

Abstract
The Bezold-Jarisch reflex, a well-described phenomenon, occurs upon the stimulation of intracardiac mechanoreceptors and is mediated by vagal afferent nerve fibers. Several factors can sensitize the cardiovascular system to develop this reflex, including acute myocardial ischemia, natriuretic peptides, and, rarely, nitroglycerin administration in the setting of acute myocardial infarction. The development of the Bezold-Jarisch reflex in the presence of severe coronary artery stenosis, specifically left main coronary artery stenosis, has not been described. We report 2 cases of patients who underwent elective coronary angiography and were given intra-arterial nitroglycerin during radial sheath insertion to reduce radial artery spasm. In both patients, bradycardia and hypotension developed along with diaphoresis, consistent with the Bezold-Jarisch reflex. Coronary angiography revealed critical (>90%) left main coronary artery stenosis in both patients. Critical left main coronary artery stenosis might sensitize mechanoreceptors or vagal afferents to the development of the Bezold-Jarisch reflex after intra-arterial nitroglycerin use; however, the mechanism of this possible relationship is unclear. In addition to discussing our patients' cases, we review the medical literature relevant to the Bezold-Jarisch reflex.
Key words: Blood pressure/physiology, bradycardia/chemically induced, heart rate/drug effects, hypotension/chemically induced, nitroglycerin/adverse effects, reflex/drug effects/physiology
Intra-arterial nitroglycerin is often used during transradial cardiac catheterization procedures to prevent radial artery spasm during sheath insertion. The Bezold-Jarisch reflex (BJR) is known to be elicited by nitroglycerin, particularly in the setting of acute myocardial infarction; however, this occurs rather rarely.1 We report the cases of 2 patients undergoing elective angiographic procedures in whom there developed a likely BJR after nitroglycerin was administered during radial sheath insertion. Neither patient had signs or symptoms of acute myocardial ischemia immediately before cardiac catheterization; however, both were found to have critical left main coronary artery (LMCA) stenosis. We propose that critical LMCA stenosis might lead to the development of the BJR in some patients after intra-arterial nitroglycerin use. In addition to reporting the cases of our patients, we review the relevant medical literature.
Case Reports
Patient 1
A 61-year-old man presented with recurrent anginal symptoms. His medical history included coronary artery disease and the placement of a drug-eluting stent in the mid-left anterior descending coronary artery (LAD) after a myocardial infarction 3 years earlier. During initial coronary angiography, no intraluminal stenoses had been noted in the other coronary arteries. At the current presentation, he underwent exercise stress testing for further evaluation (exercise duration, 9 min 40 s on standard Bruce protocol). The test results revealed an acceptable heart rate and a left ventricular ejection fraction of 0.50. However, the electrocardiographic (ECG) component revealed diagnostic 3-mm ST-segment depression in the inferolateral leads, and the echocardiographic component disclosed septal and apical wall-motion abnormalities during peak stress.
The patient was referred for coronary angiography. A right radial approach was used. A 6F introducer sheath was inserted in the radial artery. In routine fashion, 200 μg of nitroglycerin was administered intra-arterially through the sheath, to prevent radial artery spasm. The patient's blood pressure before nitroglycerin administration was 149/92 mmHg, and his heart rate was 56 beats/min. However, within 1 minute, a hypotensive and bradycardic response developed in association with diaphoresis: the patient's heart rate slowed to 28 beats/min and his systolic blood pressure decreased to 87 and then to 58 mmHg. The patient was asked to cough and was given 1 mg of intravenous atropine and normal saline solution, which yielded improvement in his heart rate and blood pressure over the next few minutes. After hemodynamic recovery, the angiographic procedure was resumed. The patient had no angina or ECG signs of ischemia. Coronary angiography revealed a >90% ostial LMCA stenosis (Fig. 1); the other coronary arteries had no luminal stenoses. The previously placed stent in the mid-LAD was patent. The patient was referred for coronary artery bypass grafting (CABG).
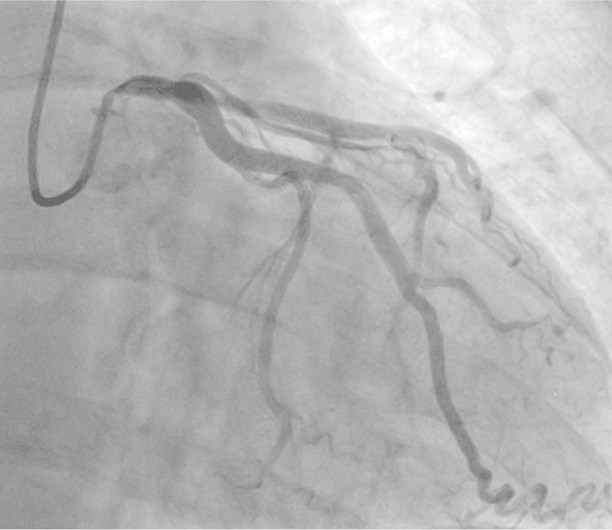
Fig. 1 Patient 1. Coronary angiogram (anteroposterior view) shows a >90% ostial left main coronary artery stenosis.
Patient 2
A 70-year-old man with a history of hypertension and type 2 diabetes mellitus presented with Canadian Cardiovascular Society (CCS) class III anginal symptoms and was referred for coronary angiography. A left radial approach was used. A 6F introducer sheath was inserted in the radial artery. In routine fashion, 200 μg of nitroglycerin was administered intra-arterially through the sheath, to prevent radial artery spasm. The patient's blood pressure before nitroglycerin administration was 153/73 mmHg, and his heart rate was 76 beats/min. However, within 1 minute, a hypotensive and bradycardic response developed in association with diaphoresis: the patient's heart rate slowed to 18 beats/min and his systolic blood pressure decreased to 55 and then to 34 mmHg. The patient was asked to cough, and he was given 1 mg of intravenous atropine followed by 0.5 mg of intravenous atropine and normal saline solution. This yielded improvement in the patient's heart rate and blood pressure over the next few minutes, after which the angiographic procedure was resumed. The patient had no angina or ECG signs of ischemia. Coronary angiography revealed a 99% distal LMCA stenosis (Fig. 2); the other coronary arteries had no luminal stenoses. The patient was referred for CABG.

Fig. 2 Patient 2. Coronary angiogram (anteroposterior view) shows a 99% distal left main coronary artery stenosis.
Discussion
In these 2 patients with critical LMCA stenosis, bradycardia and hypotension developed in response to intra-arterial nitroglycerin during radial sheath insertion. Both patients were symptomatic in terms of diaphoresis. The mechanism of each reaction was consistent with a BJR. Nitroglycerin has been shown to induce the BJR in the presence of acute myocardial infarction1; however, no association has previously been described between nitroglycerin-induced BJR and critical LMCA disease in the absence of acute infarction. The BJR includes a triad of bradycardia, hypotension and vasodilation and is often also accompanied by hypopnea, nausea, and diaphoresis.2 This vagally mediated reflex was initially recognized in 1867 by von Bezold and Hirt3; decades later, it was characterized chiefly by Jarisch.4,5 The BJR is thought to result from the stimulation of cardiopulmonary mechanoreceptors that are associated with unmyelinated vagal afferent nerve fibers, classified as C-fibers.6 These fibers terminate in the nucleus tractus solitarii in the brain stem.7 Stimulation of the C-fibers is thought to occur through mechanical or chemical means and was initially performed experimentally with the use of veratrum alkaloids. Serotonin and serotonin agonists have also evoked the BJR. Nitroglycerin has only rarely been implicated in eliciting a BJR. The mechanism is thought to be related to a decrease in ventricular filling, which leads to a vigorous contraction of myocardial muscle fibers and the subsequent activation of ventricular mechanoreceptors that are innervated by C-fibers; this in turn evokes the BJR. Given the rarity of this occurrence with nitroglycerin use, other factors might be involved in sensitizing certain patients to nitroglycerin-induced BJR. Myocardial ischemia and infarction have been implicated several times as a sensitizing factor to the BJR,7,8 and ischemia of the inferoposterior left ventricular wall has also elicited the BJR. Although the mechanism of this process is unclear, prostaglandins and oxygen-derived free radicals might act as mediators.9 The relationship is thought to have a teleologic basis. Pro-brain, atrial, and C-type natriuretic peptides have all sensitized sheep and rats to the effects of phenylbiguanide (a serotonin agonist) and increased the BJR's activation of cardiac vagal motoneurons.10–12 Rarely, radiographic contrast agents can induce the BJR, especially when injected into the right coronary artery.
Coronary stenosis alone—without concurrent ischemia—has not been reported as a sensitizing factor for development of the BJR. In terms of critical LMCA stenosis, we found no published cases that described this relationship. The afferent neural fiber bundle is anatomically near the LMCA,13 so perhaps a critical stenosis in this region sensitizes mechanoreceptors to the acute hemodynamic effects of nitroglycerin; however, the significance of this anatomic relationship as a predisposing factor for causing the BJR is uncertain. In our 2 patients, the BJR clearly developed immediately after the administration of intra-arterial nitroglycerin, before the introduction of any guidewire or catheter into the radial artery or manipulation of the coronary ostia with a catheter. It is unknown whether the same response would have been elicited with a different vasodilator (such as a calcium channel blocker, used in some laboratories) or via a different route of administration (intravenous or sublingual). It is also unclear to what extent intravenous sedation—usually given to patients before and during cardiac catheterization procedures—might amplify the effect of intra-arterial nitroglycerin. A general vagal response is clinically indistinguishable from the BJR; however, the rarity of vagal responses in our ample transradial experience, as well as the particular occurrences in these 2 nearly identical cases with critical LMCA stenosis and the timing after nitroglycerin administration, support the possibility of a BJR over a simple vagal response.
The clinician's prompt identification of the BJR, and administration of therapy with intravenous atropine and fluids along with occasionally elevating the patient's legs to increase venous return and thus preload, can be crucial in reversing hypotension and bradycardia and preventing a patient's downward spiral toward myocardial ischemia.
Given the frequent use of the radial approach for coronary angiography and the concurrent routine use of inter-arterial vasodilators such as nitroglycerin, clinicians should be aware of the potential for a BJR in patients with critical LMCA disease.
Footnotes
Address for reprints: Sergio Waxman, MD, Lahey Clinic, 41 Mall Rd., Burlington, MA 01805
E-mail: sergio.waxman@lahey.org
References
- 1.Come PC, Pitt B. Nitroglycerin-induced severe hypotension and bradycardia in patients with acute myocardial infarction. Circulation 1976;54(4):624–8. [DOI] [PubMed]
- 2.Campagna JA, Carter C. Clinical relevance of the Bezold-Jarisch reflex. Anesthesiology 2003;98(5):1250–60. [DOI] [PubMed]
- 3.Bezold A, Hirt L. Uber die physiologischen wirkungen des essigsauren veratrine [in German]. Unters Physiol Lab Wurzburg 1867;1:73–122.
- 4.Jarisch A, Henze C. Uber blutdrucksenkung durch chemische erregung depressorischer nerven [in German]. Naunyn-Schmiedeberg's Arch Exp Pathol Pharmak 1937;187:706–30.
- 5.Jarisch A. Vom herzen ausgehende kreislaufreflexe [in German]. Arch Kreislaufforsch 1940;7:360–74.
- 6.Kashihara K, Kawada T, Yanagiya Y, Uemura K, Inagaki M, Takaki H, et al. Bezold-Jarisch reflex attenuates dynamic gain of baroreflex neural arc. Am J Physiol Heart Circ Physiol 2003;285(2):H833–40. [DOI] [PubMed]
- 7.Robertson D, Hollister AS, Forman MB, Robertson RM. Reflexes unique to myocardial ischemia and infarction. J Am Coll Cardiol 1985;5(6 Suppl):99B–104B. [DOI] [PubMed]
- 8.Thames MD, Klopfenstein HS, Abboud FM, Mark AL, Walker JL. Preferential distribution of inhibitory cardiac receptors with vagal afferents to the inferoposterior wall of the left ventricle activated during coronary occlusion in the dog. Circ Res 1978;43(4):512–9. [DOI] [PubMed]
- 9.Ustinova EE, Schultz HD. Activation of cardiac vagal afferents in ischemia and reperfusion. Prostaglandins versus oxygen-derived free radicals. Circ Res 1994;74(5):904–11. [DOI] [PubMed]
- 10.Thomas CJ, May CN, Sharma AD, Woods RL. ANP, BNP, and CNP enhance bradycardic responses to cardiopulmonary chemoreceptor activation in conscious sheep. Am J Physiol Regul Integr Comp Physiol 2001;280(1):R282–8. [DOI] [PubMed]
- 11.Toader E, McAllen RM, Cividjian A, Woods RL, Quintin L. Effect of systemic B-type natriuretic peptide on cardiac vagal motoneuron activity. Am J Physiol Heart Circ Physiol 2007; 293(6):H3465–70. [DOI] [PubMed]
- 12.Deliva RD, Ackermann U. Atrial natriuretic peptide and mechanisms of cardiovascular control. Role of serotonergic receptors. Am J Physiol 1998;274(3 Pt 2):R711–7. [DOI] [PubMed]
- 13.Frink RJ, James TN. Intracardiac route of the Bezold-Jarisch reflex. Am J Physiol 1971;221(5):1464–9. [DOI] [PubMed]