

Abstract
OBJECTIVE
To investigate the risk of acute myocardial infarction (AMI) following stress hyperglycemia after hip fracture.
RESEARCH DESIGN AND METHODS
From February 2007 to February 2012, we carried out a prospective observational analysis of 1,257 consecutive patients with no history of diabetes who suffered hip fractures. Fasting blood glucose (FBG) and glycosylated hemoglobin tests as well as electrocardiography, ultrasonic cardiography, and chest X-ray examinations were performed after admission. All selected hip fracture patients were divided into stress hyperglycemia and non-hyperglycemia groups according to their FBG, and the incidence of AMI was monitored.
RESULTS
Among the patients enrolled, the frequency of stress hyperglycemia was 47.89% (602/1,257) and that of AMI was 9.31% (117/1,257), and the occurrence of AMI in the stress hyperglycemia group was higher than in the non-hyperglycemia group (12.46 vs. 6.41%, P < 0.05). In the stress hyperglycemia patients, FBG reached maximum levels at 2–3 days after hip fractures and then decreased gradually. The AMI incidence (62.67% [47/75]) of the stress hyperglycemia group was highest in the initial 3 days after hip fracture, significantly coinciding with the FBG peak time (P < 0.05). In all patients with AMI, non–ST-segment elevation myocardial infarction occurred more often than ST-segment elevation myocardial infarction (62.39% [73/117] vs. 37.61% [44/117]).
CONCLUSIONS
Stress-induced hyperglycemia after hip fracture increased the risk of AMI.
With prolonged life span, there is an increasing number of elderly people with aging-related degenerative diseases. Hip fracture is a main complication of osteoporosis among aged patients (1), and prevention of hip fracture–related complications has become increasingly important, mainly focusing on diagnosis and therapy of pulmonary embolism and bronchopneumonia. On the other hand, the risk of acute myocardial infarction (AMI) after hip fractures is not well recognized and has not been given its deserved attention (2), because adverse cardiovascular events were one of the main reasons for an increased mortality risk after hip fracture (3). Besides, research has confirmed an association between risk of cardiovascular events and osteoporosis in older men (4). Hip fractures lead to injuries of the musculoskeletal system and induce a stress state simultaneously, thereby stimulating the release of stress hormones and reducing insulin sensitivity through neuroendocrine changes. As a result, a derangement of glucose metabolism and occurrence of stress hyperglycemia is triggered (5,6), but at present, the epidemiology of stress hyperglycemia is not clear (7). There are conflicting opinions about the disadvantages and influence as well as treatments of stress hyperglycemia, and only a little information is available about the risk of AMI following stress hyperglycemia after hip fractures (8,9). We conducted a prospective clinical observation of the relationship between stress-induced hyperglycemia and AMI in nondiabetic patients who were hospitalized with acute hip fractures in our hospital.
RESEARCH DESIGN AND METHODS
Patient selection
We performed a prospective observational study at the Tianjin Hospital. Consecutive hip fracture patients (n = 1,257) were selected for the analysis during a 5-year period from February 2007 to February 2012. The study protocol was approved by the Tianjin Hospital ethics committee, and informed consent of all patients was obtained. The inclusion criteria were 1) the injury time of hip fractures was <24 h before admission and fracture diagnosis by X-ray examinations in our emergency department, 2) patient participated in physical examinations each year and blood glucose was normal (<6.1 mmol/L) with ordinary values of glycosylated hemoglobin (HbA1c), 3) a pair of lower limb venous vascular ultrasound examinations confirmed no deep venous thromboembolism (DVT), 4) osteoporosis was confirmed by bone density examination, and 5) orthopedic surgery was not completed within 1 week after admission to the hospital or no operation was performed (conservative treatment). The exclusion criteria were 1) the time of hip fracture injury was >24 h before admission; 2) diagnosed type 1 or type 2 diabetes; 3) need of emergency operation within 1 week after hip fracture; 4) the occurrence of DVT, pulmonary embolism, or thyroid disease; and 5) renal/liver failure.
Procedures
Blood and urine routine, liver and kidney function, calcium, phosphorus, and serum cardiac enzyme concentrations, insulin level, and serum lipids were tested after admission. Electrocardiography (ECG), cardiorespiratory function test, ultrasonic cardiography, chest X-ray, lower limb venous vascular ultrasound, and bone mineral density measurements of the bilateral hip were conducted. Closed reduction, bone traction treatments, and prevention of DVT were administered to all patients with hip fractures on the day of admission (10) and they continued to take their cardiac medications. All patients who met the inclusion criteria were recorded with a standardized form throughout the study course. The fasting blood glucose (FBG) was examined at 6:00 a.m. every morning from the 1st to the 7th day after admission, and ECGs were measured at admission and from the 1st to the 7th day after admission at 10:00 a.m. every morning. If clinical symptoms indicated and/or electrocardiographic changes suggested a myocardial infarction, additional blood samples were drawn from the antecubital vein in order to examine creatine kinase (CK), CK-MB isoenzyme, and troponin-I values. AMI diagnosis met ST-segment elevation myocardial infarction (STEMI) or non–ST-segment elevation myocardial infarction (NSTEMI) criteria (11,12). AMI diagnosis criteria met at least two of following: 1) the CK-MB isoenzyme and/or troponin-I concentration elevated above the hospital laboratory's myocardial infarction threshold; 2) persistent ST-T segment changes, new Q waves, or left bundle branch block occurred; 3) serious precordial chest pain lasting for 30 min or more. Stress hyperglycemia diagnosis criteria were as follows: 1) patients did not have a previous diabetes history, 2) admission or in-hospital fasting plasma glucose levels of 7 mmol/L or more in two or more tests (13), and 3) normal HbA1c values.
Statistical analyses
SPSS 17.0 (SPSS, Inc., Chicago, IL) software was applied by a professional statistician to complete the analyses. Continuous variables were expressed as mean with SD. Comparisons between continuous variables were performed using the Student t test or ANOVA. Categorical variables were expressed as frequency and percentage. Comparisons between categorical variables were compared using the χ2 test or Fisher exact test. Multiple logistic regression analysis identified risk factors of AMI. P value ≤0.05 was considered statistically significant.
Clinical follow-up
The period of follow-up interviews was 3 months after discharge, and mortality was recorded by the investigators via telephone calls and/or outpatient clinic visits.
RESULTS
Patients (n = 1,257) who met the inclusion criteria were enrolled in this clinical observation. Among the patients, the average age was 75.20 ± 7.71 years and 64.52% were women. The most prevalent comorbidity was hypertension (57.68%), followed by coronary artery disease (CAD) or family history of CAD (49.90%), dyslipidemia (elevation of LDL cholesterol [LDL-C], 49.27%; triglyceride, 39.14%; and low levels of HDL cholesterol [HDL-C], 21.40%), obesity (37.63%), and smoking (28.16%).
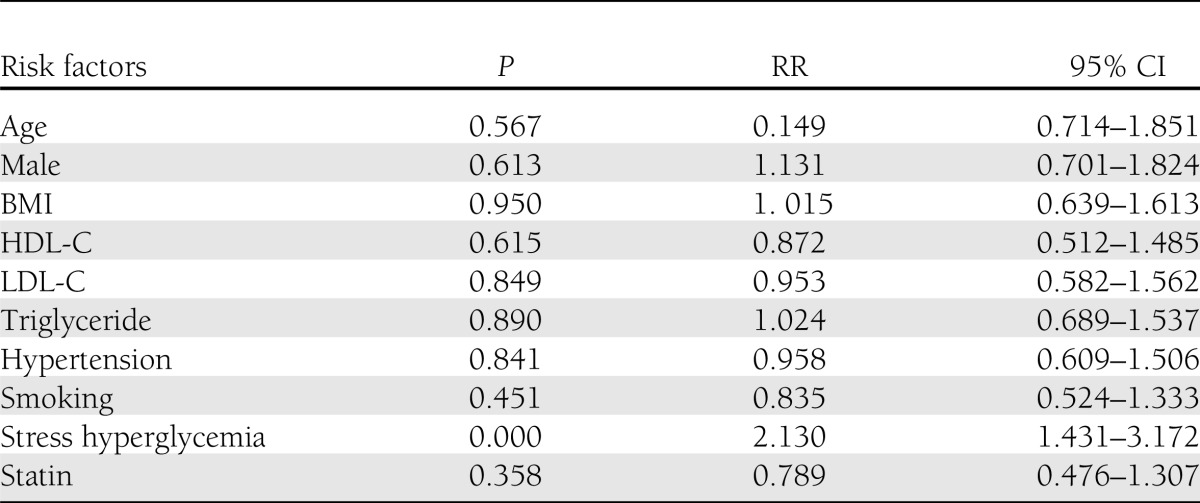
The frequency of stress hyperglycemia was 47.89% (602/1,257) and that of AMI was 9.31% (117/1,257). Table 1 shows the basic characteristics of the selected patients. There was a significant difference in admission glucose levels between the two groups. Figure 1 shows the correlation between time of fracture and FBG. In the stress hyperglycemia group, FBG values reached a maximum 2–3 days after hip fracture and then decreased gradually. Repeated ANOVAs showed that at each time point in the stress hyperglycemia group, the blood glucose values were significantly different (P < 0.05), whereas in the non-hyperglycemia patients, they did not change (P = 0.10) (Fig. 1). Table 2 shows characteristics of myocardial infarctions in the two groups. The incidence of AMI in the stress hyperglycemia group was significantly higher (12.46% [75/602]) than in the non-hyperglycemia group (6.41% [42/655], P < 0.05). The number of AMIs was correlated with the occurrence of hyperglycemia and was significantly higher ≤3 days after injury in the hyperglycemia group (P < 0.05), whereas the temporal distribution of AMI in the non-hyperglycemia group was not different between ≤3 and >3 days after injury (Table 2). In all patients with AMI, NSTEMI events occurred more often than STEMI (62.39% [73/117] vs. 37.61% [44/117]), but STEMI significantly prevailed in the stress hyperglycemia group (P < 0.05). In Table 3, risk factors for AMI and their significance are listed. A multiple logistic regression analysis using a forward stepwise (conditional) method revealed that stress hyperglycemia is an independent risk factor for the development of AMI (relative risk [RR] 2.130 [95% CI 1.431–3.172]). Patients with stress hyperglycemia after hip fracture were 2.130-fold more likely to develop an AMI than the non-hyperglycemia individuals.
Table 1.
Basic characteristics of the selected patients
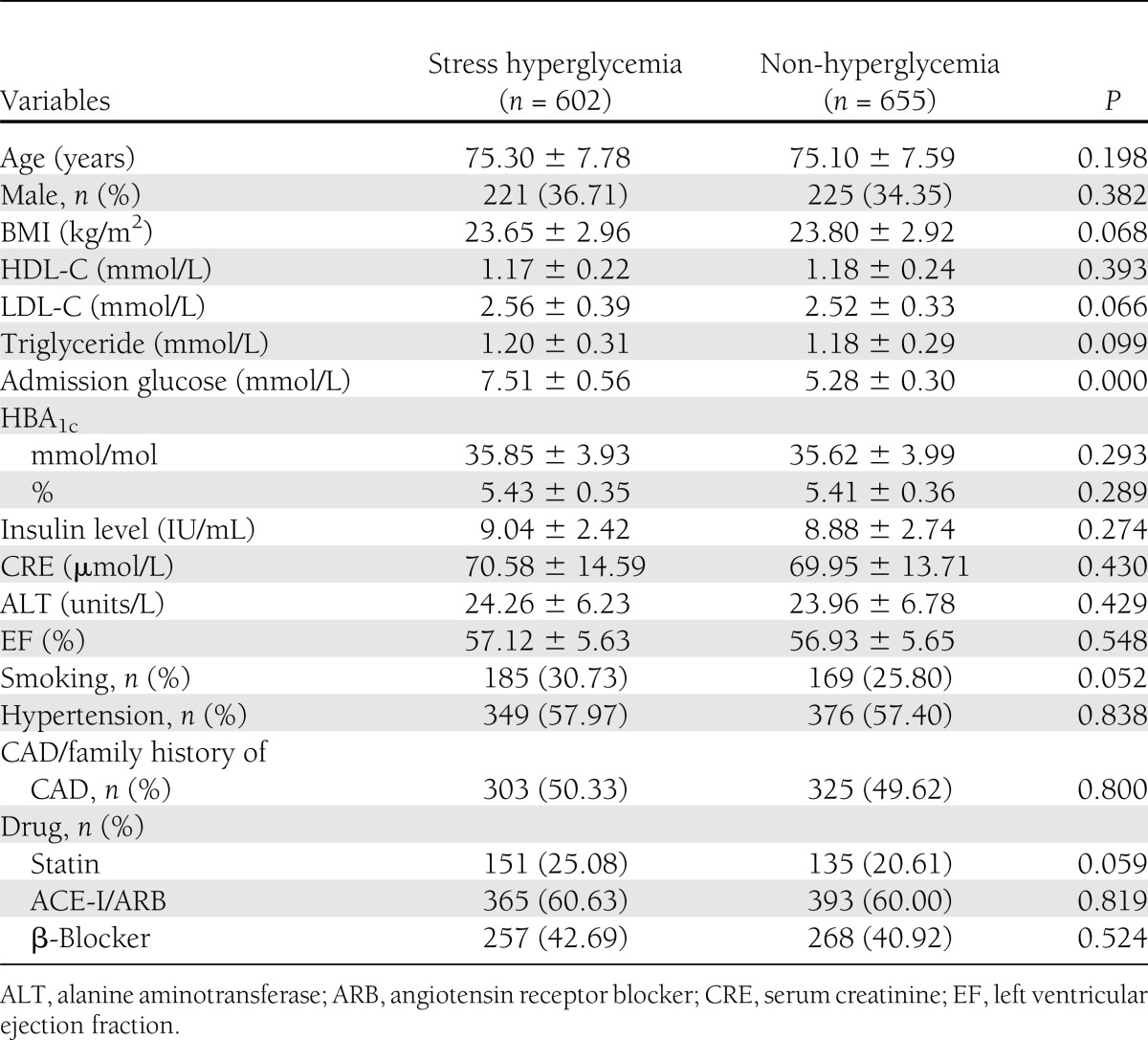
Figure 1.

Correlation between the days after fracture and FBG.
Table 2.
Characteristics of myocardial infarction in the two groups
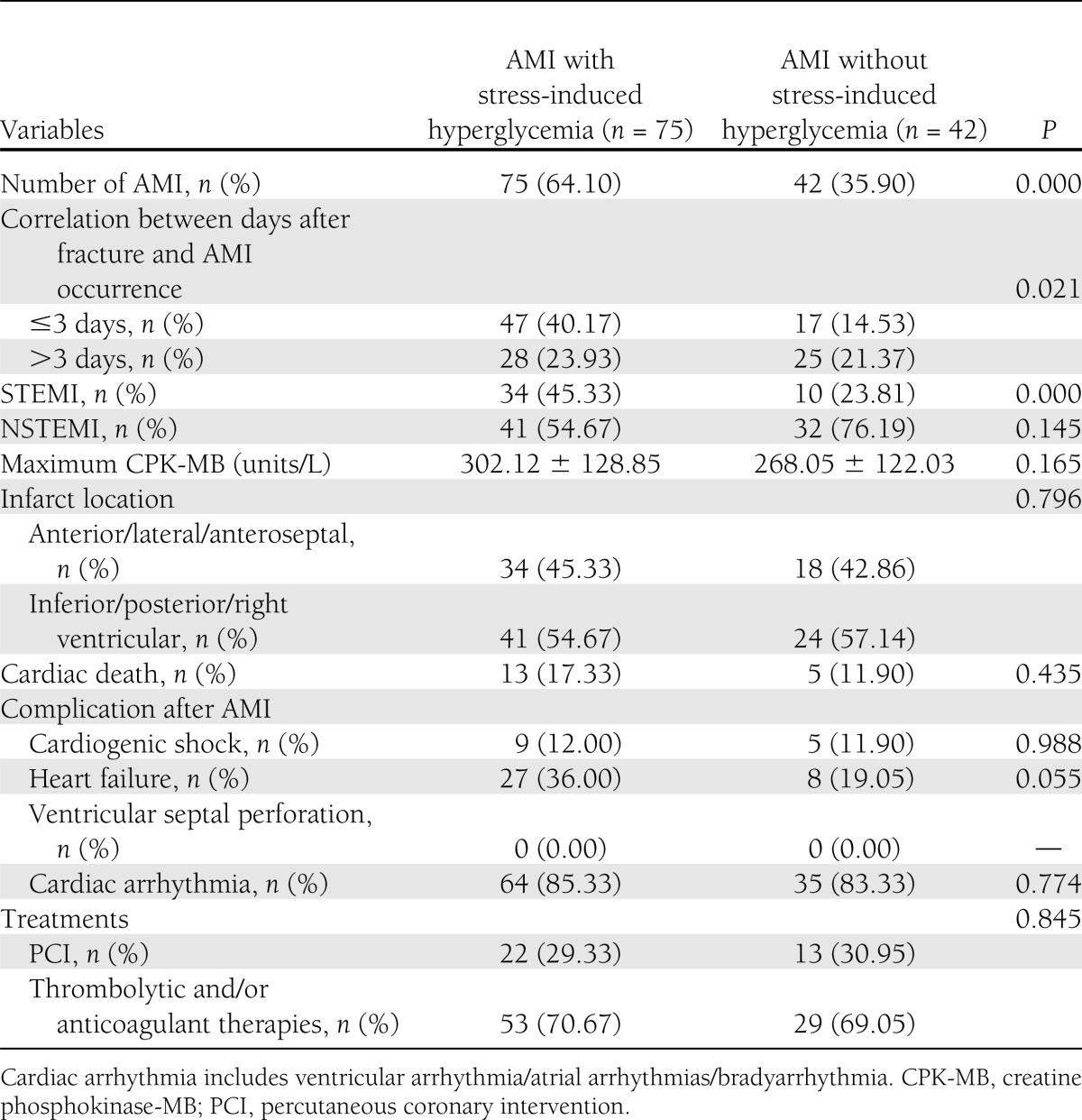
Table 3.
Risk factors of AMI
At the end of 3 months follow-up, there were no differences in mortality in patients with versus without stress-induced hyperglycemia (6.98% [42/602] vs. 4.43% [29/655], P = 0.051).
CONCLUSIONS
In our study, we found that the frequency of stress hyperglycemia was 47.89% and the incidence of AMI was 9.31% in patients after hip fractures. The incidence of AMI in the stress hyperglycemia group was 12.46%, whereas the overall AMI incidence in patients without hip fractures in China is 2.6% (14), indicating that the incidence of AMI in patients after hip fractures appears higher than overall AMI incidence in China.
Others have reported that the increased incidence of AMI after hip fracture was related to osteoporosis (4,14). Osteoporosis and cardiovascular diseases share common risk factors like poor general health status, lifestyle, nutrition, hormone secretion, vitamin D deficiency, systemic inflammation-related (e.g., C-reactive protein, interleukin-6, or tumor necrosis factor) diseases, and medications through different mechanisms both in bone and arteries (15–25).
Patients with osteoporotic fractures are likely to have coexisting blood vessel diseases, but in our study, we found that particularly stress hyperglycemia plays a vital role, because the incidence of AMI in the stress hyperglycemia group was 2.130 higher than in the non-hyperglycemia group. In patients with hip fractures, stress hyperglycemia was the sole significant independent risk factor for the development of AMI (95% CI 1.431–3.172).
Acute fractures induce stress hormone secretion of glucocorticoid, glucagon, adrenaline, thyroxin, somatotropin, and others, which is called the “stress response.” During the stress response, activation of serial hormones induces insulin resistance, resulting in hyperglycemia and the associated risk factors present then in patients with acute traumata (26). It is well known that stress hyperglycemia is associated with oxidative stress, inflammatory responses, damaging of coronary microcirculation, and markedly worsened signal transduction pathways of endogenous cardioprotective responses. Hyperglycemia can induce ADP-induced platelet aggregation and increase plasma catecholamine, which is associated with vulnerable plaque evolution, the promotion of microcircular dysfunctions, and thrombogenesis (27–37).
Our present work indicates that for patients without a history of diabetes, stress-induced hyperglycemia plays a key role in the risk of developing AMI. Our present analysis revealed that most (62.67% [47/75]) AMIs occurred within the first 3 days after hip fractures, which is in accordance with the literature (2). In the stress hyperglycemia group, blood glucose peaked at 2–3 days after hip fracture and then declined gradually, indicating a coincidence of AMI with the peak time of FBG. The cause of a more frequent STEMI occurrence in stress-induced hyperglycemia might be that raised glucose levels contribute to platelet activation and thereby enhanced platelet-mediated thrombogenesis (38), which develops into completely occlusive thrombi. In addition, our study showed stress hyperglycemia ranges of 6.1–9.7 mmol/L after hip fractures for the first time, and we recommend that stress-induced hyperglycemias after hip fracture should be identified early.
A limitation of our study was that we did not investigate an effect of inflammatory factors and/or stress hormones on FBG levels, which lead to increased AMI risk. In addition, we did not compare the results of this study with patients suffering from diabetes, and we did not find differences between the stress hyperglycemia and no hyperglycemia groups regarding comorbid disorders and/or drug administrations, e.g., statin against hypertension. Therefore we cannot completely rule out that other factors also contributed to the incidence of myocardial infarctions. Moreover, patients were not accurately diagnosed for diabetes in the longer term, and because blood glucose levels largely fluctuate, we did not specifically treat the hyperglycemias. Up until now, there has been no clear agreement on whether it is necessary to control glucose levels in these patients. In addition, we only show the significance of hyperglycemia on the incidence of AMI during admission; we did not show clinical outcome data at follow-up. However, this study underlines the importance of understanding the indication for adopting appropriate methods to identify stress-induced hyperglycemia in correlation with AMI after hip fracture.
We recommend that in patients, even without previous diabetes, FBGs and ECGs should be monitored for at least the first 7 days after hip fractures. This might be helpful for the endocrinologist, cardiologist, and orthopedic surgeon to timely detect AMIs.
We conclude that stress-induced hyperglycemia increased the risk of AMI in patients with hip fractures. Stress-induced hyperglycemias after hip fracture should be identified early.
Acknowledgments
No potential conflicts of interest relevant to this article were reported.
Y.C. designed the study, collected the data, and wrote the first draft of the manuscript. X.Y., K.M., and Z.Z. designed the study and reviewed and analyzed the data. B.M. and X.L. conducted the study. B.Q. researched data and analyzed samples. S.C., P.C., and Y.Y. researched data, analyzed samples, and conceived and edited the manuscript. B.Q. is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
The authors thank Dr. Guosheng Xing (Tianjin Hospital, Tianjin, China) who managed the data collection. The authors also thank the people with hip fractures who participated in this study.
References
- 1.Piscitelli P, Iolascon G, Gimigliano F, et al. Osteoporosis and cardiovascular diseases’ cosegregation: epidemiological features. Clin Cases Miner Bone Metab 2008;5:14–18 [PMC free article] [PubMed] [Google Scholar]
- 2.Matot I, Oppenheim-Eden A, Ratrot R, et al. Preoperative cardiac events in elderly patients with hip fracture randomized to epidural or conventional analgesia. Anesthesiology 2003;1:156–163 [DOI] [PubMed] [Google Scholar]
- 3.Bass E, French DD, Bradham DD, Rubenstein LZ. Risk-adjusted mortality rates of elderly veterans with hip fractures. Ann Epidemiol 2007;17:514–519 [DOI] [PubMed] [Google Scholar]
- 4.Szulc P, Samelson EJ, Kiel DP, Delmas PD. Increased bone resorption is associated with increased risk of cardiovascular events in men: the MINOS study. J Bone Miner Res 2009;24:2023–2031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Greisen J, Juhl CB, Grøfte T, Vilstrup H, Jensen TS, Schmitz O. Acute pain induces insulin resistance in humans. Anesthesiology 2001;95:578–584 [DOI] [PubMed] [Google Scholar]
- 6.Laird AM, Miller PR, Kilgo PD, Meredith JW, Chang MC. Relationship of early hyperglycemia to mortality in trauma patients. J Trauma 2004;56:1058–106 [DOI] [PubMed] [Google Scholar]
- 7.Kerby JD, Griffin RL, MacLennan P, Rue LW., 3rd Stress-induced hyperglycemia, not diabetic hyperglycemia, is associated with higher mortality in trauma. Ann Surg 2012;256:446–452 [DOI] [PubMed] [Google Scholar]
- 8.Vogelzang M, Nijboer JM, van der Horst IC, Zijlstra F, ten Duis HJ, Nijsten MW. Hyperglycemia has a stronger relation with outcome in trauma patients than in other critically ill patients. J Trauma 2006;60:873–877; discussion 878–879 [DOI] [PubMed] [Google Scholar]
- 9.Finfer S, Chittock DR, Su SY, et al. NICE-SUGAR Study Investigators Intensive versus conventional glucose control in critically ill patients. N Engl J Med 2009;360:1283–1297 [DOI] [PubMed] [Google Scholar]
- 10.Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126(Suppl.):338S–400S [DOI] [PubMed] [Google Scholar]
- 11.Pollack CV, Jr, Diercks DB, Roe MT, Peterson ED, American College of Cardiology. American Heart Association 2004 American College of Cardiology/American Heart Association guidelines for the management of patients with ST-elevation myocardial infarction: implications for emergency department practice. Ann Emerg Med 2005;45:363–376 [DOI] [PubMed] [Google Scholar]
- 12.Braunwald E, Antman EM, Beasley JW, et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina) ACC/AHA guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction—2002: summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). Circulation 2002;106:1893–1900 [DOI] [PubMed] [Google Scholar]
- 13.Samiullah S, Qasim R, Imran S, Mukhtair J. Frequency of stress hyperglycaemia and its influence on the outcome of patients with spontaneous intracerebral haemorrhage. J Pak Med Assoc 2010;60:660–663 [PubMed] [Google Scholar]
- 14.Chiang CH, Liu CJ, Chen PJ, et al. Hip fracture and risk of acute myocardial infarction: a nationwide study. J Bone Miner Res 2013;28:404–411 [DOI] [PubMed] [Google Scholar]
- 15.Brøndum-Jacobsen P, Benn M, Jensen GB, Nordestgaard BG. 25-Hydroxyvitamin D levels and risk of ischemic heart disease, myocardial infarction, and early death: population-based study and meta-analyses of 18 and 17 studies. Arterioscler Thromb Vasc Biol 2012;32:2794–2802 [DOI] [PubMed] [Google Scholar]
- 16.Wang TJ, Pencina MJ, Booth SL, Jacques PF, Ingelsson E, Lanier K. Vitamin D deficiency and risk of cardiovascular disease. Circulation 2008;117:503–511 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kim BJ, Yu YM, Kim EN, Chung YE, Koh JM, Kim GS. Relationship between serum hsCRP concentration and biochemical bone turnover markers in healthy pre- and postmenopausal women. Clin Endocrinol (Oxf) 2007;67:152–158 [DOI] [PubMed]
- 18.van de Luijtgaarden KM, Voûte MT, Hoeks SE, et al. Vitamin D deficiency may be an independent risk factor for arterial disease. Eur J Vasc Endovasc Surg 2012;44:301–306 [DOI] [PubMed] [Google Scholar]
- 19.Kim BJ, Yu YM, Kim EN, Chung YE, Koh JM, Kim GS. Relationship between serum hsCRP concentration and biochemical bone turnover markers in healthy pre- and postmenopausal women. Clin Endocrinol (Oxf) 2007;67:152–158 [DOI] [PubMed] [Google Scholar]
- 20.Bruunsgaard H. The clinical impact of systemic low-level inflammation in elderly populations. With special reference to cardiovasculatr disease, dementia and mortality. Dan Med Bull 2006;53:285–309 [PubMed] [Google Scholar]
- 21.Vivona N, Bivona G, Noto D, et al. C-reactive protein but not soluble CD40 ligand and homocysteine is associated to common atherosclerotic risk factors in a cohort of coronary artery disease patients. Clin Biochem 2009;42:1713–1718 [DOI] [PubMed] [Google Scholar]
- 22.Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation 2000;101:1767–1772 [DOI] [PubMed] [Google Scholar]
- 23.Cao JJ, Arnold AM, Manolio TA, et al. Association of carotid artery intima-media thickness, plaques, and C-reactive protein with future cardiovascular disease and all-cause mortality: the Cardiovascular Health Study. Circulation 2007;116:32–38 [DOI] [PubMed]
- 24.Magnus JH, Broussard DL. Relationship between bone mineral density and myocardial infarction in US adults. Osteoporos Int 2005;16:2053–2062 [DOI] [PubMed] [Google Scholar]
- 25.Szulc P, Kiel DP, Delmas PD. Calcifications in the abdominal aorta predict fractures in men: MINOS study. J Bone Miner Res 2008;23:95–102 [DOI] [PubMed] [Google Scholar]
- 26.Losser M-R, Damoisel C, Payen D. Bench-to-bedside review: glucose and stress conditions in the intensive care unit. Crit Care 2010;14:231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Bonizzoli M, Zagli G, Lazzeri C, Degl'Innocenti S, Gensini G, Peris A. Early insulin resistance in severe trauma without head injury as outcome predictor? A prospective, monocentric pilot study. Scand J Trauma Resusc Emerg Med 2012;20:69 [DOI] [PMC free article] [PubMed]
- 28.Scognamiglio R, Negut C, de Kreutzenberg SV, Tiengo A, Avogaro A. Effects of different insulin regimes on postprandial myocardial perfusion defects in type 2 diabetic patients. Diabetes Care 2006;29:95–100 [PubMed] [Google Scholar]
- 29.Scognamiglio R, Negut C, De Kreutzenberg SV, Tiengo A, Avogaro A. Postprandial myocardial perfusion in healthy subjects and in type 2 diabetic patients. Circulation 2005;112:179–184 [DOI] [PubMed] [Google Scholar]
- 30.Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation 2002;106:2067–2072 [DOI] [PubMed] [Google Scholar]
- 31.Coutinho M, Gerstein HC, Wang Y, Yusuf S. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 individuals followed for 12.4 years. Diabetes Care 1999;22:233–240 [DOI] [PubMed] [Google Scholar]
- 32.Baird TA, Parsons MW, Phanh T, et al. Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome. Stroke 2003;34:2208–2214 [DOI] [PubMed] [Google Scholar]
- 33.Leigh R, Zaidat OO, Suri MF, et al. Predictors of hyperacute clinical worsening in ischemic stroke patients receiving thrombolytic therapy. Stroke 2004;35:1903–1907 [DOI] [PubMed] [Google Scholar]
- 34.Bonora E, Muggeo M. Postprandial blood glucose as a risk factor for cardiovascular disease in type II diabetes: the epidemiological evidence. Diabetologia 2001;44:2107–2114 [DOI] [PubMed] [Google Scholar]
- 35.Anand SS, Dagenais GR, Mohan V, et al. EpiDREAM Investigators Glucose levels are associated with cardiovascular disease and death in an international cohort of normal glycaemic and dysglycaemic men and women: the EpiDREAM cohort study. Eur J Prev Cardiol 2012;19:755–764 [DOI] [PubMed] [Google Scholar]
- 36.Meigs JB, Nathan DM, D’Agostino RB, Sr, Wilson PW, Framingham Offspring Study Fasting and postchallenge glycemia and cardiovascular disease risk: the Framingham Offspring Study. Diabetes Care 2002;25:1845–1850 [DOI] [PubMed] [Google Scholar]
- 37.Ceriello A. New insights on oxidative stress and diabetic complications may lead to a “causal” antioxidant therapy. Diabetes Care 2003;26:1589–1596 [DOI] [PubMed] [Google Scholar]
- 38.Shechter M, Merz CN, Paul-Labrador MJ, Kaul S. Blood glucose and platelet-dependent thrombosis in patients with coronary artery disease. J Am Coll Cardiol 2000;35:300–307 [DOI] [PubMed] [Google Scholar]