

Sir,
Walker Warburg syndrome (WWS) is a rare form of autosomal recessive congenital muscular dystrophy with brain and eye abnormalities. Incidence of this rare syndrome is still unknown although a study from Italy suggests an incidence rate of 1.2/100,000 live births.[1] WWS is a genetically heterogeneous disease presenting with congenital muscular dystrophy, type II cobblestone lissencephaly[2,3] hydrocephalus, cerebellar malformations, and eye abnormalities.[1,2,3] There can be various anterior segment abnormalities associated with this syndrome like cataract, shallow anterior chamber, microcornea, microphthalmos, and lens defects. Posterior segment abnormalities such as retinal detachment, dysplasia, atrophy of the optic nerve coloboma, and glaucoma may be associated. It is very unusual to find microphthalmos occurring together with megalophthalmos in WWS. We would like to report such a case of WWS with the left eye megalophthalmos and right eye micropthalmos.
Case Report
A 1-day-old term female baby of primigravida was admitted with chief complaints of dehydration, inability to feed, and abnormal eye features.
On examination, she was found to have small anterior fossa with overriding of sutures, depressed nasal bridge, low set ears, pedal edema, skin fold at the nape of neck, widely spaced nipples, vulval anus, bilateral cortical thumb, retrognathia, short neck, generalized hypotonia. Further evaluation revealed congenital dislocation of both hip joint, hydrocephalus and hyperbilirubinemia.
Ocular examination showed right eye-microphthalmia, left eye-megalophthalmos [Figure 1], flat anterior chamber (corneo endothelial touch), and non-dilating non-reacting 1.00 mm pupil. B-scan right eye shows axial length of 12 mm, left eye shows axial length of 24 mm. Intraocular pressure left eye was 18 mm Hg (perkins applanation).
Figure 1.

Microphthalmos with megalophthalmos
USG skull showed hydrocephalus. Magnetic resonance imaging was suggestive of Dandy-Walker variant with small posterior fossa cyst communicating with 4th ventricle associated with gross communicating hydrocephalus [Figure 2]. Serum creatinine kinase level: 147 units/L (Normal range 0-25 units/L). Above findings confirm the case as WWS.
Figure 2.
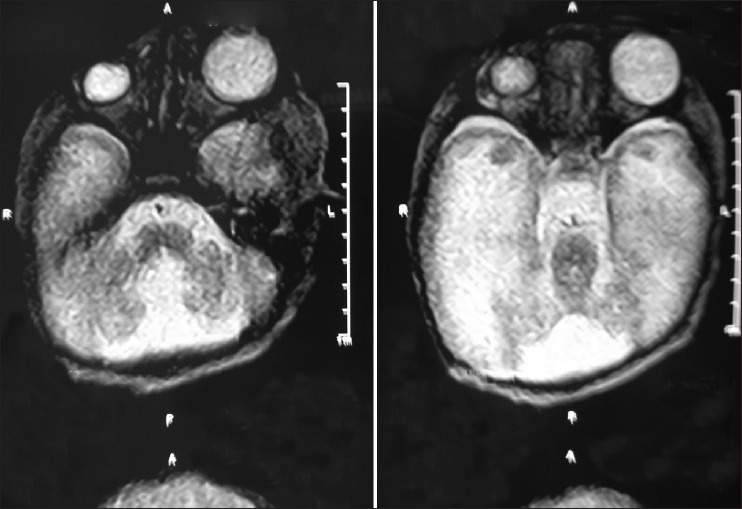
Magnetic resonance imaging shows Dandy-Walker variant with small posterior cyst communicating with 4th ventricle
Discussion
WWS is the most severe form of congenital muscular dystrophy[4] with most children dying before the age of 3 years. WWS presents at birth with generalized hypotonia, muscle weakness, developmental delay with mental retardation, and occasional seizures. It is associated with type II cobblestone lissencephaly, hydrocephalus, cerebellar malformations, eye abnormalities, and congenital muscular dystrophy characterized by hypoglycosylation of α-dystroglycan. Several genes have been implicated in the etiology of WWS, and several mutations were found such as Protein O-mannosyl transferase 1 (POMT 1) and POMT 2.[5]
WWS is associated with generalized hypotonia, muscle weakness, developmental delay with mental retardation and in some children, seizures. There may be a variety of the anterior eye anomalies (cataracts, shallow anterior chamber, microcornea and microphthalmia, and lens defects) and a spectrum of posterior eye anomalies (retinal detachment or dysplasia, hypoplasia or atrophy of the optic nerve and macula and coloboma). Glaucoma or buphthalmos may be present.
Brain abnormalities include migrational defect with type II lissencephaly (cobblestone type), hydrocephalus, vermal or general cerebellar hypoplasia, and flat brainstem with small pyramids. White matter shows hypomyelination. Additional brain anomalies such as hypoplasia/agenesis of the corpus callosum, occipital encephalocele, and Dandy-Walker malformation have been described. Other recognized associated anomalies are small penis, undescended testes, and rarely, other facial dysmorphic features such as low set or prominent ears and cleft lip or palate.
Laboratory investigations usually show elevated creatine kinase, myopathic/dystrophic muscle pathology and altered α-dystroglycan.[6]
WWS is autosomal recessive, in families with one affected child risk of having another affected child is 25%.
Rehany et al. in 1999 has reported two similar cases of WWS with unilateral glaucoma with buphthalmos and has described the presence of mesenchymal tissue in anterior angle covered by endothelium, although, in our case, there is flat anterior chamber and normal Intraocular pressure in megalophthalmic eye.[7]
Antenatal molecular diagnosis is possible in families with known mutation, although antenatal ultrasound can detect hydrocephalus at 18 weeks of gestation.
This condition is lethal with children dying before their third birthday.
References
- 1.Mostacciuolo ML, Miorin M, Martinello F, Angelini C, Perini P, Trevisan CP. Genetic epidemiology of congenital muscular dystrophy in a sample from north-east Italy. Hum Genet. 1996;97:277–9. doi: 10.1007/BF02185752. [DOI] [PubMed] [Google Scholar]
- 2.Walker AE. Lissencephaly. Arch Neurol Psychiatry. 1942;48:13–29. [Google Scholar]
- 3.Nabi NU, Mezer E, Blaser SI, Levin AA, Buncic JR. Ocular findings in lissencephaly. J AAPOS. 2003;7:178–84. doi: 10.1016/s1091-8531(02)42005-8. [DOI] [PubMed] [Google Scholar]
- 4.Warburg M. The heterogeneity of microphthalmia in the mentally retarded. Birth Defects Orig Artic Ser. 1971;7:136–54. [PubMed] [Google Scholar]
- 5.Vajsar J, Schachter H. Walker-Warburg syndrome. Orphanet J Rare Dis. 2006;1:29. doi: 10.1186/1750-1172-1-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Dobyns WB, Pagon RA, Armstrong D, Curry CJ, Greenberg F, Grix A, et al. Diagnostic criteria for Walker-Warburg syndrome. Am J Med Genet. 1989;32:195–210. doi: 10.1002/ajmg.1320320213. [DOI] [PubMed] [Google Scholar]
- 7.Rehany U, Segal ZI, Rumelt S. Congenital unilateral buphthalmos in Walker-Warburg syndrome: A clinicopathological study. Eye (Lond) 1999;13:778–80. doi: 10.1038/eye.1999.227. [DOI] [PubMed] [Google Scholar]