

Abstract
Background
Controversy exists regarding the optimal rate of weight loss for long-term weight management success.
Purpose
This study examined whether gradual initial weight loss was associated with greater long-term weight reduction than rapid initial loss.
Methods
Groups were drawn from participants in the TOURS trial, which included a sample of middle-aged (mean =59.3 years) obese women (mean BMI =36.8) who received a 6-month lifestyle intervention followed by a 1-year extended care program. Participants were encouraged to reduce caloric intake to achieve weight losses of 0.45 kg/ week. Groups were categorized as “FAST” (≥0.68 kg/week, n=69), “MODERATE” (≥0.23 and <0.68 kg/week, n= 104), and “SLOW” (<0.23 kg/week, n=89) based on rate of weight loss during first month of treatment.
Results
The FAST, MODERATE, and SLOW groups differed significantly in mean weight changes at 6 months (−13.5, −8.9, and −5.1 kg, respectively, ps <0.001), and the FAST and SLOW groups differed significantly at 18 months (−10.9, −7.1, and −3.7 kg, respectively, ps <0.001). No significant group differences were found in weight regain between 6 and 18 months (2.6, 1.8, and 1.3 kg, respectively, ps < 0.9). The FAST and MODERATE groups were 5.1 and 2.7 times more likely to achieve 10% weight losses at 18 months than the SLOW group.
Conclusion
Collectively, findings indicate both short- and long-term advantages to fast initial weight loss. Fast weight losers obtained greater weight reduction and long-term maintenance, and were not more susceptible to weight regain than gradual weight losers.
Keywords: Obesity, Weight loss, Lifestyle modification
Introduction
Successful weight loss in obese individuals has been defined as a reduction of 10% or greater of initial body weight maintained for at least 1 year [1, 2]. Numerous studies have demonstrated that lifestyle interventions consisting of 15 to 24 weekly group sessions result in an 8% to 10% reduction of initial body weight [3–5]; however, these beneficial losses are rarely maintained over the long-term [5, 6]. Because weight regain reverses the health benefits achieved with weight loss [7–9], considerable efforts have been placed on identifying behavioral factors that may be associated with long-term success in weight loss maintenance [10–12]. Studies have shown that rate of initial weight loss, even within the first few weeks of treatment, may serve as an important predictor of long-term success [12–17], but controversy exists regarding the optimal rate of initial loss [12, 15–17].
Losing weight at a slow initial rate has been shown to result in continued weight loss, reduced risk for weight regain, and successful long-term weight loss maintenance [16–20]. Lutes et al. [16] demonstrated that overweight and obese women and men who were presented choices for small changes in calories (i.e., 1,500–2,200 kcal/day and 1,900–2,600 kcal/day, respectively) and physical activity during a 16-week treatment attained a modest initial weight loss, sustained the loss, and achieved superior weight reduction at 3-months follow-up compared to those who received standard treatment. Similarly, Sbrocco and colleagues [17] showed that obese women who were prescribed mild restriction in caloric intake (i.e., 1,800 kcal/ day) attained a gradual initial weight loss and were less susceptible to weight regain at 12 months than those in a traditional behavioral treatment group (i.e., 1,200 kcal/day) who achieved a larger initial weight loss. Research investigating the impact of ethnicity on weight loss also supports the proposition that a gradual rate of initial weight loss has beneficial long-term effects; studies have shown that African American participants typically lose less weight initially than Caucasian participants, but have smaller regains and eventually achieve similar long-term losses [18–20].
Conversely, reviews of weight loss patterns have concluded that the greater the initial weight loss in obese patients, the larger the total weight loss observed at long-term follow-up [10, 21]. Jeffery and colleagues [15] found that weight reduction during an initial 12-week weight management program served as the strongest positive predictor of further weight change during a subsequent 40-week follow-up period. Similar predictive results have been shown when assessing weight loss within the initial 6 weeks [13] and within the first month of traditional behavioral treatment programs [12]. While losing weight at a more rapid initial rate has been coupled with greater long-term weight loss, it has also been associated with a larger and more rapid weight regain than a gradual weight reduction [15, 17, 22]. Such findings suggest that a larger initial weight loss may actually serve as a risk factor for later weight regain [2, 23, 24]. At present, controversy exists on how the degree of short-term weight change affects long-term success in weight management. Thus, the current study examined the association between rate of initial weight loss and long-term maintenance of lost weight. Specifically, we assessed whether losing weight at a slow initial rate resulted in larger long-term weight reduction and less weight regain than losing at a fast initial rate.
Methods and Procedures
Study Design and Participants
The present study is a secondary data analysis of the Treatment of Obesity in Underserved Rural Settings (TOURS) randomized controlled trial [25]. A detailed description of the trial is described elsewhere [25]. Participants were 298 relatively healthy, weight stable, obese women between the ages of 50 to 75 years (mean ± SD; 59.3 ± 6.2 years) with a mean baseline weight of 96.5± 14.9 kg and body mass index (BMI) of 36.8 ±5.0 kg/m2. The racial/ethnic composition of the sample is as follows: Caucasian (75.5%); Black, Non-Hispanic (20.5%); Asian, Native American, or Pacific Islander (2.3%); and Hispanic (1.7%).
Phase I of the TOURS trial included 24 weekly group behavioral treatment sessions designed to decrease caloric intake and increase moderate intensity physical activity to facilitate a weight loss of approximately 0.45 kg/week. All participants were encouraged to consume 1,200 kcal/day and to increase physical activity to reach a 10,000/day step average or attain at least 3,000 steps greater than baseline levels. No liquid meal supplements were utilized in the TOURS trial. At the conclusion of Phase I, women began their randomized assignment, a Phase II 12-month follow-up program involving contact twice per month in the form of group sessions, telephone contact, or newsletters. All participants were encouraged to maintain the new eating and exercise habits learned during the Phase I intervention. The university institutional review board approved the study, and informed consent was obtained from all participants.
Measures
The primary outcome measure was change in body weight, which was measured to the nearest 0.1 kg using a certified balance beam scale. Participants were weighed at weekly group sessions and at assessments at baseline and months 6 and 18 while wearing light indoor clothing, without shoes, and with empty pockets.
Secondary outcome measures included caloric intake, physical activity, attendance, and adherence. Caloric intake within the first month was averaged according to daily written food records kept by each participant. Physical activity within the first month of treatment was assessed according to the average number of steps recorded by participants on ACCUSPLIT pedometers. Session attendance was recorded if the participant arrived at the treatment session and was weighed by a staff member. Adherence was measured by the total number of daily records of dietary intake participants completed. Participants did not return food diaries during the first week of the treatment program, thus adherence was calculated according to the number of food records kept between weeks 2 and 4.
Statistical Analyses
Weight-Change Categories
Participants were classified into three categories according to their rate of weight loss during the first month of the intervention. To compare average weekly weight losses, change scores were calculated by subtracting participant baseline weights from weights 1 month into the intervention and then dividing this number by 4. Participants were then categorized into the “FAST” (≥0.68 kg [1.5 lb]/week), “MODERATE” (≥0.23 kg [0.5 lb] and <0.68 kg [1.5 lb]/ week) and “SLOW” (<0.23 kg [0.5 lb]/week) weight loss groups. These specific categories were chosen to center around the typical mean weekly weight loss of approximately 0.4 kg [nearly 1.0 lb]/week found in similar trials of lifestyle of interventions for obesity [26]. A post-hoc power analysis using G*Power 3.1 indicated a 0.98 power to detect a difference among weight loss groups.
Missing Data
Of the original 298 TOURS participants, 36 were excluded because they did not have a recorded weight at 1 month. Thus, data from 262 participants were used in this study. Thirteen participants (FAST, n =1; MOD, n =3; and SLOW, n = 9) did not have recorded weights at 6 months; for these participants, we carried forward their baseline weight, conservatively assuming no treatment effects. Twelve of these 13 cases also had no recorded weights at 18 months, so their baseline weights were again carried forward to fill in the missing 18-month data. Analyses were run with and without these 13 cases and results were similar; therefore, we chose to use this more conservative intent-to-treat format. Nineteen participants had 6-month weights but did not have 18-month weights (FAST, n=4; MOD, n =11; and SLOW, n = 4). For these participants, we added 3.6 kg to their 6-month weights. This 0.3 kg per month addition was based on average weight regain observed in the TOURS trial and other similar lifestyle interventions [25, 27–29].
Residualized Change Scores
Residualized change scores were used to assess differences in the magnitude of weight loss between groups at each time point. These scores were created by regressing 6-month weight on baseline weight, regressing 18-month weight on 6-month weight, and regressing 18-month weight on baseline weight. Each residual was then saved as a change score. This method measures change while accounting for any baseline differences.
Weight Outcomes
A repeated measures analysis of covariance was used to investigate differences in weight change between weight loss groups at 6 and 18 months. Residualized change scores between baseline and 6 months, between 6 and 18 months, and between baseline and 18 months were used as dependent variables versus using weights at each time point. This method allowed for examination of the magnitude of weight loss between groups from baseline to 6 months and baseline to 18 months, as well as weight regain from 6 to 18 months. As a secondary analysis, we investigated which groups were statistically more likely to achieve a clinically significant 10% weight loss at 18 months. For this analysis we used Pearson’s chi-square test, categorizing participants into groups who lost 10% of their baseline weight or greater and participants who lost less than 10%. Finally, we calculated odds ratios to measure the effect size of these associations. All statistical analyses were conducted using SPSS statistical software version 16.0.
Secondary Outcomes
To examine differences between groups in terms of attendance, adherence, caloric intake, and physical activity, we conducted multivariate analyses of variance. Bonferroni-adjusted post-hoc tests were used to investigate differences by weight loss group for total attendance, adherence, average daily caloric intake, and average daily steps taken during the first month of treatment.
Results
Weight Loss Groups
After accounting for missing data, data from 262 participants in the TOURS study were used. Based on weight losses in the first month of treatment, 69 women were categorized into the FAST group, 104 women were categorized into the MODERATE group, and 89 women were categorized into the SLOW group.
Ethnicity varied significantly by group categorization, χ2(2, N = 262), =13.7, p = 0.001, such that the FAST group contained the largest proportion of Caucasian participants while the SLOW group contained the largest proportion of minority participants. Therefore, ethnicity was used as a covariate in all of the following analyses. No additional differences in baseline characteristics were found among groups (see Table 1). Furthermore, no significant group differences were found in baseline caloric intake or physical activity, or in Phase II assignment to group sessions, telephone contact, or twice-monthly newsletter follow-up program.
Table 1.
Baseline Values by Weight Loss Category
| FAST n = 69 |
MODERATE n = 104 |
SLOW n = 89 |
||||
|---|---|---|---|---|---|---|
| Variable | M | SD | M | SD | M | SD |
| Age (years) | 59.2 | 6.1 | 59.6 | 6.5 | 59.1 | 6.0 |
| Weight (kg) | 99.3 | 15.3 | 94.7 | 14.0 | 95.8 | 15.0 |
| BMI (kg/m²) | 37.5 | 4.9 | 36.4 | 4.9 | 36.6 | 5.1 |
| n | % | n | % | n | % | |
| Race/ethnicity | ||||||
| Caucasian | 63 | 91.3% | 79 | 76.0% | 59 | 66.3% |
| African American | 3 | 4.3% | 21 | 20.2% | 28 | 31.5% |
| Hispanic American | 2 | 2.9% | 1 | 1.0% | 2 | 2.2% |
| Asian, Native American, or Pacific Islander | 1 | 1.4% | 3 | 2.9% | 0 | 0.0% |
| Education | ||||||
| 12 years or less | 26 | 37.7% | 39 | 37.5% | 30 | 33.7% |
| 13–15 years | 39 | 56.5% | 53 | 51.0% | 50 | 56.2% |
| 16 years or more | 4 | 5.8% | 12 | 11.5% | 9 | 10.1% |
Initial Rate of Weight Loss and Weight Outcomes
Mean participant weight changes from baseline to 6 months for the FAST, MODERATE, and SLOW weight loss groups were −13.5, −8.9, and −5.1 kg, respectively (Table 2). The assumption of homogeneity of variances and covariances was met and error variance was not significantly different among the dependent variables, therefore Wilk’s Lambda was used in the following analyses. A repeated measures analysis of covariance using residualized change scores for weight change showed a significant interaction effect for time and weight loss group, F(4,514) =16.2, p <0.001, partial η2 = 0.11. There was no significant effect for ethnicity, p = 0.174. Bonferroni-adjusted post-hoc tests found that between baseline and 6 months the FAST group lost significantly more weight than the MODERATE group, t(258)=−5.0, p<0.001, and the SLOW group, t(258)= −8.2, p < 0.001, and the MODERATE group lost significantly more weight than the SLOW group, t(258) = −3.9, p <0.001. Weight regain did not differ between groups from 6 to 18 months (2.6, 1.8, and 1.3 kg, respectively, all ps <0.9, Table 2). Specifically, despite the greater magnitude of weight loss experienced by participants in the FAST group from baseline to 6 months, they did not regain more weight than participants in the other groups from 6 to 18 months. Finally, when looking at change from baseline to 18 months, including both Phase I and Phase II of the project, weight changes in the FAST, MODERATE, and SLOW groups were −10.9, −7.1, and −3.7 kg, respectively (Table 2). Participants in the FAST group lost significantly more weight than the SLOW group t(258) = −4.2, p<0.001; however, the FAST group did not differ significantly from the MODERATE group, and the MODERATE group did not differ significantly from the SLOW group (ps <0.05). Figure 1 illustrates the weight changes by group across 0, 6, and 18 months.
Table 2.
Weight loss according to rate of weight loss category
| FAST | MODERATE | SLOW | ||||
|---|---|---|---|---|---|---|
| M (kg) | SD | M (kg) | SD | M (kg) | SD | |
| Baseline to 6 months | −13.5a | 5.6 | −8.9a | 4.5 | −5.1 | 4.5 |
| 6 to 18 months | 2.6 | 6.8 | 1.8 | 5.7 | 1.3 | 5.4 |
| Basline to 18 months | −10.9a | 8.3 | −7.1 | 8.0 | −3.8 | 7.5 |
From baseline to 6 months both the FAST and MODERATE groups lost significantly greater weight than the SLOW group (all ps<0.001). From baseline to 18 months the FAST group lost significantly greater weight than the SLOW group (p<0.001)
Fig. 1.
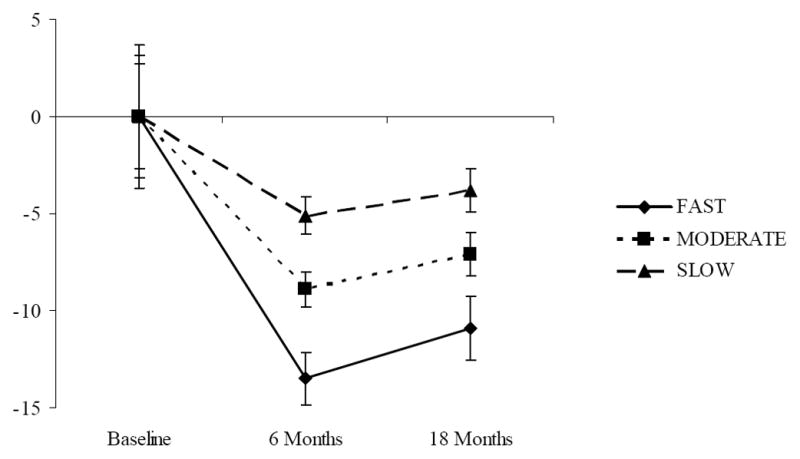
Body weight change (mean ± SE) according to rate of weight loss category
Maintenance of a Clinically Significant Weight Loss at 18 Months
At 18 months, 50.7% of participants in the FAST group, 35.6% of participants in the MODERATE group, and 16.9% of participants in the SLOW group maintained a clinically significant 10% reduction in body weight. A Pearson’s chi-square showed that weight loss group was significantly associated with maintenance of a 10% weight loss at 18 months, χ2 (2, N = 262) = 20.5, p <0.001, Cramer’s V = 0.28, such that the FAST group was significantly more likely to maintain a 10% weight loss than participants in the MODERATE group, χ2 (1, N = 173) =3.9, p =0.048, Cramer’s V = 0.15, and participants in the SLOW group, χ2 (1, N = 158) =20.6, p <0.001, Cramer’s V =0.36. Furthermore, the MODERATE group was significantly more likely to maintain a 10% weight loss than participants in the SLOW group, χ2 (1, N =193)=8.5, p=0.003, Cramer’sV=0.21.
Those who lost weight at a FAST rate within the first month of behavioral treatment were 5.1 times more likely to achieve successful weight loss maintenance at 18 months than those who lost at a SLOW rate. Those who were categorized as MODERATE were 2.7 times more likely to attain a 10% reduction at 18-months than those in the SLOW group.
Secondary Outcomes
The assumption of homogeneity of variances and covariances was not met, F(20,190384.3) =6.3, p <0.001, and error variance was significantly different between groups for attendance, F(2,256) =13.8, p < 0.001, and adherence, F (2,256) =44.4, p <0.001, therefore Pillai’s Trace, a conservative F-approximation, was used in the following analysis. A significant main effect was found for weight loss groups, F(8,508) =5.1, p <0.001, η2 = 0.07, such that attendance, adherence, caloric intake, and physical activity during the first month of treatment varied by weight loss group. Specifically, participants in the FAST group attended significantly more sessions than participants in the SLOW group, t(256) = 2.7, p = 0.025, completed significantly more food records, t(256) =4.7, p <0.001, and consumed significantly fewer calories, t(256) = −2.6, p =0.034. Participants in the MODERATE group also completed significantly more food records, t(256) =4.2, p < 0.001, and walked significantly more steps per day, t(256) =2.8, p =0.014, than participants in the SLOW group. There were no significant differences between the FAST and MODERATE groups in terms of first-month attendance, adherence, daily average calories consumed, or daily average steps (Table 3).
Table 3.
Attendance, adherence, caloric intake, and step count after 1 month of treatment according to rate of weight loss category
| FAST | MODERATE | SLOW | ||||
|---|---|---|---|---|---|---|
| MD | SD | M | SD | M | SD | |
| Attendance | 3.9a | 0.3 | 3.8 | 0.5 | 3.6 | 0.5 |
| Adherence | 20.4a | 2.1 | 20.0 | 2.4 | 17.4 | 4.0 |
| Caloric intake | 1,366.4a | 238.9 | 1,387.6a | 223.1 | 1,486.8 | 295.4 |
| Step count | 4,571.3 | 2,222.6 | 4,877.0a | 2,320.3 | 3,975.8 | 2,200.8 |
Compared to the SLOW group, the FAST group attended significantly more sessions (p<0.05), completed more food records (p<0.001), and consumed fewer calories (p<0.05). Compared to the SLOW group, the MODERATE group consumed fewer calories (p<0.001) and walked more steps (p<0.05)
Discussion
There were three key findings with regards to weight outcomes. First, women who lost weight at a FAST rate during the first 4 weeks of treatment achieved significantly greater weight reductions at 6 months than those who lost at MODERATE and SLOW rates, and those who lost at a MODERATE rate during the first 4 weeks of treatment lost significantly more weight than those who lost at a SLOW rate. At 18 months, the FAST group maintained a significantly greater weight loss than the SLOW group. These findings are consistent with previous research demonstrating that larger initial weight losses are associated with greater long-term weight loss success [10, 12–15, 21, 30].
Second, no significant differences between groups were observed in terms of weight regain. Contrary to previous research [15, 17], participants in the present study who lost at a greater initial rate did not experience greater amounts of weight regain post-treatment than those who lost at a slower initial rate.
Third, the FAST and MODERATE group were 5.1 and 2.7 times, respectively, more likely to achieve successful and beneficial weight loss maintenance of 10% body weight reduction at 18-months follow-up than the SLOW group. Only 16.9% of the SLOW group attained this successful 10% weight loss in the year following active behavioral treatment compared to 35.6% of the MODERATE group and 50.7% of the FAST group.
Taken together, these results suggest that losing weight at a slow initial rate does not lead to greater long-term weight loss and smaller weight regain. From a learning theory perspective, it may be argued that losing at a slow initial rate may be less reinforcing to participants than losing at a moderate or fast initial rate. Indeed, participants who reduced weight at a fast rate lost significantly more weight and maintained this loss at an 18-months follow-up. Carels et al. [13] showed that improvement in quality of life factors (e.g., general appearance, body image, physical mobility, energy, and perceived health) during the first 4 weeks of a weight control program were associated with greater weight reductions at end of treatment. Large initial weight losses and the related positive quality of life changes may serve as reinforcers, increasing healthy behaviors and healthy habit learning. This in turn may lead to successful weight loss and maintenance. Similarly, participants in the present study who lost at fast initial rates made more positive behavioral changes initially than those who lost at slower rates (i.e., greater attendance and adherence rates and lower calorie consumption). Conversely, unsatisfactory early weight loss has been associated with poor treatment outcomes [13]. This suggests that when the shaping of healthy behavior occurs very slowly, the ensuing small weight changes may not provide sufficient reinforcement to promote learning and long-term habit change.
Weight regains in this study did not significantly differ across FAST, MODERATE, and SLOW groups. A potential explanation of these findings could be the study design. Specifically, TOURS incorporated a year-long extended care regimen during which participants received continuing contact twice per month from their intervention group leaders in the form of group sessions, telephone contact, or newsletters [25]. Studies that have found associations between greater initial weight loss and subsequent larger and more rapid weight regain have not employed continuing contact past the initial intervention in their study designs [15, 17, 22]. Extended care has been shown to enhance long-term progress [4], and it is believed that continuing contact may provide the “overlearning” that is necessary for long-term habit changes to become fully ingrained for long-term weight loss success [31]. Because those who lose larger amounts of weight are often more susceptible to regain [2, 23, 24], our results suggest that “overlearning” of habit changes through extended care may be necessary to enhance the maintenance of initial weight losses. In addition, the present study utilized a larger sample size than previous trials of its kind [12, 13, 15, 17, 22] and exhibited a low attrition rate, which contribute to the uniqueness of these findings.
There are three potential limitations to the present study. First, this study used a correlational design and thus cannot directly assess causality. This post-hoc separation of groups according to initial rate of weight loss did not account for underlying physiology or behaviors that may have self-selected participants into each group and determined long-term outcomes. Future studies employing a prospective, randomized design to assign participants to the FAST, MODERATE, and SLOW weight loss categories are necessary to validate our findings regarding initial rate of weight loss. Our results are consistent with previous studies that indicate a greater initial rate of weight loss leads to long-term success [10, 12–15, 21, 30]; however, prescribing faster initial rates of weight loss may not always produce better long-term outcomes. Studies of very-low-calorie diets (VLCD, i.e., 500–800 kcal/day) have shown that participants randomized to VLCDs have greater initial losses but experience larger weight regains and no relative long-term advantage compared to participants randomized to standard behavioral treatment with low-calorie diets (i.e., 800–1,200 kcal/day) [22, 32]. Weight regain in these studies was much larger for participants in the VLCD groups; thus there were no long-term benefits of the initial fast weight losses [22, 32]. These results suggest that utilizing very-low-calorie diets (<800 kcal/day) to attain fast initial weight losses may not lead to successful long-term weight maintenance. All participants in the TOURS study were prescribed a 1,200 kcal/day diet and provided extended care to promote maintenance of weight loss. Results suggest that a faster rate of weight loss is superior; however, it remains unclear whether prospectively prescribing various calorie levels to promote fast or slow initial rates of weight loss would result in similar weight maintenance outcomes.
Second, reinforcing consequences, such as change in physical appearance, improvement in body image, increased energy, and perceived enhancement of health within the first month of behavioral treatment have previously been linked to long-term weight loss success [13], but were not measured in the present study. Therefore, it is not possible to separate these additional factors that may affect weight loss within the first month of behavioral treatment from rate of weight loss. Finally, the study sample was comprised of relatively healthy middle-aged and older obese women. Generalizability to treatment of men and younger women as well as those with serious health conditions is unknown. Future studies prospectively assigning initial rates of weight loss in diverse population samples, while assessing modalities of achieving this weight loss, are warranted.
In conclusion, this study further provides evidence that, within the context of lifestyle treatment where women are encouraged to consume 1,200 kcal/day, losing weight at a fast initial rate leads to greater short-term weight reductions, does not result in increased susceptibility to weight regain, and is associated with larger weight losses and overall long-term success in weight management. It is therefore suggested that, within lifestyle weight control programs, substantial efforts be focused on promoting large rather than small behavioral changes during the initial weeks of treatment.
Acknowledgments
This research was supported by grant R18HL073326 from the National Heart, Lung, and Blood Institute.
Footnotes
ClinicalTrials.gov NCT00201006.
Disclosure: The authors declare no conflict of interest.
Contributor Information
Lisa M. Nackers, Email: lnackers@phhp.ufl.edu, Department of Clinical and Health Psychology, University of Florida, PO Box 100165, Gainesville, FL 32610-0165, USA
Kathryn M. Ross, Department of Clinical and Health Psychology, University of Florida, PO Box 100165, Gainesville, FL 32610-0165, USA
Michael G. Perri, Department of Clinical and Health Psychology, University of Florida, PO Box 100165, Gainesville, FL 32610-0165, USA
References
- 1.National Heart, Lung and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Obes Res. 1998;6:51S–209. [PubMed] [Google Scholar]
- 2.Wing RR, Hill JO. Successful weight loss maintenance. Annu Rev Nutr. 2001;21:323–41. doi: 10.1146/annurev.nutr.21.1.323. [DOI] [PubMed] [Google Scholar]
- 3.Jeffery RW, Epstein LH, Wilson GT, Drewnowski A, Stunkard AJ, Wing RR. Long-term maintenance of weight loss: current status. Health Psychol. 2000;19 (Suppl 1):5–16. doi: 10.1037/0278-6133.19.suppl1.5. [DOI] [PubMed] [Google Scholar]
- 4.Perri MG, Fuller PR. Success and failure in the treatment of obesity: where do we go from here? Med Exerc Nutr Health. 1995;4:255–72. [Google Scholar]
- 5.Wadden TA, Butryn ML, Byrne KJ. Efficacy of lifestyle modification for long-term weight control. Obes Res. 2004;12:151S–62. doi: 10.1038/oby.2004.282. [DOI] [PubMed] [Google Scholar]
- 6.Perri MG. The maintenance of treatment effects in the long-term management of obesity. Clin Psychol: Sci Pract. 1998;5:526–43. [Google Scholar]
- 7.Klein S. Outcome success in obesity. Obes Res. 2001;9:354S–8. doi: 10.1038/oby.2001.142. [DOI] [PubMed] [Google Scholar]
- 8.Krebs JD, Evans S, Cooney L, et al. Changes in risk factors for cardiovascular disease with body fat loss in obese women. Diab Obes Metab. 2002;4:379–87. doi: 10.1046/j.1463-1326.2002.00231.x. [DOI] [PubMed] [Google Scholar]
- 9.Moore LL, Visioni JJ, Wilson PW, D’Agostino RB, Finkle WD, Ellison RC. Can sustained weight loss in overweight individuals reduce the risk of diabetes mellitus? Epidemiology. 2000;11:269–73. doi: 10.1097/00001648-200005000-00007. [DOI] [PubMed] [Google Scholar]
- 10.Elfhag K, Rössner S. Who succeeds in maintaining weight loss? A conceptual review of factors associated with weight loss maintenance and weight regain. Obes Rev. 2005;6:67–85. doi: 10.1111/j.1467-789X.2005.00170.x. [DOI] [PubMed] [Google Scholar]
- 11.Vogels N, Diepvens K, Westerterp-Plantenga MS. Predictors of long-term weight maintenance. Obes Res. 2005;13:2162–8. doi: 10.1038/oby.2005.268. [DOI] [PubMed] [Google Scholar]
- 12.Wadden TA, Foster GD, Wang J, et al. Clinical correlates of short- and long-term weight loss. Am J Clin Nutr. 1992;56:271S–4. doi: 10.1093/ajcn/56.1.271S. [DOI] [PubMed] [Google Scholar]
- 13.Carels RA, Cacciapaglia HM, Douglass OM, Rydin S, O’Brien WH. The early identification of poor treatment outcome in a women’s weight loss program. Eat Behav. 2003;4:265–82. doi: 10.1016/S1471-0153(03)00029-1. [DOI] [PubMed] [Google Scholar]
- 14.Fogelholm M, Kukkonen-Harjula K, Oja P. Eating control and physical activity as determinants of short-term weight maintenance after a very-low-calorie diet among obese women. Int J Obes. 1999;23:203–10. doi: 10.1038/sj.ijo.0800825. [DOI] [PubMed] [Google Scholar]
- 15.Jeffery RW, Wing RR, Mayer RR. Are smaller weight losses or more achievable weight loss goals better in the long term for obese patients? J Consult Clin Psychol. 1998;66:641–5. doi: 10.1037//0022-006x.66.4.641. [DOI] [PubMed] [Google Scholar]
- 16.Lutes LD, Winett RA, Barger SD, et al. Small changes in nutrition and physical activity promote weight loss and maintenance: 3-month evidence from the ASPIRE randomized trial. Ann Behav Med. 2008;35:351–7. doi: 10.1007/s12160-008-9033-z. [DOI] [PubMed] [Google Scholar]
- 17.Sbrocco T, Nedegaard RC, Stone JM, Lewis EL. Behavioral choice treatment promotes continuing weight loss: preliminary results of a cognitive-behavioral decision-based treatment for obesity. J Consult Clin Psychol. 1999;67:260–6. doi: 10.1037//0022-006x.67.2.260. [DOI] [PubMed] [Google Scholar]
- 18.Kumanyika SK, Espeland MA, Bahnson JL, et al. Ethnic comparison of weight loss in the trial of nonpharmacologic interventions in the elderly. Obes Res. 2002;10:96–106. doi: 10.1038/oby.2002.16. [DOI] [PubMed] [Google Scholar]
- 19.Stevens VJ, Obarzanek E, Cook NR, et al. Long-term weight loss and changes in blood pressure: results of the trials of hypertension prevention, phase II. Ann Intern Med. 2001;134:1–11. doi: 10.7326/0003-4819-134-1-200101020-00007. [DOI] [PubMed] [Google Scholar]
- 20.Wassertheil-Smoller S, Langford HG, Blaufox MD, et al. Effective dietary intervention in hypertensives: sodium restriction and weight reduction. J Am Diet Assoc. 1985;85:423–30. [PubMed] [Google Scholar]
- 21.Astrup A, Rössner S. Lessons from obesity management programmes: greater initial weight loss improves long-term maintenance. Obes Rev. 2000;1:17–9. doi: 10.1046/j.1467-789x.2000.00004.x. [DOI] [PubMed] [Google Scholar]
- 22.Wadden TA, Foster GD, Letizia KA. One-year behavioral treatment of obesity: comparison of moderate and severe caloric restriction and the effects of weight maintenance therapy. J Consult Clin Psychol. 1994;62:165–71. doi: 10.1037//0022-006x.62.1.165. [DOI] [PubMed] [Google Scholar]
- 23.McGuire MT, Wing RR, Klem ML, Lang W, Hill JO. What predicts weight regain in a group of successful weight losers? J Consult Clin Psychol. 1999;67:177–85. doi: 10.1037//0022-006x.67.2.177. [DOI] [PubMed] [Google Scholar]
- 24.Weiss EC, Galuska DA, Kettel Khan L, Gillespie C, Serdula MK. Weight regain in U.S. adults who experienced substantial weight loss; 1999–2002. Am J Prev Med. 2007;33:34–40. doi: 10.1016/j.amepre.2007.02.040. [DOI] [PubMed] [Google Scholar]
- 25.Perri MG, Limacher MC, Durning PE, et al. Extended-care programs for weight management in rural communities: the treatment of obesity in underserved rural settings (TOURS) randomized trial. Arch Intern Med. 2008;168:2347–54. doi: 10.1001/archinte.168.21.2347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Perri MG, Corsica JA. Improving the maintenance of weight lost in behavioral treatment of obesity. In: Wadden TA, Stunkard AJ, editors. Handbook of obesity treatment. New York: Guilford Press; 2001. pp. 357–79. [Google Scholar]
- 27.Jeffery RW, Drewnowski A, Epstein LH, et al. Long-term maintenance of weight loss: current status. Health Psychol. 2008;19:5–16. doi: 10.1037/0278-6133.19.suppl1.5. [DOI] [PubMed] [Google Scholar]
- 28.Wadden TA, Berkowitz RJ, Sarwer DB, Prus-Wisniewski R, Steinberg C. Benefits of lifestyle modification in the pharmacologic treatment of obesity. Arch Intern Med. 2001;161:218–27. doi: 10.1001/archinte.161.2.218. [DOI] [PubMed] [Google Scholar]
- 29.Wadden TA, Berkowitz RI, Womble LG, et al. Randomized trial of lifestyle modification and pharmacotherapy for obesity. N Engl J Med. 2005;353:2111–20. doi: 10.1056/NEJMoa050156. [DOI] [PubMed] [Google Scholar]
- 30.Stotland SC, Larocque M. Early treatment response as a predictor of ongoing weight loss in obesity treatment. Br J Health Psychol. 2005;10:601–14. doi: 10.1348/135910705X43750. [DOI] [PubMed] [Google Scholar]
- 31.Latner JD, Stunkard AJ, Wilson GT, Jackson ML, Zelitch DS, Labouvie E. Effective long-term treatment of obesity: a continuing care model. Int J Obes. 2000;24:893–8. doi: 10.1038/sj.ijo.0801249. [DOI] [PubMed] [Google Scholar]
- 32.Toubro S, Astrup A. Randomised comparison of diets for maintaining obese subjects’ weight after major weight loss: ad lib, low fat, high carbohydrate diet v fixed energy intake. Br Med J. 1997;4:314–29. doi: 10.1136/bmj.314.7073.29. [DOI] [PMC free article] [PubMed] [Google Scholar]