

Abstract
Adult onset Still's disease (AOSD) is a systemic inflammatory disorder of unknown etiology characterized by spiking fever, evanescent skin rash, arthralgia or arthritis, involvement of various organs, and predominantly neutrophilic leucocytosis. AOSD, although uncommon, has a characteristic constellation of clinical and laboratory features and should be considered in the differential diagnosis of pyrexia of unknown origin associated with a rash and arthralgia. The diagnosis is one of clinical suspicion and it is essential that infections, malignancy, and other rheumatic diseases are excluded. We report a case which illustrates the typical features of AOSD that were treated with steroids and azathioprine.
Keywords: Adult-onset Still's disease, AOSD, Still's disease
Introduction
What was known?
Adult onset Still's disease (AOSD) is a systemic inflammatory disorder of unknown etiology characterized by spiking fever, evanescent salmon-pink skin rash, polyarthralgia or polyarthritis, involvement of various organs and predominantly neutrophilic leucocytosis. The diagnosis is one of clinical suspicion, requiring the exclusion of infection, malignancy, and systemic disease. The typical Still's rash is transient, asymptomatic macular or maculopapular and has a characteristic salmon-pink colour. It is regarded as a major diagnostic criterion with high sensitivity and specificity.
Adult-onset Still's disease (AOSD) is a systemic inflammatory disorder of unknown etiology characterized by spiking fever, evanescent skin rash, arthralgia or arthritis, involvement of various organs, and predominantly neutrophilic leucocytosis. We report a case which illustrates the typical features of AOSD that were treated with steroids and azathioprine.
Case Report
A 23-year-old male was admitted for acute viral myopericarditis with heart failure in which he presented with chest pain associated with dyspnoea, persistent spiking fever with temperature more than 39°C, sore throat, productive cough, and arthralgia. In addition, he developed transient non-pruritic rashes over the neck, axillae, and limbs. Clinical examination revealed a febrile patient who was in heart failure. He had cervical lymphadenopathy, hepatosplenomegaly, and non-scaly orange red plaques and papules over the neck, axillae, and limbs [Figures 1 and 2].
Figure 1.

Urticated and erythematous plaques and papules on the dorsum of right hand and fingers
Figure 2.

Urticated plaques over the right antecubital fossa
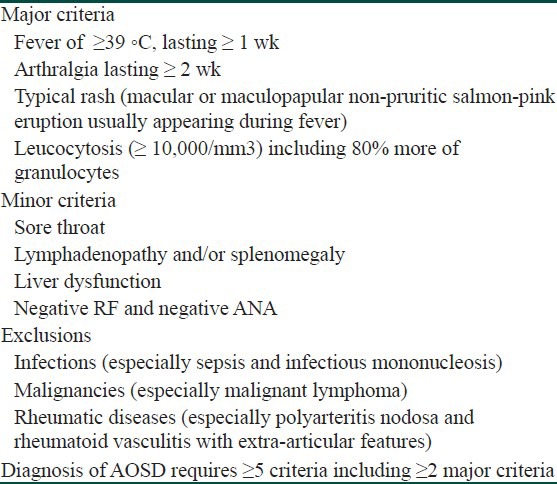
Laboratory investigations revealed raised cardiac enzymes, positive Troponin I, ECG changes consistent with pericarditis, marked leucocytosis with neutrophil predominance, hyperferritinemia, and elevated erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The rheumatoid factor (RF), anti-nuclear antibody (ANA), and anti-dsDNA were negative. Blood and urine cultures were also negative. Histopathological examination of the skin biopsy revealed features of a neutrophilic dermatosis [Figure 3]. He was diagnosed with AOSD as he had four major and three minor criteria for this entity according to the Yamaguchi's criteria [Table 1].
Figure 3.
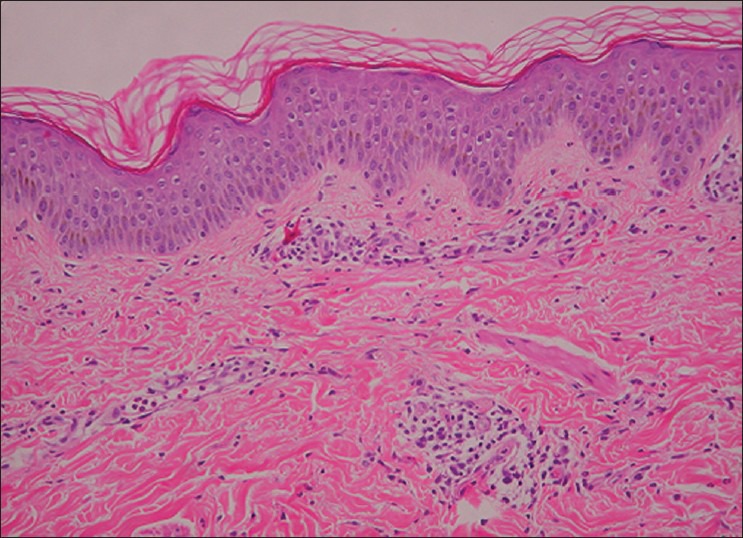
Histology shows superficial and deep perivascular infiltrates of lymphocytes and neutrophils with neutrophils in between collagen bundles
Table 1.
Yamaguchi's criteria for diagnosis of adult-onset Still's disease
He was treated with steroids, diclofenac and azathioprine, which controlled the rash and improved the arthralgia. Subsequently, the patient was out of heart failure and myopericarditis resolved.
Discussion
AOSD is a systemic inflammatory disorder of unknown etiology characterized by spiking fever, evanescent salmon-pink skin rash, polyarthralgia or polyarthritis, involvement of various organs and predominantly neutrophilic leucocytosis. The diagnosis is one of clinical suspicion, requiring the exclusion of infection, malignancy, and systemic disease.[1] A number of authors have proposed a diagnostic criteria for AOSD with the most sensitive being the one proposed by Yamaguchi et al.[1] [Table 1].
Patients who have AOSD commonly present with fever which is classically described as quotidian, with temperature spiking once a day to 39°C or higher, usually in the evening or night as in our patient. The typical Still's rash is transient, asymptomatic macular, or maculopapular and has a characteristic salmon-pink color.[2] It is regarded as a major diagnostic criterion with high sensitivity and specificity. The rash is frequently evanescent lasting a few hours and prominent during febrile spikes. Various atypical skin lesions such as persistent pruritic plaques have been reported in sporadic cases with active AOSD.[3] It is characterized by necrotic keratinocytes in the upper half of epidermis with a neutrophilic infiltrate in the papillary dermis histologically.[3] Arthralgia is universal and usually increases in intensity with the fever spike.
Our patient presented with myopericarditis with congestive cardiac failure and pleural effusion which is a rare manifestation that has been reported in previous literature.[4] Myocarditis is a known complication in AOSD and may result in cardiac failure or arrhythmia. It is therefore imperative to screen and investigate patients for cardiac involvement, particularly those presenting with chest pain, tachycardia, or mild ST elevations on ECG.
Laboratory tests are non-specific and reflect heightened immunological activity. The most striking abnormality is a marked leucocytosis with neutrophilic predominance as seen in our patient. An increased ESR is universal and the CRP level is commonly elevated. Marked hyperferritinemia associated with diminished concentration of glycosylated ferritin is a characteristic feature of AOSD.[5] The histological findings of a skin biopsy are non-specific and variable. There is often a relatively sparse perivascular mixed inflammatory infiltrate containing some neutrophils as seen in our patient.
The management of AOSD is first directed at the acute systemic features of the disease. In chronic disease, arthritis is the major concern. Treatment consists of non-steroidal anti-inflammatory agents (NSAIDs), corticosteroids, disease modifying anti-rheumatic drugs (DMARD), immunosuppressive agents, and intravenous gamma globulin (IVIG). The recent successful application of biologic agents, often in combination with traditional immunosuppressive agents, has been very promising. Immunosuppressive agents including methotrexate, azathioprine, and cyclosporine A have been used as second-line drugs in the treatment of AOSD. In our case, the patient was commenced on azathioprine in addition to steroids.
In conclusion, AOSD, although uncommon, has characteristic constellation of clinical and laboratory features and should be considered in the differential diagnosis of pyrexia of unknown origin associated with a rash and arthralgia. The diagnosis is one of clinical suspicion and it is essential that infections, malignancy, and other rheumatic diseases are excluded.
What is new?
Various atypical skin lesions such as persistent pruritic plaques and prurigo pigmentosa-like lesions have been reported in sporadic cases with active AOSD. There were frequent reports of AOSD patients who presented with pruritic persistent papules and plaques clinically. A recent case series demonstrated that it is characterized by necrotic keratinocytes in the upper half of epidermis with a neutrophilic infiltrate in the papillary dermis histologically. This type of rash may represent a specific manifestation of this syndrome and awareness of the distinctive pathologic features of persistent plaques and papules may facilitate an earlier diagnosis of AOSD.
Myocarditis is a known complication in AOSD and may result in cardiac failure or arrhythmia. Therefore it is imperative to monitor patients closely with routine ECGs and echocardiographies in AOSD patients presenting even with vague signs of myocarditis such as chest pain, tachycardia or mild ST-elevations on ECG.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H, et al. Preliminary criteria for classification of adult Still's disease. J Rheumatol. 1992;19:424–30. [PubMed] [Google Scholar]
- 2.Mok CC, Lau CS, Wong RW. Clinical characteristics, treatment, and outcome of adult onset Still's disease in southern Chinese. J Rheumatol. 1998;25:2345–51. [PubMed] [Google Scholar]
- 3.Wolgamot G, Yoo J, Hurst S, Gardner G, Olerud J, Argenyi Z. Unique histopathologic findings in a patient with adult-onset Still disease. Am J Dermatopathol. 2007;29:194–6. doi: 10.1097/DAD.0b013e3180332826. [DOI] [PubMed] [Google Scholar]
- 4.Kristensen LE, Bartosik I. Myocarditis in adult-onset Still's disease despite significant immunosuppressive therapy. Scand J Rheumatol. 2006;35:330–1. doi: 10.1080/03009740500499492. [DOI] [PubMed] [Google Scholar]
- 5.Fautrel B, Le Moël G, Saint-Marcoux B, Taupin P, Vignes S, Rozenberg S, et al. Diagnostic value of ferritin and glycosylated ferritin in adult onset Still's disease. J Rheumatol. 2001;28:322–9. [PubMed] [Google Scholar]