for arm external rotation during pitching have been recorded in excess of 210°, and routinely are reported in the order of 180°. The clinical assessment of a thrower’s passive rotational range of motion needs to be made with these figures in mind.
The finding that increased range of external rotation is associated with an increase in throwing speed was originally described by Atwater, 1979 who investigated ranges of motion and throwing speed in a group of varsity pitchers. Subsequently Wang et al., 1995 using 2 150Hz cameras examined fastball pitches of 3 pitchers (2 college, 1 high school with an average release velocity of 32.34 m·sec-1 ± 3.63 m·sec-1). This group showed a correlation between the amount of maximum external rotation at the beginning of the acceleration phase and ball release velocity, with the Pearson r value measuring 0.86. This work was further expanded in the investigation of Matsuo who found an increased maximum displayed shoulder external rotation range (from 166.3° ± 9° to 179° ± 7.7°) to be associated with higher throwing velocities in his group of 127 healthy college and professional pitchers (Matsuo et al., 2001).
Baseball players have regularly been shown to have both an increased passive range of external rotation in their dominant arm, and a reduction of passive range toward internal rotation (Donatelli et al., 2000; Ellenbecker et al., 2002). It has been suggested that those in whom the lost range of internal rotation exceeds their gained external rotation are at a greater risk of subsequent shoulder labral injury (Burkhart et al., 2003c) and that remediation (Burkhart et al., 2003b) and prevention (Burkhart et al., 2003b) of this lost range of motion is curative and preventive of these injuries.
During the investigation of Werner et al., 2001, the amount of shoulder distraction at the point of maximum external rotation was found to be proportional to the total external rotation range displayed. Werner's group (2001) investigated the total shoulder distractive force as a dependent variable in their regression analysis as it was thought to relate to the potential for pathology at the rotator cuff and glenoid labrum (Werner et al., 2001). Shoulder distractive forces ranging from 83% to 139% of body weight (108% ± 16%) were found for the group of forty professional pitchers playing in the Cactus League of 1998, which was in line with other reported data (Feltner and Dapena, 1986; Fleisig et al., 1995) regarding the maximum distractive force at the shoulder during throwing. Shoulder joint distraction during the follow-through phase where the biceps is acting forcefully to decelerate the extending elbow has been theoretically implicated as a potential source of traction injury to the biceps anchor at the superior glenoid labrum (Andrews et al., 1985). More recently in a cadaveric study of tension on the proximal long head of biceps at the glenoid labrum, arm external rotation in abduction (in a simulated position of arm cocking) was shown to be associated with markedly higher amounts of strain in the proximal long head of biceps than in any of the other simulated throwing positions (Pradhan et al., 2001).
In the examination of American and Korean pitchers by Escamilla the Korean pitchers were shown to have a reduction in maximum arm external rotational range of motion during arm cocking (180 ± 10° vs. 165 ± 10°), and this was associated with a reduced kinetics at the shoulder and elbow, and reduced ball velocity (Escamilla et al., 2002).
When considering the total amount of arm external rotation, and the contribution of the glenohumeral joint, the amount of individual humeral torsion needs to be factored into the equation. The degree of humeral torsion an individual displays has been shown to be associated with the total range of external rotation as well as the propensity for anterior dislocation (Crockett et al., 2002; Kronberg and Brostrom, 1990; 1991; 1995; Kronberg et al., 1993; 1990; Osbahr et al., 2002; Reagan et al., 2002). Pieper in a study of 51 male National Level Handball players found a variation in the side to side values of humeral torsion when measuring with longitudinal X-Ray analysis (Pieper, 1998). Interestingly of his sample the 13 who were presently complaining of shoulder pain had an average reduction of humeral torsion of 5.4° on their dominant side, whilst the remaining 38 healthy players had an average increase of 14.4° of humeral retrotorsion. Similar conclusions were reached by Osbahr et al., 2002 who used longitudinal X-Ray to find a 10° increase in retroversion of the dominant side humeral head of 19 male college baseball pitchers. This figure concurs with the findings of Crockett who used CT to investigate the humeral torsion and glenoid version in 25 professional baseball pitchers and 25 non-throwing controls (Crockett et al., 2002). This group showed an average increase of 17° in the retrotorsion of the dominant arm's humeral head in the pitchers that was not found in the controls. This increased humeral retroversion was found to be associated with an increase in humeral external rotation when measured at 90° of abduction, and would clearly influence the amount of arm rotation which is occurring at the glenohumeral joint. This work suggests that the increased arm external rotation and concomitant reduction in internal rotation (which has often been ascribed to capsular and muscular adaptive changes) may well be partly bony in origin, and a requisite for healthy performance of the extreme range of external rotation seen in throwing athletes.
1.4. Horizontal abduction and adduction
1.4.1. Horizontal adduction
Published data show the maximum horizontal adduction a pitcher displays to be in the order of 14° ± 7° (Fleisig, 1994). Pitching coaches will often see an excessive amount of arm horizontal adduction as a mechanical fault, sometimes describing this pattern as 'leading with the elbow'. Fleisig, 1994 found the maximum horizontal adduction range displayed to be proportional to the maximum elbow medial force during arm cocking phase at a rate of 2.4 N/°. Since the total amount of elbow medial force during the arm cocking phase was 270N in Fleisig's study, an increase of 7° horizontal adduction would be associated with an 18N or 7% increase in this force.
1.4.2. Horizontal abduction
Escamilla et al's (2002) investigation of differences between a group of American and Korean pitchers showed the higher velocity American pitchers to have an increase in the amount of horizontal abduction at stride foot contact (23 ± 12° vs. 14 ± 9°, Figure 8).
Figure 8.
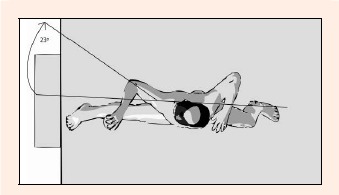
Maximum arm horizontal abduction during pitching.
It has been theorized that an increase in the amount of shoulder horizontal abduction range during the arm cocking phase is associated with a propensity for shoulder pathology. Jobe deemed this to be 'hyperangulation' and thought that it would be coupled with attenuation of the shoulder anterior capsular structures, and therefore anterior shoulder instability (Jobe and Pink, 1996). These workers state that this is seen with a throwing pattern of the hand not being “on top of the ball ”as is thought to be preferred by pitching coaches.
Burkhart's group (2003a) believe that in the presence of a tight and thickened postero-inferior glenohumeral capsule, horizontal abduction combined with external rotation as is shown in the arm cocking phase will be associated with a postero-superior translation of the humeral head relative to the glenoid such that it no longer contacts the posterosuperior glenoid labrum. These researchers feel that the normal contact of the trapped posterosuperior glenoid labrum in this position increases tension in the anterior glenohumeral capsule in a cam like manner, thereby enhancing glenohumeral stability and so the failure of this mechanism during postero-superior translation leads to a failure of the shoulder's normal stability apparatus.
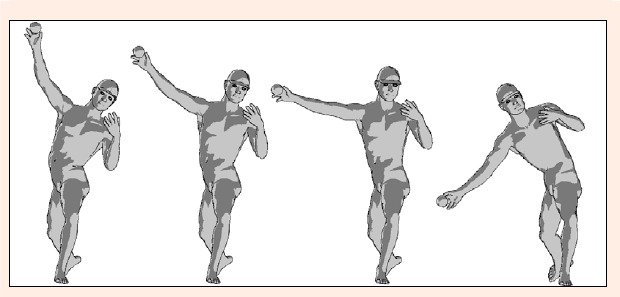
1.4.3. Timing of horizontal abduction and arm external rotation
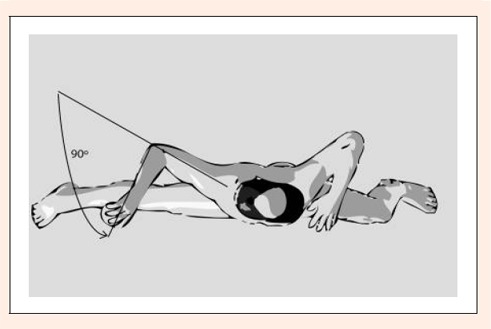
It is seen that during the arm cocking and subsequent acceleration phases, the arm moves from horizontal abduction to adduction and from extremes of external rotation to internal rotation with extremes of external rotation displayed during concomitant shoulder horizontal adduction (Figure 9). Clinically, it is commonly seen that the amount of painless passive external rotation available when measured at 90° of arm abduction will be reduced with increased arm horizontal abduction. Whilst this has not been formally investigated it would seem rational to suggest that shoulder pain would be present in those individuals who aberrantly 'leave' their arm too long in horizontal abduction during the external rotation phase of arm cocking via a similar mechanism perhaps through attenuation of the anterior capsular structures.
Figure 9.
Comparison of glenohumeral external rotation in horizontal abduction and horizontal adduction. The image on the left depicts the proposed effect of performing the shoulder external rotation during the cocking phase whilst the arm is “left” in horizontal abduction of the early cocking phase. The subject on the right would be susceptible to less attenuation of the anterior capsular structures through performing this external rotation in the plane of the scapula, and hence less horizontal abduction coupled with the required glenohumeral external rotation.
1.5. Arm abduction
Atwater was the first to propose that across all the throwing and striking sports, the amount of arm abduction at release/impact stayed relatively constant at 90° with apparent variations being due to trunk inclination (Atwater, 1979). This has only recently been partially challenged by Matsuo who analyzed a group of 2 submarine type pitchers, 2 sidearm type pitchers, and a control group of 13 ¾ arm style pitchers (Matsuo et al., 2000). Matsuo found the submarine style pitchers to abduct their arms to less than 75° during the arm acceleration phase, and that this style of throwing was associated with an increased maximum shoulder anterior force in comparison to the ¾ arm style pitchers (Matsuo et al., 2000). This is a significant finding, as it has been suggested by some pitching coaches that submarine style pitching whilst generally capable of lower velocity than ¾ style pitching, is less stressful on the arms of those performing it, and has been recommended to injured pitchers as a way of extending their careers. The sidearm pitchers were noted to have an increased medial elbow force in comparison to the ¾ arm style pitchers, and this would appear to concur with the majority of opinion of pitching instructors (see Figure 10).
Figure 10.
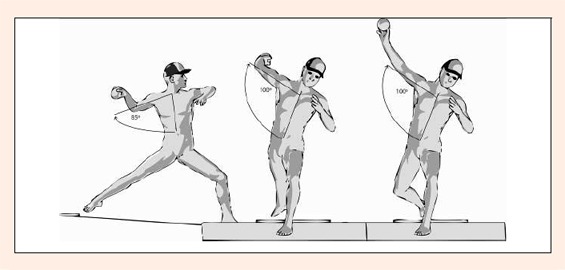
Arm abduction during pitching from the point of Stride foot contact to Maximum External Rotation, and then to release.
Matsuo et al., 1999 modeled the effect of varying the amount of arm abduction at ball release (through the ranges 50° to 130°) during the throw for a number of kinetic and performance variables. This group found that wrist velocity was at a maximum when the shoulder was at 90° abduction at ball release. Elbow varus torque was at a minimum at 80° of arm abduction at release, while peak shoulder anterior force was minimized at 110° arm abduction at release. Shoulder compressive force was at its lowest at 130° arm abduction at release, increasing with all lower values investigated. This work was complemented by a subsequent investigation of eleven professional pitchers by Matsuo et al., 2002 where a two camera videotape analysis was conducted calculating elbow varus torque and peak wrist velocity. Subsequently these values were recalculated with theoretically varied levels of arm abduction. Each pitcher was found to have optimized their level of arm abduction to minimize the amount of elbow varus torque and maximize the peak wrist velocity. More recently, this work was followed up with a 4 camera, 200Hz investigation into 33 healthy college pitchers upon whom a two-way analysis of variance was performed examining the effects of trunk tilt and arm abduction on elbow varus torque through modeling predicted forces across a range of trunk inclination and arm abduction angles (Matsuo et al., 2006). In the simulated overhand and three-quarter arm conditions (see section 7 for and explanation of these terms) elbow varus torque was minimized with arm abduction of 90°, while overall varus torque was minimized at 100° of arm abduction with a contralateral trunk tilt of 10°. During ipsilateral trunk tilt conditions the optimum angle of arm abduction in terms of minimizing elbow varus torque was generally 100° or greater.
Werner's group (2001) found the amount of arm abduction at stride foot contact to be 109° ± 33°, with Flesig's (1994) investigation showing lower values. Fleisig reported arm abduction at ball release to be approximately 95°, and most authors show the arm to slightly abduct from the time of stride foot contact until maximum external rotation, then to slightly adduct until ball release, and then there is a sharp abduction during the decelatory phase until maximum internal rotation of the arm is reached. Increasing the amount of arm abduction was shown by Werner et al., 2002 to be contributory to increasing the amount of valgus stress at the elbow. In contrast to these findings, Escamilla's (2002) investigation of a group of American and Korean pitchers showed the lower velocity (and reduced kinetics) Korean group to have an increase in the amount of arm abduction at stride foot contact (94 ± 11° vs. 104 ± 7°). These findings should be considered in light of Matsuo's (2002) more recent modeling work in which arm abduction angle and trunk inclination were found to be interdependent and analyses examining only one aspect may be therefore be superficially confounding only.
1.6. Lead knee position
At the point of stride foot contact, the lead knee has been reported to be in varying amounts of flexion, and then move toward more flexion, extension, or not at all (Figure 11). In Matsuo's (2001) previously described investigation of a high and low velocity pitching group, the higher velocity group displayed both a slower rate of knee flexion on landing, and a higher rate of subsequent knee extension. Pitching coaches will occasionally describe this behavior as 'firming up the front side', and have been reported as claiming that those throwers who allow their 'front side to soften' (by letting their lead knee move toward more flexion during the acceleration and release phases) are not throwing to their highest potential velocity. In agreement with these findings, Escamilla et al., 2002 showed a reduction in the amount of knee flexion at release (37 ± 14° vs. 48 ± 16°) in the higher velocity group of American pitchers in comparison to their Korean counterparts.
Figure 11.
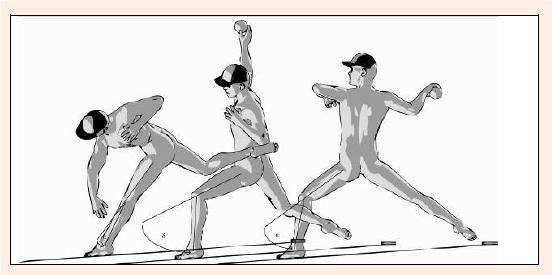
Lead knee position during pitching. Significant variations are seen in the amount of knee flexion from the point of stride foot contact to release and then follow through. The lead knee may increase, decrease, or remain unchanged in terms of flexion. The rate of knee extension has been shown to be associated with an increase in ball velocity (Matsuo et al, 2001).
In an investigation of kinematic differences between pitch types (fastball, curveball, changeup, and slider) thrown by 16 college pitchers, Escamilla et al., 1998) showed the changeup pitch to have the greatest excursion of knee flexion from stride foot contact to ball release, and the lowest ball velocity across all pitch types.
MacWilliams et al., 1998 investigated the ground reaction forces during pitching for one high school and six collegiate pitchers. This group placed a force platform immediately in front of the pitching rubber (underneath the stance leg of the pitcher) and another at the site of stride foot landing. This enabled them to record the magnitude and directions of the 'push off' and 'landing' forces during pitching. They also measured wrist linear velocity (a good correlate of ball speed). They found that ground reaction force directed toward the plate was highly correlated with throwing speed (r2 = 0.82) indicating that those who pushed hardest toward the plate (from their stance leg) and therefore were also able to decelerate most strongly with their landing leg also displayed the highest linear wrist velocities. The results of this study contrast somewhat with the findings of Elliot et al., 1988 who examined 8 International level pitchers whilst throwing fastball and curveball pitches using a force platform analysis of the push-off leg. In the data from the 3 highest velocity pitchers, it was found that the timing of the force pushing toward the plate was later in the pitch cycle but of a similar magnitude to those three who threw slowest.
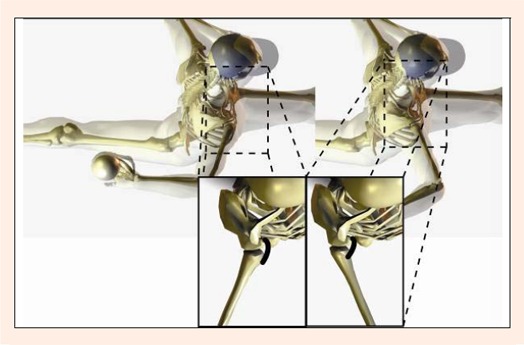
1.7. Pelvic and trunk orientation
Whilst there appear to be no strictly held definitions, it would seem that pitchers are classified in terms of their degree of forearm inclination at release from vertical, and the extent and direction of trunk sideflexion. Those who display significant trunk sideflexion away from the throwing arm side with a concomitant vertically oriented forearm at release will be termed 'Overhand' throwers. If the same pitcher were to have their trunk vertically oriented and the forearm almost horizontal at release then they are termed 'Sidearm' pitchers. The majority of pitchers display mechanics somewhere between these two extremes with a trunk inclined slightly toward the contralateral (to the throwing arm) side and the forearm in between the extremes of vertical and horizontal. This style is termed a 'Three-Quarter arm' throwing. Less commonly, a thrower will inclined their trunk toward the throwing arm side delivering the ball from a lower height. These throwers are termed 'Submarine' style pitchers. (See Figure 12 for an explanation of these terms).
Figure 12.
Depiction of Pitching styles. Pitching style is termed according to the angle of inclination of the trunk and the forearm of the throwing arm. The leftmost image shows a pitcher sideflexing his trunk toward the contralateral (to the throwing arm) side, and an almost vertically placed forearm at release. This throwing style is termed 'overhand'. The third image shows a thrower standing erect with an almost horizontally placed forearm, this is termed 'sidearm' throwing. The second image shows a thrower with only a small amount of contralateral sideflexion and a forearm inclined between the extremes shown in sidearm and overhand throwing, this is termed 'three-quarter' throwing. The right-most image shows a thrower displaying ipsilateral trunk sideflexion, and a lesser amount of arm abduction than the first three images, this is termed 'submarine' throwing.
Matsuo et al., 2000 investigated the kinematics and kinetics of two sidearm and two submarine pitchers. This group found that the sidearm style of throwing was associated with an increase of peak medial elbow force which concurs with the majority of opinion of pitching instruction. Perhaps more surprisingly given the weight of opinion of pitching instructors, the two submarine style throwers were found to show an increase in the maximum amount of shoulder anterior force.
In an effort to determine if variation in trunk sideflexion influences the optimal angle of arm abduction in terms of the sum of minimum torque squared required, Matsuo et al., 2003 using a 4 camera 200Hz analysis investigated the kinematics of seven professional pitchers (throwing with an average velocity of 38.0 ± 1.3 m·sec-1). After determining the kinematics for each of the pitchers, torque squared was recalculated considering variations in trunk tilt angle for seven cases (-20°, -10°, 0°, 10°, 20°, 30°, and 40°) and for 6 different angles of arm abduction at release (70°, 80°, 90°, 100°, 110°, and 120°) giving 42 possible combinations for each individual. For these subjects, Matsuo found that for contralateral trunk tilt (10° to 40° conditions) optimal arm abduction angle varied from 90° to 105° whilst in the ipsilateral conditions, torque squared decreased as arm abduction as shoulder abduction increased, although the optimal abduction angle was not found in the ranges of arm abduction studied (Matsuo et al., 2003). It was concluded that on average ipsilateral trunk tilt was associated with greater requirements of torque squared than for the contralateral conditions, and that the optimal condition (in terms of minimum torque squared) was in the condition of 100° of shoulder abduction and 30° of contralateral trunk tilt. However the authors hastened to point out that two of the seven subjects did not fit this pattern in that altering their kinematics toward this condition increased their torque squared, suggesting that other factors (they put forward trunk inclination and elbow extension angular velocity as possible candidates) may be significant contributors. A subsequent investigation (Matsuo et al., 2006) using similar methodology and 33 college pitchers (average ball release velocity 36.8 ± 0.9 m·sec-1) which again modeled varied kinematics across the same combinations of 42 variables and compared varus torque as a dependent variable showed similar results in that peak elbow varus torque varied according to both arm abduction and trunk inclination angles. In this investigation, peak elbow varus torque generally displayed a minimum shifted toward greater arm abduction angles as trunk tilt angle increased ipsilaterally. Again, there were individual differences between subjects however this data showed a shoulder abduction angle minimizing elbow varus torque depending on the trunk tilt angle with minimum varus torque at approximately 90° of arm abduction in the cases of contralateral trunk tilt in the order of 20° to 30° - the trunk inclination generally described as overhand and three-quarter pitchers, and in accordance with the general teaching of pitching coaches.
In an EMG investigation into muscular activity during throwing, Hirashima et al., 2002 showed activity of the external oblique muscle contralateral to the throwing arm prior to the ipsilateral external oblique. This pattern of muscle activity during the axial rotation phase of trunk movement is thought to be best disposed to assist in the transfer of torque from the lower limb to the upper limb. Activity in the rectus abdominus was only seen immediately prior to release suggesting active trunk flexion activity occurred quite late in the propulsive phase. In their investigation of 127 college and professional pitchers, Matsuo et al., 2001 looked at kinematic differences between the groups which threw at 1 standard deviation above and below the sample mean. Among their results was the finding that higher velocity throwers tended to display an increased forward trunk tilt at the moment of ball release. As rectus abdominus is considered to be a primary trunk flexor, it would appear that this EMG activity seen by Hirashima et al., 2002 late in the throwing cycle is significant in the generation of ball speed.
Stodden et al., 2001 investigated aspects of trunk and pelvic positioning in the horizontal plane during pitching for a group of 19 elite level subjects (7 professional, 9 college, 3 high school). Each of the participants displayed a variation of at least 1.8 m/sec (approximately 4.0 mph) in their trial of 10 maximal effort fastball pitches averaging 35 ± 2 m·sec-1 (78.3 ± 4.5 mph). The variables studied were pelvic orientation and upper torso orientation (in the horizontal plane) at maximum knee height; stride foot contact; instant of maximal arm external rotation; and at the instant of ball release. They also considered pelvic and upper torso angular velocity (in the horizontal plane) during the arm cocking and arm acceleration phases. This data was then analyzed using a mixed model analysis including all 12 pelvis and trunk related variables, of which 5 were found to be associated with variations in velocity. Principal findings were that during the higher velocity trials, subjects displayed a more 'open' pelvis and upper torso at the point of maximum arm external rotation, and a more open pelvis at the point of ball release. It was also shown that the higher velocity throws were made with higher pelvic angular velocities during the arm cocking phase and higher upper torso angular velocities during the arm acceleration phase. Whilst this work was limited to the horizontal plane, Matsuo et al., 2001 in their investigation of pitchers throwing more than one standard deviation above and below the mean velocity of the group of 127 pitchers considered variables in the horizontal and sagittal planes. Matsuo et al., 2001 investigated maximum pelvis linear velocity, maximum pelvis and upper trunk angular velocity (in the horizontal plane), trunk forward tilt angular velocity, and forward tilt at the instant of ball release. With the exception of linear pelvic velocity, these entire trunk related variables were of higher magnitude in the high velocity group. However, only forward trunk tilt at the instant of ball release (36.7° ± 6.7° in contrast to 28.6° ± 11.1°) reached statistical significance.
In accordance with these findings, Escamilla et al., 2002 in their investigation of a group of American and Korean pitchers, showed the higher velocity American group to have a higher pelvic angular velocity during arm cocking (660 ± 60°/s vs. 610 ± 55°/s), and an increase in forward trunk tilt at ball release (32 ± 8° vs. 26 ± 9°).
In a 2001 investigation into 9 pitchers separated into low and high skill level by an experienced coach, Murata, 2001 looked at the amount of non-throwing shoulder movement. Using a two camera, 200Hz analysis, a marker was placed over the acromion process of the non-throwing arm, and its three dimensional motion recorded from stride foot contact until ball release and normalized as a function of body height. The skilled group of four pitchers threw their fastballs at 38.22 ± 1.02 m·sec-1 in comparison to the less skilled group who threw at 35.96 ± 1.45 m·sec-1. The skilled group of throwers were found to have a reduction in the amount of non-throwing shoulder movement in all directions for both fastball and curveball trials during the period from stride foot contact until ball release. A reduction in the amount of x-axis movement was strongly associated with an increase in fastball velocity, and perceived skill level. These findings concur with the observations of Feltner, 1989 who suggested that the rotation around a relatively stationary non-throwing shoulder would give rise to higher trunk rotation torques and therefore higher throwing velocity.
Aguinaldo et al., 2003 in a preliminary investigation looked at the timing of pelvic and trunk rotation in a group of 37 pitchers (5 professional, 11 collegiate, 12 high school, and 9 youth level). For the purposes of the study, the pitch cycle was normalized to Stride Foot Contact = 0%, and Ball Release = 100%. Professional pitchers were found to begin their trunk rotation significantly later in the pitch cycle (34% ± 5%) in comparison to the rest of the groups. Differences were also seen in the peak internal rotation torques seen, with the youth level pitchers displaying the lowest values, followed by the professional pitchers, then the high school pitchers, and highest of all the college pitchers. It was speculated by the authors that the youth level pitchers had the lowest internal rotation torques given their relative skeletal immaturity, whilst the college and high school pitchers were speculated to have higher internal rotation torques to compensate for their earlier onset of trunk rotation.
Shimada et al., 2000 using a two camera 200Hz analysis complemented with two force platforms sampling at 250Hz (one at the stance foot, and one under the landing foot) investigated the contributions of the trunk and lower limbs to pitched ball velocity. These workers calculated joint torques, joint torque powers, and work done by the torso, hip, knee, and ankle joints for 10 pitchers. This group found no relation between work done by the torso and hip joints and pitched ball velocity.
Watkins et al., 1989 in an EMG investigation of the trunk muscle activity of 15 professional baseball pitchers showed the activation patterns to be quite similar across each of the individual trials, and have documented the firing pattern of muscle activity for this group.
1.8. Deceleration
Once the ball has left contact with the throwing arm, no further action by the pitcher can alter the ball's course. Any alteration in mechanics of follow-through therefore, can only be directed toward the health of the pitcher. The force required to decelerate the throwing arm is directly proportional to the ball speed (Fleisig, 1994). An increase duration of the follow-through phase will result in a reduction in the force required while maintaining the same impulse (by virtue of an increase in the time that force is applied) and is recommended by most pitching authorities. Some of the force required to decelerate the rapidly internally rotating shoulder may be provided by the posterior inferior glenohumeral ligament. It has been suggested that repeated traction to this structure results in an adaptive shortening and thickening which subsequently alters the centering of the humeral head during the arm cocking phase of throwing (Burkhart et al., 2003a). These authors believe that this alteration is critical in the formation of superior labral tears of the glenoid associated with undersurface fraying of the postero-superior cuff (Burkhart et al., 2003a). The ossification seen at the postero-inferior glenoid originally described by Bennett could be explained in terms of maladaptation to the repeated tensile overload in this region (Bennett, 1941), and may explain its presence in 25% of asymptomatic pitchers in Connor's investigation (Connor et al., 2003).
To reduce the peak forces required in deceleration of the throwing arm, attention can be paid to all aspects of the kinetic link, not just the throwing arm. Tempering this desire for an extended follow-through is the practical matter of fielding a batted ball: if the pitcher has made such an elaborate follow-through maneuver as to render him unable to field a ball batted back in his general direction, then his effectiveness will be diminished and his personal safety may be at risk.
2. Curveballs
In the only published investigation of ball spin, the standard fastball pitch has been described to impart an underspin on the ball at a rate of 29.9 revolutions per second; whilst the curveball has a similar rotational velocity (26.6 revolutions per second) its direction is almost exactly opposite to that of a fastball, causing an alteration in the flight path of the ball such that the downward and sideways movement is exaggerated (Escamilla et al., 1998).
Coaches regularly relate the supposed increased stresses associated with throwing curveballs, and recommendations have been made to limit the throwing of curveballs by skeletally immature athletes (Andrews et al., 1999; Jobe and Nuber, 1986). Lyman investigated a group of 476 pitchers aged 9 to 14 for a single season (Lyman et al., 2002). This group questioned the participants regarding the total number of pitches thrown in given games, and throughout the season; the kinds of pitches thrown; and the presence of pain or discomfort during or after play. They also performed a videotape analysis of 240 of the pitchers prior to the season documenting 24 parameters as 'proper, insufficient, or excessive.' The study concluded that throwing curveballs and sliders were associated with a higher risk of shoulder and elbow pain respectively. The group was unable to associate any of the supposed incorrect pitching mechanics with pain. The findings of this investigation need to be considered in light of the work of Olsen et al., 2006 who compared 95 adolescent pitchers who had shoulder or elbow surgery with a group of 45 adolescent baseball pitchers who had not complained of any shoulder or elbow pain. This work found no effect of either frequency of pitch type, nor age at which certain pitch types were thrown to be related to injury occurrence. Rather the greatest indicators of injury incidence were pitching frequency, pitching with pain, and pitching with fatigue (Olsen et al., 2006).
The spin imparted on the ball will depend on the motion path taken by the hand and fingers, and the release pattern of the fingers on the ball. Tarbell, 1971 using a film capture rate of 1500 frames per second examined one fastball pitch and found that the thumb was the first digit to leave the ball but was unable to elucidate whether the index or middle fingers left next. Ketlinski, 1971 examined one curveball pitch using a capture rate of 1000 frames per second and found a finger release pattern of thumb followed by middle finger followed by index finger for the curveball pitch. Stevenson, 1985 investigated the finger release patterns of 9 collegiate baseball pitchers for 103 fastballs and 88 curveballs. Using 1000 frames per second cinematographic analysis, these throwers were found to have an average release velocity of 31.8 meters per second for the fastball trials and 25.5 m·sec-1. for the curveballs. Stevenson, 1985 found the finger release patterns to vary between and within pitchers. For all fastball trials the thumb was found to leave the ball first in 97.1% of cases [at 6.18 msec prior to release (SEM: 0. 37, SD: 3.72)], followed by the middle and index fingers which left almost simultaneously [at 0.28 (SEM: 0.06, SD: 0.13 msec) and 0.52 (SEM: 0.13, SD: 1.20 msec prior to release)]. During the curveball trial, only one pitcher of the nine demonstrated the finger release pattern documented by Ketlinski, 1971. Seventy-five percent of the curveball pitches were thrown with a release pattern of thumb-middle- index, whilst 25% were thrown with a pattern of middle-thumb-index (Ketlinski, 1971). The curveball trials showed five of the 9 pitchers to reliably have a release sequence of thumb, then middle, then index fingers whilst the remaining four pitchers showed a pattern of thumb and middle fingers off almost simultaneously then index finger. The group data for the curveball trials was thumb released at 6.41 (SEM: 0.63, SD: 5.86 msec prior); Index finger at 0.02 (SEM: 0.05, SD: 0. 11) and middle finger 2.48 (SEM: 0.16, SD: 1.48)
Several groups of authors have investigated kinematic differences between the fastball and off speed pitches. Elliot et al. (1986) were the first to investigate this matter in their study of 6 national level Australian pitchers using 2 cameras recording at 200 frames per second and one at 300 frames per second. Whilst they found that the fastball and curveball pitches were quite similar in many respects, there were differences in stride length, and forearm and wrist position at release. Specifically, in the curveball group, stride length was shown to be slightly shorter (81.4 ± 6% compared with 82.3 ± 2. 3% of body height), and the curveball was associated with a slightly more open lead foot position (8. 4 cm compared with 7.0 cm for the fastball). The most striking differences occurred just prior to release with the forearm placed in more supination “such that the palm of the hand almost faces the head ”and the wrist was more flexed (188° compared with 178° for the fastball.) Higher angular velocities for the wrist joint (332.3 °/sec compared with 177.6 °/sec) and elbow joint (986 °/sec and 969 °/sec) were seen just prior to release with the curveball indicating higher contributions of the wrist and hand to the total velocity (31.8% for the curveball compared with 26. 5% for the fastball). In 1993, Sakurai et al., 1993 published their findings of a kinematic analysis of 6 Japanese University pitchers throwing fastball and curveball pitches. In this analysis small sticks were placed on the wrist and hand and two cameras capturing data at 200 frames per second were used. This group found no differences between the pitch types for shoulder and elbow temporal sequences, but confirmed the findings of Elliot et al. (1986) of increased radioulnar supination and dorsiflexion immediately prior to release.
This kinematic data was furthered with the work of Escamilla et al., 1998 who investigated 16 college pitchers throwing fastball, curveball, changeup, and slider pitches. For this group, Escamilla et al., 1998 examined 26 kinematic variables across each of the pitch types. In summary, the greatest differences were shown between the fastball and changeup groups (with 14 of the 26 parameters showing significant differences) whilst the fastball and slider groups showed the least differences (only 2 of 26 parameters). In contrast to the findings of Elliot etal. (1986) this group found that during the arm cocking and acceleration phases, the peak values for arm internal rotation and elbow extension (along with trunk rotation) were higher in the fastball and slider groups, lower in the curveball, and lowest in the changeup group. At ball release, the curveball group was found to have the greatest trunk lateral tilt of the pitch types.
Using accelerometers mounted to the forearm, Saitou et al., 2000 examined the pronation/supination movements of 5 college baseball pitchers confirming the finding of the movement of pronation before and after release in both curveball and fastball pitch types, with no difference in peak angular velocity between pitch types, although the peak velocity occurred closer to ball release in the fastball.
Escamilla et al., 1998 have published the only kinetic data regarding differences between throwing fastballs and off-speed pitches. In their preliminary examination of 18 healthy college pitchers who threw fastballs, changeups, curveballs, and sliders, they found statistically significant increases in medial elbow force and elbow varus torque when throwing curveballs. Conversely, the changeup consistently showed the lowest segmental angular speeds and forces at the shoulder and elbow.
It had been suggested that the increase in medial elbow problems with throwing curveballs was due to an increase in the activity of the flexor pronator muscle mass which takes a common origin at the medial epicondyle (Atwater, 1979). This would appear unlikely given the findings of Sisto et al., 1987 who investigated eight collegiate pitchers with dynamic EMG of muscles of the forearm whilst throwing fastball and curveball pitches. No statistically significant differences were found for any muscle groups for either pitch, with only slight increases in activity of the Extensor Carpi Radialis Longus and Brevis muscles during late cocking, acceleration, and follow-through of the curve ball as compared to the fast ball. Saitou et al., 2001 have revisited this notion and found an increase of activity in the Pronator Teres muscle whilst throwing a fastball in comparison to the curveball. Interestingly, Pomianowski et al., 2001 in a cadaveric investigation of failure loads of the ulnar collateral ligament have shown that the elbow's resistance to valgus stress is rotation dependent, with increasing stiffness in supination as opposed to pronation. Given the finding that curveballs appear to be associated with release in a position of increased forearm supination (Elliott et al., 1986; Saitou et al., 2000; Sakurai et al., 1993) and that the highest valgus torques are present at the late cocking phase of throwing, it would seem reasonable to suggest that throwers endeavor to maintain a supinated forearm throughout the early portion of the acceleration phase in an effort to minimize the any potentially deleterious effects of valgus overload stress at the medial elbow.
3. Teaching Throwing Mechanics
Long-standing motor patterns can be difficult to alter. If aberrant mechanics can be related to pathologic forces and diminished performance, then it stands to reason that more correct mechanics would be best taught early in a thrower's career. In the only paper documenting kinematics kinetics across varying ages, Fleisig investigated 17 kinematic and 8 kinetic parameters in a group of 231 pitchers (Fleisig et al., 1999). The group was subdivided into 4 groups based on their age: 23 youth (age range: 10-15 years); 33 high school (15-20 years); 115 college (17-23 years); and 60 professional (20-29 years) level athletes. This investigation showed each of the 4 velocity parameters to vary across the groups, but differences in only one of the positional parameters and no temporal differences were displayed in the 6 items examined. Each of the 8 kinetic variables increased with increasing age group which was thought to represent the increased force generating potential of the increasingly skeletally mature subjects. Since there were few differences in positional and temporal parameters across this large sample of subjects representing most aspects of throwing ages, it is reasonable to suggest that teaching correct mechanics can be performed from the earliest participation in the sport.
In light of the relatively high incidence of injury in the throwing athlete in general (McFarland and Wasik, 1998) and the skeletally immature athlete in particular (Gugenheim et al., 1976; Larson et al., 1976) it has been recommended that younger athletes limit their exposure to throwing (Olsen et al., 2006; Sabick et al., 2004). Recommendations have been made in terms of total numbers of pitches to be made in any individual outing (Lyman et al., 2001) and for the entire season (Lyman et al., 2002). It has also been recommended that since increased forces at the shoulder and elbow are shown during throwing the curveball and slider that these pitches should be discouraged until skeletal maturity and discarded in preference for the fastball and circle change-up (Andrews et al., 1999; Nelson, 2001).
By and large, throwing mechanics is taught by pitching coaches whose principal tool is visual inspection of 'live' performance, and increasingly videotaped analysis of recent performance. It is pertinent to note that the reliability of such analysis has been called into question in the only investigation performed thus far. Fleisig et al., 1999 developed a checklist of key throwing parameters which was subsequently investigated by Nicholls et al., 2003 in a study of twenty male youth pitchers (mean age of 12.86 ± 1.29 years). This group were filmed outdoors using a standard video camera placed at three positions to best view each of the identified parameters, and then scored on a checklist to rate if the items were deemed to be 'proper' (acceptable), 'excessive' (high), or inadequate (low) by two raters. The results of this were then compared with a 6 camera, 240Hz laboratory investigation into the same 20 pitchers to estimate the agreement between the two methods. Unfortunately, only four of the 24 kinematic variables showed agreement between the two methods, and inter-rater reliability showed agreement on only 33% of the variables viewed by the two raters. Accordingly, standard videotape analysis can only be viewed (at best) as preliminary data in the investigation of throwing mechanics, and at worst routinely misleading. Nicholls et al., 2003 identified poor lighting and subsequently large shutter speeds (entailing a large degree of motion blur) as a potential confounding factor in their analysis (Nicholls, et al. 2003).
Occasionally scholarly works will discuss the perceived throwing mechanics of an individual, inferring a potential for injury. For example, the following two images are taken from the paper of Burkhart et al., 2003b where they state that the pitcher in the first image displays: 'abduction in extension, with angulation of the arm posterior to the plane of the scapula rather than in the plane of the scapula. Note the “dropped elbow ”in this pitcher, causing the arm-body angle to drop below the horizontal.' Whilst the text accompanying the second image claims: 'Ideal mechanics involve abduction in the plane of the scapula (A, dotted line) with the elbow high enough to keep the upper arm at or above the horizontal plane. (B) With a “dropped elbow ”(solid line), the upper arm hyperangulates posterior to the plane of the scapula. (C) This pitcher has excellent mechanics, with the arm abducted in the plane of the scapula and positioned above the horizontal plane (Figure 13).'
Figure 13.
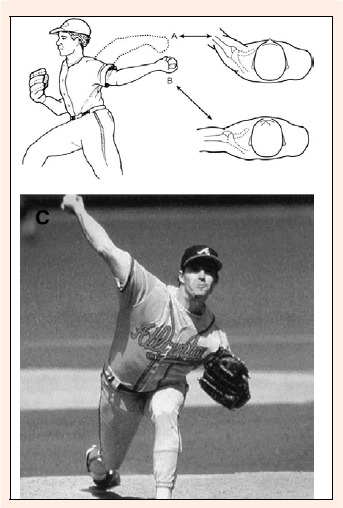
Image taken from Burkhart, S.S., Morgan C.D. and Kibler, W.B. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 19(6), 649, 2003. The original caption to the image reads: 'Ideal mechanics involve abduction in the plane of the scapula (A, dotted line) with the elbow high enough to keep the upper arm at or above the horizontal plane. (B) With a “dropped elbow ”(solid line), the upper arm hyperangulates posterior to the plane of the scapula. (C) This pitcher has excellent mechanics, with the arm abducted in the plane of the scapula and positioned above the horizontal plane.' Note that this image shows an overhand thrower at or close to maximum external rotation of the arm.
It is interesting to note then that the first image (Figure 13) is taken of a pitcher in the early phase of arm cocking whilst the second image (Figure 14) is of a pitcher close to release. As is evidenced from many investigations into throwing mechanics, the amount of arm horizontal abduction, and arm abduction varies substantially between these two points. One can only guess that the assumed poor mechanics are related to the first thrower's more vertically oriented trunk position, and therefore since his contralateral shoulder is higher, giving the illusion of having his throwing arm abducted less.
Figure 14.
Image taken from Burkhart, S.S., Morgan, C.D. and Kibler, W.B. The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 19(6), 650, 2003. The original caption reads: 'This pitcher has excellent mechanics, with the arm abducted in the plane of the scapula and positioned above the horizontal plane. This pitcher shows abduction in extension, with angulation of the arm posterior to the plane of the scapula rather than in the plane of the scapula. Note the “dropped elbow ”in this pitcher, causing the arm-body angle to drop below the horizontal.' Note that this image shows a pitcher soon after stride foot contact, and before arm cocking has been undertaken to any great extent. Therefore it is not an unusual finding to have a reduced amount of arm abduction, and an increased amount of arm horizontal abduction at this point in the throwing cycle.
Conclusion
While this review of the available literature regarding pitching and throwing of baseballs and their relation to performance and health has shown some diversity of opinion in several areas, and some technical difficulties still render some of the findings as preliminary, much can be gleaned for the coach, athlete, and treating physician from this work. In order to maximize performance and maintain health, ongoing research is needed to further refine these areas of investigation in particular to investigate the interaction of varying more than one of the kinematic variables discussed.
Biography
Rod Whiteley
Employment
Sports Physiotherapist in private practice who is currently undertaking a PhD by research in physiotherapy at the Univer-sity of Sydney, Australia.
Degree
MSc
Research interests
Baseball stems from an ongoing involvement in all aspects of the game.
E-mail: whiteley.rod@gmail.com
References
- Aguinaldo A., Buttermore J., Chanmbers H. (2003) Sequential body motion and shoulder joint torque between baseball pitchers of various levels. Available from URL: http://www.sandiegogaitlab.com/chp/pitching_abstract03.pdf [DOI] [PubMed]
- Albright J.A., Jokl P., Shaw R., Albright J.P. (1978) Clinical study of baseball pitchers: correlation of injury to the throwing arm with method of delivery. American journal of sports medicine 6, 15-21 [DOI] [PubMed] [Google Scholar]
- Alexander M.J.L. (1994) Overhand throwing mechanics and injuries. Critical Reviews in Physical & Rehabilitation Medicine. 6, 291-315 [Google Scholar]
- Alexander R.M. (1991) Optimum timing of muscle activation for simple models of throwing. Journal of Theoretical Biology, 150, 349-372 [DOI] [PubMed] [Google Scholar]
- Altchek D.W., Hobbs W.R. (2001) Evaluation and management of shoulder instability in the elite overhead thrower. Orthopedic Clinics of North America 32, 423-430 [DOI] [PubMed] [Google Scholar]
- Andrews J.R. (1985) Bony injuries about the elbow in the throwing athlete. Instructional Course Lectures 34, 323-331 [PubMed] [Google Scholar]
- Andrews J.R., Broussard T.S., Carson W.G. (1985) Arthroscopy of the shoulder in the management of partial tears of the rotator cuff: a preliminary report. Arthroscopy 1, 117-122 [DOI] [PubMed] [Google Scholar]
- Andrews J.R., Carson E.G., McLeod W.D. (1985) Glenoid labrum tears related to the long head of the biceps. American journal of sports medicine 13, 337-341 [DOI] [PubMed] [Google Scholar]
- Andrews J.R., Fleisig G.S. (1998) Preventing throwing injuries. Journal of Orthopaedic & Sports Physical Therapy 27, 187-188 [DOI] [PubMed] [Google Scholar]
- Andrews J.R., Fleisig G.S., Whiteside J.A. (1999) Little Leaguer's Elbow: evalution, treatment and prevention Sports Medicine Update 14, 11-15 [Google Scholar]
- Andrews J.R., Heggland E.J., Fleisig G.S., Zheng N. (2001) Relationship of ulnar collateral ligament strain to amount of medial olecranon osteotomy. American Journal of Sports Medicine 29, 716-721 [DOI] [PubMed] [Google Scholar]
- Andrews J.R., Wilk K.E. (1994) The athlete's shoulder. Churchill Livingstone, New York [Google Scholar]
- Atwater A.E. (1979) Biomechanics of overarm throwing movements and of throwing injuries. Exercise & Sport Sciences Reviews 7, 43-85 [PubMed] [Google Scholar]
- Atwater A.E. (1973) Cinematographic analysis of human movement. Exercise & Sport Sciences Reviews 1, 217-258 [PubMed] [Google Scholar]
- Azar F.M. (2003) History and examination of the thrower's elbow Sports Medicine and ArthroscopyRreview 11, 10-14 [Google Scholar]
- Baltaci G., Johnson R., Kohl H., 3rd (2001) Shoulder range of motion characteristics in collegiate baseball players. Journal of Sports Medicine & Physical Fitness 41, 236-242 [PubMed] [Google Scholar]
- Barrett D.D., Burton A.W. (2002) Throwing patterns used by collegiate baseball players in actual games. Research Quarterly for Exercise and Sport, 73, 19-27 [DOI] [PubMed] [Google Scholar]
- Basmajian J.V., Griffin W.R.Jr. (1972) Function of anconeus muscle. An electromyographic study. Journal of Bone and Joint Surgery, 54, 1712-1714 [PubMed] [Google Scholar]
- Bennett G. (1941) Shoulder and elbow lesions of the professional baseball pitcher. Journal of the Americal Medical Association 117, 510-514 [Google Scholar]
- Bigliani L.U., Codd T.P., Connor P.M., Levine W.N., Littlefield M.A., Hershon S.J. (1997) Shoulder motion and laxity in the professional baseball player. American Journal of Sports Medicine 25, 609-613 [DOI] [PubMed] [Google Scholar]
- Braatz J.H., Gogia P.P. (1987) The mechanics of pitching. Journal of Orthopaedic and Sports Physical Therapy 9, 56-69 [DOI] [PubMed] [Google Scholar]
- Brown L.P., Niehues S.L., Harrah A., Yavorsky P., Hirshman H.P. (1988) Upper extremity range of motion and isokinetic strength of the internal and external shoulder rotators in major league baseball players. American Journal of Sports Medicine 16, 577-585 [DOI] [PubMed] [Google Scholar]
- Burkhart S.S., Morgan C. (2001) SLAP lesions in the overhead athlete. Orthopedic Clinics of North America 32, 431-441 [DOI] [PubMed] [Google Scholar]
- Burkhart S.S., Morgan C.D., Kibler W.B. (2003a) The disabled throwing shoulder: spectrum of pathology. Part I: Pathoanatomy and biomechanics. Arthroscopy 19, 404-420 [DOI] [PubMed] [Google Scholar]
- Burkhart S.S., Morgan C.D., Kibler W.B. (2003b) The disabled throwing shoulder: spectrum of pathology Part III: The SICK scapula, scapular dyskinesis, the kinetic chain, and rehabilitation. Arthroscopy 19, 641-661 [DOI] [PubMed] [Google Scholar]
- Burkhart S.S., Morgan C.D., Kibler W.B. (2003c) The disabled throwing shoulder: spectrum of pathology. Part II: evaluation and treatment of SLAP lesions in throwers. Arthroscopy 19, 531-539 [DOI] [PubMed] [Google Scholar]
- Cain E.L., Jr., Dugas J.R., Wolf R.S., Andrews J.R. (2003) Elbow injuries in throwing athletes: a current concepts review. American Journal of Sports Medicine 31, 621-635 [DOI] [PubMed] [Google Scholar]
- Clements A.S., Ginn K.A., Henley E.C. (2001) Comparison of upper limb musculoskeletal function and throwing performance in adolescent baseball players and matched controls. Physical Therapy in Sport Journal 2, 4-14 [Google Scholar]
- Connor P.M., Banks D.M., Tyson A.B., Coumas J.S., D'Alessandro D.F. (2003) Magnetic resonance imaging of the asymptomatic shoulder of overhead athletes: a 5-year follow-up study. American Journal of Sports Medicine 31, 724-727 [DOI] [PubMed] [Google Scholar]
- Conte S., Requa R.K., Garrick J.G. (2001) Disability days in major league baseball [see comment]. American Journal of Sports Medicine 29, 431-436 [DOI] [PubMed] [Google Scholar]
- Crockett H.C., Gross L.B., Wilk K.E., Schwartz M.L., Reed J., O'Mara J., Reilly M.T., Dugas J.R., Meister K., Lyman S., Andrews J.R. (2002) Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. American Journal of Sports Medicine 30, 20-26 [DOI] [PubMed] [Google Scholar]
- Cross R. (2004) Physics of overarm throwing. American Journal of Physics 72, 305-312 [Google Scholar]
- Curtis A.S., Deshmukh R. (2003) Throwing injuries: Diagnosis and treatment. Arthroscopy 19(Suppl 1), 80-85 [DOI] [PubMed] [Google Scholar]
- Dillman C.J., Fleisig G., Andrews J. (1996) Mechanics of throwing. Churchill Livingstone, New York [Google Scholar]
- Dillman C.J., Fleisig G.S., Andrews J.R. (1993) Biomechanics of pitching with emphasis upon shoulder kinematics. Journal of Orthopaedic & Sports Physical Therapy 18, 402-408 [DOI] [PubMed] [Google Scholar]
- Donatelli R., Ellenbecker T.S., Ekedahl S.R., Wilkes J.S., Kocher K., Adam J. (2000) Assessment of shoulder strength in professional baseball pitchers. Journal of Orthopaedic & Sports Physical Therapy 30, 544-551 [DOI] [PubMed] [Google Scholar]
- Duda M. (1985) Prevention and treatment of throwing-arm injuries. Physician and Sportsmedicine 13, 181-184; 186 [DOI] [PubMed] [Google Scholar]
- Ellenbecker T.S., Roetert E.P., Bailie D.S., Davies G.J., Brown S.W. (2002) Glenohumeral joint total rotation range of motion in elite tennis players and baseball pitchers Medicine & Science in Sports & Exercise 34, 2052-2056 [DOI] [PubMed] [Google Scholar]
- Elliot B., Grove J.R., Gibson B. (1988) Timing of the lower limb drive and throwing limb movement in baseball pitching. International Journal of Sport Biomechanics 4, 59-67 [Google Scholar]
- Elliott B., Grove J.R., Gibson B., Thurston B. (1986) A three-dimensional cinematographic analysis of the fastball and curveball pitches in baseball. IJSB: International Journal of Sport Biomechanics 2, 20-28 [Google Scholar]
- Escamilla R., Fleisig G., Barrentine S., Andrews J., Moorman C., 3rd (2002) Kinematic and kinetic comparisons between American and Korean professional baseball pitchers. Sports Biomechanics 1, 213-228 [DOI] [PubMed] [Google Scholar]
- Escamilla R.F., Fleisig G.S., Barrentine S.W., Zheng N., Andrews J.R. (1998) Kinematic comparisons of throwing different types of baseball pitches. Journal of Applied Biomechanics 14, 1-23 [Google Scholar]
- Feltner M., Dapena J. (1986) Dynamics of the shoulder and elbow joints of the throwing arm during a baseball pitch International Journal of Sport Biomechanics 2, 235-259 [Google Scholar]
- Feltner M.E. (1989) Three-dimensional interactions in a two-segment kinetic chain. Part II: Application to the throwing arm in baseball pitching. International Journal of Sport Biomechanics 5, 420-450 [Google Scholar]
- Fleisig G., Escamilla R., Andrews J., Matsuo T., Satterwhite Y., Barrentine S. (1996) Kinematic and kinetic comparison between baseball pitching and football passing. Journal of Applied Biomechancs 12, 207-224 [Google Scholar]
- Fleisig G.S. (1994) The biomechanics of baseball pitching. Doctoral thesis University of Alabama [Google Scholar]
- Fleisig G.S., Andrews J.R., Dillman C.J., Escamilla R.F. (1995) Kinetics of baseball pitching with implications about injury mechanisms. American Journal of Sports Medicine 23, 233-239 [DOI] [PubMed] [Google Scholar]
- Fleisig G.S., Barrentine S.W., Escamilla R.F., Andrews J.R. (1996) Biomechanics of overhand throwing with implications for injuries. Sports Medicine 21, 421-437 [DOI] [PubMed] [Google Scholar]
- Fleisig G.S., Barrentine S.W., Zheng N., Escamilla R.F., Andrews J.R. (1999) Kinematic and kinetic comparison of baseball pitching among various levels of development. Journal of Biomechanics 32, 1371-1375 [DOI] [PubMed] [Google Scholar]
- Fleisig G.S., Escamilla R.F. (1996) Biomechanics of the elbow in the throwing athlete. Operative Techniques in Sports Medicine 4, 62-68 [Google Scholar]
- Gainor B.J., Piotrowski G., Puhl J., Allen W.C., Hagen R. (1980) The throw: biomechanics and acute injury. American Journal of Sports Medicine 8, 114-118 [DOI] [PubMed] [Google Scholar]
- Grana W.A., Rashkin A. (1980) Pitcher's elbow in adolescents .American Journal of Sports Medicine 8, 333-336 [DOI] [PubMed] [Google Scholar]
- Grove J.R., Elliott B.C., Gibson B. (1988) Performance correlates of pitching from the windup and set positions. Journal of Applied Research in Coaching and Athletics 3, 274-288 [Google Scholar]
- Gugenheim J.J.Jr., Stanley R.F., Woods G.W., Tullos H.S. (1976) Little League survey: the Houston study. American Journal of Sports Medicine 4, 189-200 [DOI] [PubMed] [Google Scholar]
- Hamner D.L., Pink M.M., Jobe F.W. (2000) A modification of the relocation test: arthroscopic findings associated with a positive test. Journal of Shoulder and Elbow Surgery 9, 263-267 [DOI] [PubMed] [Google Scholar]
- Hill J.A. (1983) Epidemiologic perspective on shoulder injuries. Clinics in Sports Medicine 2, 241-246 [PubMed] [Google Scholar]
- Hirashima M., Kadota H., Sakurai S., Kudo K., Ohtsuki T. (2002) Sequential muscle activity and its functional role in the upper extremity and trunk during overarm throwing. Journal of Sports Sciences 20, 301-310 [DOI] [PubMed] [Google Scholar]
- Jobe F.W., Kvitne R.S., Giangarra C.E. (1989) Shoulder pain in the overhand or throwing athlete. The relationship of anterior instability and rotator cuff impingement. Orthopaedic Review 18, 963-975 [PubMed] [Google Scholar]
- Jobe F.W., Nuber G. (1986) Throwing injuries of the elbow. Clinics in Sports Medicine 5, 621-636 [PubMed] [Google Scholar]
- Jobe F.W., Pink M.M. (1996) Operative techniques in upper extremity sports injuries. Mosby, St. Louis [Google Scholar]
- Johnson L. (1992) Patterns of shoulder flexibility among college baseball players Journal of athletic training. 27, 44-45;48-49 [PMC free article] [PubMed] [Google Scholar]
- Joyce M.E., Jelsma R.D., Andrews J.R. (1995) Throwing injuries to the elbow. Sports Medicine and Arthroscopy Review 3, 224-236 [Google Scholar]
- Karduna A.R., McClure P.W., Michener L.A., Sennett B. (2001) Dynamic measurements of three-dimensional scapular kinematics: A validation study. Journal of Biomechanical Engineering, 123, 184-190 [DOI] [PubMed] [Google Scholar]
- Ketlinski R. (1971) How is the curveball thrown? The Athletic Journal 51, 75-76 [Google Scholar]
- Kreighbaum E., Barthels K.M. (1985) Biomechanics: A qualitative approach for studying human movement. 2nd edition Burgess Pub. Co., Minneapolis, Minn [Google Scholar]
- Kronberg M., Brostrom L.A. (1990) Humeral head retroversion in patients with unstable humeroscapular joints. Clinical Orthopaedics 207-211 [PubMed] [Google Scholar]
- Kronberg M., Brostrom L.A. (1991) Proximal humeral osteotomy to correct the anatomy in patients with recurrent shoulder dislocations. Journal of Orthopaedic Trauma, 5, 129-133 [DOI] [PubMed] [Google Scholar]
- Kronberg M., Brostrom L.A. (1995) Rotation osteotomy of the proximal humerus to stabilise the shoulder. Five years' experience. The Journal of Bone and Joint Surgery. British Volume, 77, 924-927 [PubMed] [Google Scholar]
- Kronberg M., Brostrom L.A., Posch E. (1993) Stability in relation to humeral head retroversion after surgical treatment of recurrent anterior shoulder dislocations Orthopedics 16, 281-285 [DOI] [PubMed] [Google Scholar]
- Kronberg M., Brostrom L.A., Soderlund V. (1990) Retroversion of the humeral head in the normal shoulder and its relationship to the normal range of motion. Clinical Orthopaedics, 113-117 [PubMed] [Google Scholar]
- Larson R.L., Singer K.M., Bergstrom R., Thomas S. (1976) Little League survey: the Eugene study American Journal of Sports Medicine 4, 201-209 [DOI] [PubMed] [Google Scholar]
- Levin J.S., Zheng N., Dugas J., Cain E.L., Andrews J.R. (2004) Posterior olecranon resection and ulnar collateral ligament strain. Journal of Shoulder and Elbow Surgery 13, 66-71 [DOI] [PubMed] [Google Scholar]
- Lyman S., Fleisig G.S., Andrews J.R., Osinski E.D. (2002) Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. American Journal of Sports Medicine 30, 463-468 [DOI] [PubMed] [Google Scholar]
- Lyman S., Fleisig G.S., Waterbor J.W., Funkhouser E.M., Pulley L., Andrews J.R., Osinski E.D., Roseman J.M. (2001) Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Medicine & Science in Sports & Exercise 33, 1803-1810 [DOI] [PubMed] [Google Scholar]
- MacWilliams B.A., Choi T., Perezous M.K., Chao E.Y.S., McFarland E.G. (1998) Characteristic ground-reaction forces in baseball pitchng. American Journal of Sports Medicine 26, 66-71 [DOI] [PubMed] [Google Scholar]
- Matsen F.A.3rd., Harryman D.T., 2nd., Sidles J.A. (1991) Mechanics of glenohumeral instability. Clinics in Sports Medicine 10, 783-788 [PubMed] [Google Scholar]
- Matsuo T., Escamilla R.F., Fleisig G.S., Barrentine S.W., Andrews J.R. (2001) Comparison of kinematic and temporal parameters between different pitch velocity groups. Journal of Applied Biomechanics 17, 1-13 [Google Scholar]
- Matsuo T., Fleisig G.S., Zheng N.Q., Andrews J.R. (2006) Influence of shoulder abduction and lateral trunk tilt on peak elbow varus torque for college baseball pitchers during simulated pitching. Journal of Applied Biomechanics 22, 93-102 [DOI] [PubMed] [Google Scholar]
- Matsuo T., Flesig G.S., Barrentine S., Zheng N. (2003) Lateral trunk tilt influences the optimal shoulder abduction during baseball pitching. International Society of Biomechanics XIXth Congress, Dunedin, New Zealand [Google Scholar]
- Matsuo T., Matsumoto T., Mochizuki Y., Takada Y., Saito K. (2002) Optimal shoulder abduction angles during baseball pitching from maximal wrist velocity and minimal kinetics viewpoints. Journal of Applied Biomechanics 18, 306-320 [Google Scholar]
- Matsuo T., Matsumoto T., Takada Y. (1999) Influence of different shoulder abduction angles during baseball pitching on throwing performance and joint kinetics. International Society of Biomechanics [Google Scholar]
- Matsuo T., Takada Y., Matsumoto T., Saito K. (2000) Biomechanical characteristics of sidearm and underhand baseball pitching: comparison with those of overhand and three-quarter-hand pitching. Japanese Journal of Biomechanics in Sports and Exercise 4, 243-252 [Google Scholar]
- McClure P.W., Michener L.A., Sennett B.J., Karduna A.R. (2001) Direct 3-dimensional measurement of scapular kinematics during dynamic movements in vivo. Journal of Shoulder and Elbow Surgery 10, 269-277 [DOI] [PubMed] [Google Scholar]
- McFarland E.G., Wasik M. (1998) Epidemiology of collegiate baseball injuries. Clinical Journal of Sport Medicine 8, 10-13 [DOI] [PubMed] [Google Scholar]
- Meister K., (2000) Injuries to the shoulder in the throwing athlete. Part two: evaluation/treatment.[see comment]American Journal of Sports Medicine 28, 587-601 [DOI] [PubMed] [Google Scholar]
- Montgomery J., Knudson D. (2002) A method to determine stride length for baseball pitching. Applied Research in Coaching and Athletics Annual 17, 75-84 [Google Scholar]
- Murata A. (2001) Shoulder joint movement of the non-throwing arm during baseball pitch--comparison between skilled and unskilled pitchers. Journal of Biomechanics 34, 1643-1647 [DOI] [PubMed] [Google Scholar]
- Nadler S.F. (2004) Injury in a throwing athlete: understanding the kinetic chain. American Journal of Physical Medicine & Rehabilitation 83, 79. [DOI] [PubMed] [Google Scholar]
- Nelson T.L. (2001) Musculoskeletal Q & A: Practical answers to your critical questions. Preventing Little League elbow. Journal of Musculoskeletal Medicine 18, 292 [Google Scholar]
- Nicholls R., Fleisig G., Elliott B., Lyman S., Osinski E. (2003) Accuracy of qualitative analysis for assessment of skilled baseball pitching technique. Sports Biomechanics 2, 213-226 [DOI] [PubMed] [Google Scholar]
- Norkus S.A. (2000) A comparison of the three-dimensional characteristics of a full-effort overhand throw and the throwing motions involved in a rehabilitative throwing program. Doctoral thesis, The University of Toledo [Google Scholar]
- Olsen S.J., 2nd., Fleisig G.S., Dun S., Loftice J., Andrews J.R. (2006) Risk factors for shoulder and elbow injuries in adolescent baseball pitchers. American Journal of Sports Medicine 34, 905-912 [DOI] [PubMed] [Google Scholar]
- Osbahr D.C., Cannon D.L., Speer K.P. (2002) Retroversion of the humerus in the throwing shoulder of college baseball pitchers. American Journal of Sports Medicine 30, 347-353 [DOI] [PubMed] [Google Scholar]
- Pappas A.M., Zawacki R.M., McCarthy C.F. (1985a) Rehabilitation of the pitching shoulder. American Journal of Sports Medicine 13, 223-235 [DOI] [PubMed] [Google Scholar]
- Pappas A.M., Zawacki R.M., Sullivan T.J. (1985b) Biomechanics of baseball pitching. A preliminary report. American Journal of Sports Medicine 13, 216-222 [DOI] [PubMed] [Google Scholar]
- Pieper H.G. (1998) Humeral torsion in the throwing arm of handball players. American Journal of Sports Medicine, 26, 247-253 [DOI] [PubMed] [Google Scholar]
- Pincivero D.M., Heinrichs K., Perrin D.H. (1994) Medial elbow stability. Clinical implications. Sports Medicine 18, 141-148 [DOI] [PubMed] [Google Scholar]
- Pomianowski S., O'Driscoll S.W., Neale P.G., Park M.J., Morrey B.F., An K.N. (2001) The effect of forearm rotation on laxity and stability of the elbow. Clinical Biomechanics 16, 401-407 [DOI] [PubMed] [Google Scholar]
- Pradhan R.L., Itoi E., Hatakeyama Y., Urayama M., Sato K. (2001) Superior labral strain during the throwing motion. A cadaveric study. American Journal of Sports Medicine 29, 488-492 [DOI] [PubMed] [Google Scholar]
- Rash G.S., Shapiro R. (1995) A three-dimensional dynamic analysis of the quarterback's throwing motion in American football. Journal of Applied Biomechancs 11, 443-459 [Google Scholar]
- Reagan K.M., Meister K., Horodyski M.B., Werner D.W., Carruthers C., Wilk K. (2002) Humeral retroversion and its relationship to glenohumeral rotation in the shoulder of college baseball players. American Journal of Sports Medicine 30, 354-360 [DOI] [PubMed] [Google Scholar]
- Roberts T.W. (1971) Cinematography in biomechanical investigation: selected topics in biomechanics. CIC Symposium on Biomechanics Chicago Ser. Ed. 41-50 [Google Scholar]
- Sabick M.B., Torry M.R., Lawton R.L., Hawkins R.J. (2004) Valgus torque in youth baseball pitchers: A biomechanical study. Journal of Shoulder and Elbow Surgery 13, 349-355 [DOI] [PubMed] [Google Scholar]
- Saitou K., Ohgi Y., Ichikawa H., Adachi K., Miyaji C., Takai S. (2000) Comparison of forearm motion before and after ball-release between fast ball and curve ball pitches. In: 5th Annual Congress of the European College of Sport Science Proceedings Jyväskylä: Finaland. Eds: Avela K.P., Komulainen J.638 [Google Scholar]
- Saitou K., Ohgi Y., Ichikawa H., Inoue S., Matsuo T., Adachi K., Miyaji C., Takai S. (2001) Change in upper limb muscle activity when ball speed increases and type of pitch differs.) Bulletin of Institute of Health and Sport Sciences 24, 79-88 [Google Scholar]
- Sakurai S., Ikegami Y., Okamoto A., Yabe K., Toyoshima S. (1993) A three-dimensional cinematographic analysis of upper limb movement during fastball and curveball baseball pitches. Journal of Applied Bbiomechanics 9, 47-65 [Google Scholar]
- Selecky M.T., Tibone J.E., Yang B.Y., McMahon P.J., Lee T.Q. (2003) Glenohumeral joint translation after arthroscopic thermal capsuloplasty of the rotator interval. Journal of Shoulder and Elbow Surgery 12, 139-143 [DOI] [PubMed] [Google Scholar]
- Shimada K., Ae M., Fujii N., Yuki M., Kawamura T. (2000) Biomechanical study on the functions of the torso and lower limbs in baseball pitching. Japanese Journal of Biomechanics in Sports and Exercise 4, 47-60 [Google Scholar]
- Sisto D.J., Jobe F.W., Moynes D.R., Antonelli D.J. (1987) An electromyographic analysis of the elbow in pitching. American Journal of Sports Medicine 15, 260-263 [DOI] [PubMed] [Google Scholar]
- Stevenson J.M. (1985) Finger release sequence for fastball and curveball pitches. Canadian Journal of Applied Sport Sciences 110, 21-25 [PubMed] [Google Scholar]
- Stodden D.F., Fleisig G.S., McLean S.P., Lyman S.L., Andrews J.R. (2001) Relationship of pelvis and upper torso kinematics to pitched baseball velocity. Journal of Applied Biomechanics 17, 164-172 [DOI] [PubMed] [Google Scholar]
- Tarbell T. (1971) Some mechanical aspects of the overarm throw. Selected topics in biomechanics: Proceedings of the C.I.C. Symposium on Biomechanics Chicago, USA [Google Scholar]
- Tullos H.S., King J.W. (1973) Throwing mechanism in sports. Orthopedic clinics of North America 4, 709-720 [PubMed] [Google Scholar]
- Walsh D. (1989) Shoulder evaluation of the throwing athlete. Sports Medicine Update 4, 24-27 [Google Scholar]
- Wang Y.T., Ford H.T., Shin D.M. (1995) Three dimensional kinematic analysis of baseball pitching in acceleration phase. Perceptual and Motor Skills 80, 43-48 [DOI] [PubMed] [Google Scholar]
- Watkins R.G., Dennis S., Dillin W.H., Schnebel B., Schneiderman G., Jobe F., Farfan H., Perry J., Pink M. (1989) Dynamic EMG analysis of torque transfer in professional baseball pitchers. Spine 14, 404-408 [DOI] [PubMed] [Google Scholar]
- Werner S.L., Fleisig G.S., Dillman C.J., Andrews J.R. (1993) Biomechanics of the elbow during baseball pitching. Journal of Orthopaedic & Sports Physical Therapy 17, 274-278 [DOI] [PubMed] [Google Scholar]
- Werner S.L., Gill T.J., Murray T.A., Cook T.D., Hawkins R.J. (2001) Relationships between throwing mechanics and shoulder distraction in professional baseball pitchers. American Journal of Sports Medicine 29, 354-358 [DOI] [PubMed] [Google Scholar]
- Werner S.L., Murray T.A., Hawkins R.J., Gill T.J. (2002) Relationship between throwing mechanics and elbow valgus in professional baseball pitchers. Journal of Shoulder & Elbow Surgery 11, 151-155 [DOI] [PubMed] [Google Scholar]
- Wilk K.E., Meister K., Fleisig G., Andrews J.R. (2000) Biomechanics of the overhead throwing motion. Sports Medicine and Arthroscopy Review 8, 124-134 [Google Scholar]
- Wilson F.D., Andrews J.R., Blackburn T.A., McCluskey G. (1983) Valgus extension overload in the pitching elbow. American Journal of Sports Medicine 11, 83-88 [DOI] [PubMed] [Google Scholar]
- Xue Q., Masuda K. (1997) A biomechanical study of fast throwing movements of the shoulder in baseball pitching. Chinese Medical Journal 110, 220-224 [PubMed] [Google Scholar]
- Zheng N., Fleisig G., Andrews J. (1999) Biomechanics and injuries of the shoulder during throwing. Athletic Therapy Today 4, 6-10 [Google Scholar]