

Abstract
Here, we describe the case of a 62-year old woman who required aortic and mitral valve replacement plus coronary artery bypass grafting. Transoesophageal echocardiogram revealed stenosis of the aortic valve (Ao valve area, 0.9 cm2; PG, 45 mmHg; MG, 25 mmHg) and a diseased calcified mitral valve with stenosis and regurgitation (mitral valve area, 1.1 cm2; MG, 10 mmHg; RV, 25 ml; ERO, 12 mm2). The mitral annulus calcifications were very deep into the left atrium and the left ventricle muscle, around the full annulus circumference. We decided to avoid complete deep mitral annulus decalcification. The left atrium was surgically exposed, and we deployed a 26-mm Edwards SAPIEN XT endovalve through the left atriotomy. To prevent paravalvular leakage, we then used a pericardial patch to close the gap between the endovalve and the calcified mitral annulus. The postoperative echocardiogram showed perfect anchoring of the endovalve in the mitral annulus without any paravalvular leakage.
Keywords: Transcatheter aortic valve implantation, Mitral calcification
CASE REPORT
A 62-year old woman was admitted to hospital for heart failure. Transoesophageal echocardiogram revealed aortic valve stenosis (Ao valve area, 0.9 cm2; PG, 45 mmHg; MG, 25 mmHg) and a diseased calcified mitral valve with stenosis and regurgitation (mitral valve area, 1.1 cm2; MG, 10 mmHg; RV, 25 ml; ERO, 12 mm2). The preoperative coronary angiogram showed double-vessel disease. The calculated EuroSCORE II was 4.08. Her medical history included chronic lymphocytic leukaemia in 1999 with recurrence in 2004, 2005 and 2007, requiring multiple courses of chemotherapy. She also had renal cancer that was treated with right nephrectomy in 2006, followed by end-stage renal insufficiency and definitive dialysis.
We proposed surgical aortic valve replacement, mitral valve replacement and double coronary bypass grafting. The procedure started with cardiopulmonary bypass (CPB) insertion and cardioplegia. Then, we decalcified the aortic valve first, even though the aortic and mitral calcifications were fused. Opening the left atrium and exposing the mitral valve revealed heavy mitral annulus calcifications, which were very deep into the left atrium and the left ventricle muscle, around the full annulus circumference. We decided to avoid complete deep mitral annulus decalcification (Fig. 1A). Using the transapical Ascendra system (Edwards Lifesciences, Inc., Irvine, CA, USA), we inserted a 26-mm Edwards SAPIEN XT valve (Edwards Lifesciences, Inc.) through the left atriotomy under visual control (Fig. 1B), without using guide wire or fluoroscopy.
Figure 1:
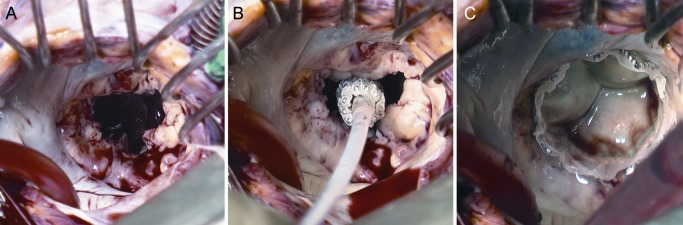
(A) Intraoperative view of the heavily calcified mitral annulus. (B) Positioning of the Edwards SAPIEN valve under visual inspection without any guiding wire or fluoroscopy. (C) Deployment of the Edwards SAPIEN valve with careful positioning into the calcified mitral annulus.
The balloon was inflated into the calcified annulus. After deflation, we tested the anchoring of the endovalve into the mitral annulus. The valve diameter perfectly fit the mitral annulus diameter, and it was impossible to pull back the stented valve with our forceps (Fig. 1C). However, the water test revealed paravalvular leakage around the stented valve. The annulus was not perfectly circular and was heavily calcified, inducing some degree of non-apposition of the endovalve around the annulus. To prevent paravalvular leakage, we closed the gap between the endovalve and the calcified annulus using a ring of bovine pericardium, with one side sutured on the stent and the other side on the atrial tissue over the annulus calcification (Fig. 2A). We used a running suture of Prolene 4.0 to close the gap. The water test then showed no leakage (Fig. 2B).
Figure 2:

(A) The custom-made bovine pericardium ring used to close the gap between the endovalve and the calcified mitral annulus to avoid paravalvular leakage. (B) Final outcome of using the sutured pericardial patch to close the paravalvular leakage area around the endovalve, resulting in a perfect water test. (C) Postoperative echocardiography shows the perfect positioning of the mitral Edwards valve without any paravalvular leakage. The chest X-ray shows both the aortic and mitral bioprosthetic valves.
The atrium was closed using a running suture of Prolene 3.0. PERIMOUNT Magna (21 mm; Edwards Lifesciences, Inc.) was implanted in the aortic position. A double venous bypass was performed on the right and first marginal coronary arteries. The CPB weaning was performed easily. Postoperative echocardiography showed a good position of the endovalve in the mitral annulus, with a 2.0-cm2 valve area and a 3-mmHg mean gradient without paravalvular leakage (Fig. 2C).
DISCUSSION
Mitral valve surgery in the presence of extensive annular calcification remains a surgical challenge. In 1987, Cammack et al. [1] referred to mitral annulus calcification as ‘the bar of death’; at that time, the mortality after such surgery was 30%. To approach the difficult problem of mitral valve surgery after decalcification, several techniques have been described, with a number of severe complications, including left ventricular rupture, haemorrhagic complications, atrioseptal defect and atrioventricular fistula. Improved management of these complications during this complex surgery has led to decreased mortality. Recently, Feindel et al. [2] reported an operative mortality of 9.3%. The five deaths in that study included two due to severe coagulopathy, one to low cardiac output, one to sepsis and multiorgan failure and one to myocardial infarction complicated by posterior interventricular septum rupture related to occlusion of a diseased right coronary artery.
El Asmar et al. [3] described a technique of mitral valve repair to avoid the risks associated with mitral valve replacement in a severely calcified mitral annulus. They performed mitral valve repair by en bloc resection of the annular calcium deposits, and annular reconstruction was performed using pledgeted-supported sutures, with good results. However, this technique is limited by the requirements for a repairable valve and non-extensive calcification, as radical decalcification leaves tissue that is of poor quality for holding sutures and atrioventricular fistula.
Small case series have recently described the successful off-label use of transcatheter aortic valve implantation (TAVI) in patients with degenerated bioprosthetic valves in the mitral position. This technique was first demonstrated in seven sheep models by Kempfert et al. [4]; they implanted a 26-mm Physio ring, then positioned an Edwards SAPIEN valve within the annuloplasty ring under fluoroscopic guidance. In 2010, Webb et al. [5] published a study involving valve-in-valve implantations in seven mitral bioprostheses. They reported successful Edwards SAPIEN valve implantation, with immediate restoration of satisfactory valve function in all patients. No patient had more than mild regurgitation after implantation, and no patient died during the procedure. Thirty-day mortality was 4.2%. Each of the above-described studies used a valve-in-valve technique, with the endovalve seated in an artificial rigid structure (Physio ring or bioprosthesis). In the present case report, we describe a totally new concept, in which the endovalve was placed into a native calcified mitral annulus. We further used a ring pericardial patch to prevent paravalvular leakage between the endovalve and the native annulus. To our knowledge, this is also the first report of Edwards SAPIEN valve implantation using the Ascendra system through a left atrium access.
The described technique was a bailout procedure to reduce the operative mortality associated with complete mitral annulus decalcification during a long procedure requiring bi-valve replacement and double bypass grafting. In such a case, the use of a balloon-expandable valve under visual control must be considered, as this technique decreases the operative time and the potential injuries of full mitral decalcification. The present case shows the feasibility of using TAVI during open surgery, with easy valve positioning and deployment without any guiding system or fluoroscopy. The visual inspection and slow inflation of the balloon provide accurate endovalve positioning in the native calcified mitral annulus.
In conclusion, we report that the use of a sutureless valve, such as an Edwards SAPIEN valve, is a promising method for mitral valve replacement in complex cases involving bar calcification of the mitral annulus.
Conflict of interest: none declared.
REFERENCES
- 1.Cammack PL, Edie RN, Edmunds LH. Bar calcification of the mitral annulus. A risk factor in mitral valve operations. J Thorac Cardiovasc Surg. 1987;94:399–404. [PubMed] [Google Scholar]
- 2.Feindel CM, Tufail Z, David TE, Ivanov J, Armstrong S. Mitral valve surgery in patients with extensive calcification of the mitral annulus. J Thorac Cardiovasc Surg. 2003;126:777–82. doi: 10.1016/s0022-5223(03)00081-3. doi:10.1016/S0022-5223(03)00081-3. [DOI] [PubMed] [Google Scholar]
- 3.El Asmar B, Acker M, Couetil JP, Perier P, dervanian P, Chauvaud S, et al. Mitral valve repair in the extensively calcified mitral valve annulus. Ann Thorac Surg. 1999;52:66–9. doi: 10.1016/0003-4975(91)91420-z. doi:10.1016/0003-4975(91)91420-Z. [DOI] [PubMed] [Google Scholar]
- 4.Kempfert J, Blumenstein JM, Borger MA, Linke A, Lehmann S, Pritzwald-Stegmann P, et al. Minimally invasive off-pump valve-in-a-valve implantation: the atrial transcatheter approach for re-operative mitral valve replacement. Eur Heart J. 2009;29:2382–7. doi: 10.1093/eurheartj/ehn285. doi:10.1093/eurheartj/ehn285. [DOI] [PubMed] [Google Scholar]
- 5.Webb JG, Wood DA, Ye J, Gurvitch R, Masson JB, Rodés-Cabau J, et al. Transcatheter valve-in-valve implantation for failed bioprosthetic heart valves. Circulation. 2010;121:1848–57. doi: 10.1161/CIRCULATIONAHA.109.924613. doi:10.1161/CIRCULATIONAHA.109.924613. [DOI] [PubMed] [Google Scholar]