
Figure 2.
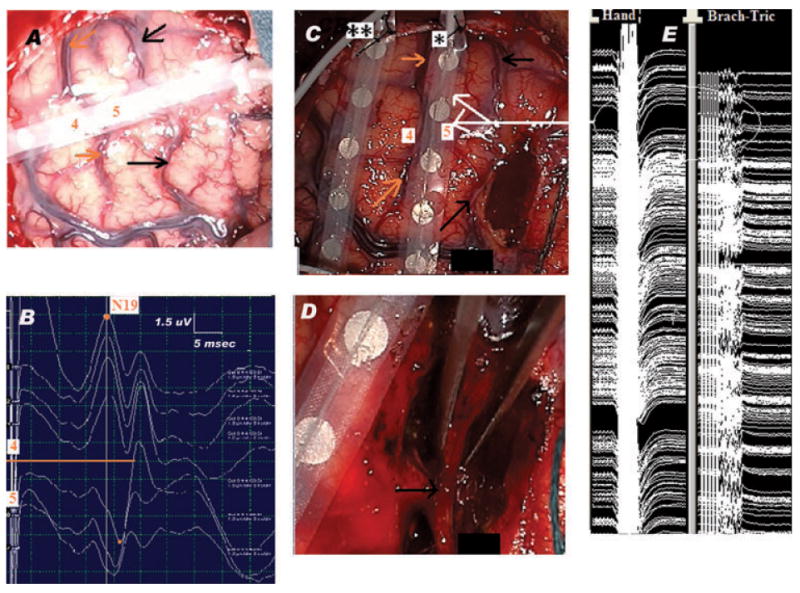
Pericentral region: Neurophysiologic-neuroanatomic correlation. Lesionectomy under continuous MEP monitoring. (A) Surgical field showing the SSEP recording strip placed across the precentral (black arrows) and central (orange arrows) sulci, with contact 5 over the hand region within the motor strip and contact 4 in the postcentral region, over the somatosensory cortex. (B) MSSEP phase reversal technique: the MSSEPs are recorded via the eight-contact subdural strip placed over the right frontoparietal cortex, perpendicular and across the presumed location of the CS, as shown in panel A. The reference electrode is located on the contralateral mastoid. The left median nerve is stimulated at the wrist with repetitive electrical pulses, at 3.17 Hz, pulse width 0.3 ms, intensity 15 mA. The orange line centers the SSEP phase reversal, which occurs at the level of CS. Note N19 recorded as a negative peak at contact 4 of the strip, in a referential montage. The recording is done using a 16-channel EP machine (XLTEK manufacturer), LFF = 30 Hz, HFF = 500 Hz. (C) Resection of the anterior portion of the lesion, situated anterior to the precentral sulcus (black arrows). Notice the placement of the two strips, one used for cortical stimulation (*), the other used for recording ADs (**). The orange arrows point toward the CS; labels 4 and 5 show the previous position of contacts 4 and 5, respectively, of the strip used for CS localization. The white arrows show the location of areas of the motor strip, which stimulated at PMC threshold (i.e., 10 mA) triggered MEPs in hand and arm regions. The stimulation was done via a handheld monopolar stimulator, connected to the anode. The cathode was a sterile needle placed at the periphery of the surgical field. Repetitive trains of six monophasic electrical pulses (250 Hz frequency of pulses within each train, each pulse of 0.5 ms duration), were delivered at 2 Hz. The recording was done using subdermal needle electrodes placed in the contralateral hemibody muscles: orbicularis oris, oculi, masseter, trapezius, deltoid, brachioradialis, triceps, abductor policis brevis (APB), abductor digiti mimini (ADM), quadriceps, anterior tibialis (AT), and abductor hallucis (AH) muscles. Two view windows allowed observation of the muscle channels and identification of MEPs locked to the stimulation as well as of self-sustained and/or spontaneous muscle activity (free EMG). This set up was important in order to easily differentiate stimulus triggered MEPs from motor seizure activity and/or muscle artifact. The PMC mapping threshold was 10 mA. The recording is done using a 16-channel EP machine (XLTEK manufacturer). LFF = 100 Hz, HFF = 2 KHz. (D) End of the resection: lesionectomy was done anterior as well as posterior to the preserved precentral sulcus (black arrow). (E) Continuous hand and arm MEPs (circled) monitoring during resection. Within the precentral gyrus, the location of the stimulated regions is indicated by the white arrows in panel C. The same recording set up was used for both motor mapping and monitoring. However, during the latter, the anodal stimulation was done via one of the contacts of a second subdural strip (*) which was placed on top of the PMC. This change in anodal stimulation resulted in a new PMC threshold (12 mA), used for the MEPs monitoring (using otherwise the same stimulus parameters).
Epilepsia © ILAE