

Abstract
The fundamental assertion of worldview-based models of posttraumatic stress disorder is that trauma symptoms result when traumatic experiences cannot be readily assimilated into previously held worldviews. In two studies, we test the anxiety buffer disruption hypothesis, which states that trauma symptoms result from the disruption of normal death anxiety-buffering functions of worldview. In Study 1, participants with trauma symptoms greater than the cutoff for PTSD evinced greater death-thought accessibility than those with sub-clinical or negligible symptoms after a reminder of death. In Study 2, participants with clinically significant trauma symptoms showed no evidence of worldview defense though death-thoughts were accessible. These results support the anxiety buffer disruption hypothesis, and suggest an entirely new approach to experimental PTSD research.
Keywords: trauma, PTSD, terror management, anxiety buffer, death, shattered assumptions
Cognitive models have offered a useful conceptualization of posttraumatic stress disorder (PTSD) in terms of face validity, research generation, and treatment success (see Ozer & Weiss, 2004, for a review). One class of cognitive models proposes a worldview comprised of underlying assumptions about the self and the world that are undermined, or shattered, by the experience of trauma (e.g., Janoff-Bulman, 1992).
In “shattered assumptions” theory, Janoff-Bulman (1992) articulates the role of the worldview in psychological efforts to retain and enhance perceptions of control and stability after traumatic events. According to “shattered assumptions” theory (Janoff-Bulman, 1992), individuals develop fundamental, yet unarticulated, assumptions about the world and themselves (i.e., worldviews) that allow for healthy human functioning. The most important assumptions include beliefs in a just, benevolent, predictable world in which the individual possesses competence and worth. The worldview’s primary function is to provide the individual with meaning, self-esteem, and the illusion of invulnerability.
According to shattered assumptions theory, when individuals experience an event that damages their worldview (i.e., traumatic material that cannot be easily integrated with previously held worldviews), they no longer perceive the world as benevolent and predictable or themselves as competent and invulnerable. The subsequent state of defenseless, terrifying, and confusing awareness of personal vulnerability gives rise to the anxiety and physiological reactivity that characterize PTSD. Importantly, it is not only that worldviews are undermined, but that individuals become intensely aware of their own mortality when those beliefs are stripped away (Janoff-Bulman, 1992). While worldview-based models are intuitively compelling to many researchers and clinicians, they must be judged on the validity of their central premise: trauma symptoms are caused by shattering of worldviews.
Evidence for worldview-based models of PTSD
Support for the notion that worldview shattering is responsible for trauma symptoms is equivocal. Research aimed at assessing the shattered assumptions hypothesis has relied almost exclusively on the World Assumptions Scale (WAS; Janoff-Bulman, 1989), which has been shown to have psychometric problems (e.g., Elklit, Shevlin, Solomon, & Dekel, 2007; Kaler et al., 2008) and, more importantly, assumes that people have “on line” access to the content of their own worldviews. That is, while the theory states that worldview content is largely unconscious, the WAS requires participants to rate their global perceptions about abstract notions such as the degree to which the world is just.
A second major limitation of extant research is the use of retrospective reporting on pre-trauma worldviews. While some studies suggest that PTSD is related to worldview change (e.g., Drescher & Foy, 1995), self-reported retrospective worldview change is no substitute for prospective research. Indeed, the only prospective study to test whether the experience of a traumatic event produced change on the WAS found that experiencing a potentially traumatic event did not change individuals’ worldviews (Kaler et al., 2008).
Rather than asking participants to report on their worldview content, or retrospectively report whether that content has changed, a better approach is to directly test for the protective functioning of worldviews. A reliable way to directly measure the functioning of worldviews has been pioneered by Terror Management Theory (TMT; Solomon, Greenberg, & Pyszczynski, 1991), and the theoretical groundwork and some empirical support for its extension to PTSD have been offered by Anxiety Buffer Disruption Theory (ABDT; Abdollahi, Pyszczynski, et al., in press). TMT states that functioning worldviews keep the awareness of morality out of consciousness, so worldview functioning can be measured by assessing the degree to which death-related thoughts are cognitively accessible (i.e., death-thought accessibility; DTA).
Terror Management Theory and Worldviews
Like the “shattered assumptions” perspective, terror management theory (TMT) suggests that worldviews provide people with a sense of meaning, structure, purpose, and invulnerability (Solomon et al., 1991). TMT argues that humans have the unique ability to be self-aware in a spatiotemporal context, and to mentally project the self through space and time (Wheeler, Stuss, & Tulving, 1997) in order to envision and plan for future threats. An unfortunate consequence of these useful cognitive adaptations is that humans also possess an awareness of their own impending death, a future threat that cannot be avoided. This awareness has the potential to incite psychological “terror” if individuals are forced to face thoughts about their own inescapable mortality (see Solomon, Greenberg, Pyszczynski, & Koole, 2004, for a review).
Terror is managed collectively by worldviews, which provide either literal (e.g., religious worldviews; afterlife) or symbolic (e.g., secular worldviews; lasting achievements) routes to immortality. Properly functioning worldviews are vital because they allow individuals to keep death thoughts out of consciousness. A large body of research has demonstrated that when individuals are reminded of their personal morality (i.e., mortality salience; MS), they rely on worldviews as a psychological defense. MS has been manipulated using a variety of techniques [e.g., showing videos portraying scenes of death (Greenberg, Solomon, Pyszczynski, Rosenblatt, Burling, Lyon, et al., 1992) or asking participants to “jot down, as specifically as you can what you think will happen to you as you physically die” (Rosenblatt, Greenberg, Solomon, & Pyszczynski, 1989). In response to these reminders of mortality, participants have repeatedly been shown to engage in worldview defense strategies. That is, when thoughts of death are made conscious, participants report greater preference for others who share their beliefs and hostility to those who do not, display attempts to enhance their own self-esteem, vigorously protect sacred cultural icons and symbols, and reaffirm closely held cultural beliefs (see Pyszczynski, Greenberg, Solomon, Arndt, & Schimel, 2004, for a review).
While worldview defense has been consistently observed as a response to MS, high self-esteem can preempt defensive responses. Self-esteem serves as a buffer against the terror of mortality because it is a signal that the individual is living up to the standards for immortality afforded by the cultural worldview (Pyszczynski et al., 2004). In research on its terror management functions, self-esteem has been manipulated via false feedback on personality, IQ, and other tests (Solomon et al., 2004)
Research on the workings of the terror management system has delineated the process and time course of a given instance of “terror” (i.e., MS). Proximal defenses are seen immediately following death reminders and consist of complete suppression of death thoughts. That is, immediately following an overt MS manipulation, an individual’s degree of death-thought accessibility is significantly lower than that of an individual not reminded of death. Distal defenses are seen as proximal defenses wane, the overt reminder of mortality moves to the edges of consciousness, and death thought accessibility becomes high (e.g., after a delay and distraction task). Distal defenses consist of meaning and self-esteem bolstering efforts, such as worldview defense and outgroup derogation, which occur when DTA is high (see Arndt et al., 2004, for a review). However, research has shown that when self-esteem is temporarily bolstered prior to MS, defensive responses are attenuated and death-thought accessibility remains low (Harmon-Jones, Simon, Greenberg, & Pyszczynski, 1997). A compromised worldview fails to provide proximal defense. That is, after an overt reminder of their own mortality, individuals with a compromised worldview experience increased DTA immediately (DTA; Hayes, Schimel, Faucher, & Williams, 2008; Schimel, Hayes, Williams, & Jahrig, 2007).
Perception of meaning in life and self-esteem as self-report indicators of worldview functioning
In contrast to specific worldview content that is partly unconscious, a sense of life’s meaningfulness and self-esteem are indicators of a functioning worldview that are readily available to consciousness and, thus, can be self-reported. They are not components of the worldview itself; rather, they indicate that the worldview is present and functioning properly. Trauma survivors often report that trauma impacts their sense of self, as well as perceptions of meaning and purpose, just as they report greater awareness of their own mortality and vulnerability (Falsetti, Resick, & Davis, 2003).
Anxiety Buffer Disruption Theory
Anxiety Buffer Disruption Theory (ABDT; Pyszczynski & Kesebir, in press; Abdollahi et al., in press) broadens TMT by explicitly bridging it to worldview-based models of PTSD. This extension of TMT is heavily influenced by shattered assumptions theory, as both highlight the existential problem at the root of PTSD symptoms. ABDT posits that trauma symptoms are precisely the psychological consequences that TMT has long proposed worldviews act to ameliorate. The physiological arousal symptoms of PTSD occur because the normal anxiety-buffering functions of worldviews are disrupted by the traumatic event, leaving the individual unprotected against the terror of mortality. Further, the “cognitive cycling” between intrusive thoughts about the trauma and avoidance of traumatic material signals attempts to integrate the traumatic event into the worldview in order to restore its anxiety-buffering capability. The distinction between ABDT and shattered assumptions theory is one of emphasis. Where shattered assumptions emphasizes the often unarticulated (and, perhaps, unobservable) cognitive discrepancies between worldview and traumatic material, ABDT focuses on the (observable) disruption of worldview functioning.
ABDT adds to worldview-based models of PTSD the hypothesis that peri-traumatic dissociation (i.e. dissociation during the traumatic event) is a signal that the normal anxiety-buffering functions of worldview have been overwhelmed, and points to evidence that peri-traumatic dissociation is a potent predictor of later PTSD symptoms (Ozer et al., 2003) as support for that assertion. In their initial test of ABDT, Abdollahi and colleagues (in press; Study 1) found that survivors of the deadly 2005 Zarand, Iran earthquake who reported a high tendency to dissociate did not engage in worldview defense (i.e., the normal protective functions of worldview were disrupted) in response to reminders of mortality or the earthquake. Two years later, in a second study with the same participants, those with high levels of trauma symptoms showed no evidence of worldview defense after MS or reminders of the earthquake, while those with low symptoms responded with worldview defense. Most compelling, however, were the findings that dissociation at Time 1 predicted trauma symptoms at Time 2, and further, the relationship was partially mediated by decreased worldview defense at both Time 1 and Time 2 (Abdollahi et al., in press; Study 2). These findings yield the first evidence that the disruption of the anxiety-buffering functions of worldviews play a role in the development and maintenance of trauma symptoms, and that peri-traumatic dissociation may signal anxiety buffer disruption.
Present studies
The work by Abdollahi and colleagues (in press) represents a critical first step in demonstrating that PTSD symptoms may be a result of compromised worldviews that no longer buffer individuals from existential terror. However, this seminal work omits direct examination of the two fundamental hypotheses of the terror management system: (1) compromised worldviews fail to buffer individuals from death thought accessibility in the face of mortality salience, and (2) compromised worldviews fail to provide individuals with self-esteem. If, as ABDT suggests, PTSD represents a disruption of worldview functioning, then individuals experiencing PTSD symptoms should not demonstrate an initial suppression of DTA in the face of mortality salience and should demonstrate lower perceptions of meaning and lower self-esteem. Further, if worldview functioning is compromised in these individuals, boosts to self-esteem—a strategy previously used to bolster worldview functioning before MS (e.g., Greenberg, Pyszczynski, Solomon, Pinel, Simon, & Jordan, 1993)—should not be an effective “antidote” (i.e., should not initiate death thought suppression). Thus, low DTA after a reminder of mortality is evidence of proper worldview functioning, even if a self-esteem boost is required to achieve it.
In Study 1, we asked individuals with three levels of trauma symptom severity (i.e., low: negligible symptoms, medium: significant but sub-clinical symptoms, and high: symptoms greater than the suggested cutoff for PTSD) to report their level of self-esteem and the degree to which they perceived meaning in their lives. Then, we assessed worldview functioning in those three groups by measuring DTA after overtly reminding participants of their own mortality (mortality salience; MS), their most stressful/traumatic event (trauma salience; TS), or a control topic (dental pain). In accordance with the standard TMT experimental paradigm, we measured DTA either immediately following the salience prime (no delay) or after a delay and distraction so that we could observe DTA in both the proximal and distal stages of the terror management process. We expected that the lowest self-esteem, least perceived life meaning, and greatest degree of DTA would be observed in the high trauma symptom group, followed by the medium and low symptom groups. Further, we expected a 3-way interaction of trauma symptom group, salience prime, and stage of terror management process, such that participants in the high and medium trauma symptom groups would evince the greatest degree of DTA in the proximal stage (i.e., no delay) following MS and TS primes. Finally, we expected only the low trauma symptom group to engage in worldview defense, and only in the distal stage (i.e., after a delay and distraction).
Study 1
Method
Participants
Four hundred forty-seven students (206 women and 241 men, mean age= 19) at the University of XX [for blind review] participated in the study for partial research credit in an introductory psychology course.
Procedure
Participants reserved appointment times for the study entitled “Personality, experiences, and opinions” through an online participant pool system. Upon arrival to the laboratory, each participant read and signed informed consent forms, was randomly assigned to 1 of 6 experimental conditions, then escorted to a small room that contained only a chair, a desk, and a Dell desktop PC. All measures were completed on MediaLab v.6 software. Participants were then debriefed and given contact information for mental health professionals.
Materials
The measures listed below were presented to participants in the order listed.
Salience manipulation
Based on assigned condition, participants first completed 1 of 3 versions of The Projective Life Attitude Assessment (Rosenblatt, Greenberg, Solomon, Pyszczynski, & Lyon, 1989), in which 2 open-ended questions are presented under the guise of a new, innovative measure of personality. The open-ended instructions for the mortality salience condition (MS) are as follows: “Please briefly describe the emotions that the thought of your own death arouses in you”, and “Jot down, as specifically as you can, what you think will happen to you as you physically die and once you are physically dead.” Parallel questions were presented in the trauma salience (TS) and dental pain (control) conditions, except that “what happened during your most stressful or traumatic experience” or “dental pain” was substituted for death.
Delay and distract/No delay
Based on assigned condition, immediately following the experimental manipulation, participants were either presented with two puzzles (one word search, one word-stem completion task) which served as a delay and distraction task between the salience induction and the measure of death-thought accessibility (DTA), or were immediately presented with the DTA measure. This type of delay and distraction has been widely used in TMT research, and has been shown to be necessary to demonstrate increased DTA after reminders of mortality due to the proximal defenses described above (see Arndt, Cook, & Routledge, 2004, for a review).
Death-thought accessibility (DTA)
Following Greenberg, Arndt, Simon, Pyszczynski, & Solomon (2000), DTA was assessed by the number of death-related words participants generated in a word completion task which included 13 word fragments which could be completed with a neutral or death-related word (e.g., COFF_ _ could be completed as COFFEE or COFFIN ). Word stems completed with a death-related word were summed for a total DTA score.
Worldview defense
Participants were asked to rate their agreement with a number of current political positions that imply group membership (i.e., immigration, separation of church/state, abortion, intelligent design) as a measure of worldview defense (e.g., “The children of illegal immigrants should automatically be granted U.S. citizenship.” Response options ranged from 1 (strongly disagree) to 7 (strongly agree), and were summed for a total worldview defense score (α= .79).
Self-esteem
The Rosenberg Self-Esteem Scale (1965) assessed trait self-esteem. It consists of 10 statements (e.g., “On the whole, I am satisfied with myself “) related to overall feelings of self-worth or self-acceptance. Response options ranged from 1 (strongly disagree) to 4 (strongly agree), and were summed for a total self-esteem score (α= .75).
Meaning
Perceptions of life’s meaningfulness were assessed with the Perceived Personal Meaning Scale (PPMS; Wong, 1998) on which participants rate five items (α= .94) regarding their life meaning (e.g., “My life as a whole has meaning”) on a scale ranging from 1 (strongly disagree) to 10 (strongly agree). The Perceived Personal Meaning Scale has shown good concurrent and predictive validity (Wong, 1998).
Trauma history
The Traumatic Life Events Questionnaire (TLEQ; Kubany et al., 2000) assessed whether participants had ever experienced each of 18 types of potentially traumatic experiences (e.g., natural disasters, vehicle accidents, sexual violence). For each event type, participants were asked to provide the number of times it had occurred (i.e., PTSD Criterion A1), from 0 (never) to 5 (5 or more), and whether they experienced fear, helplessness, or horror (yes/no; i.e., PTSD Criterion A2 per DSM-IV-TR). After providing responses for each event type, participants were asked to select which event was most distressing in the present.
Trauma symptoms
The PTSD Checklist-Civilian (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993), a 17-item self-report measure adapted from the 17 PTSD symptoms listed in the DSM-IV, assessed the presence and severity of trauma symptoms related to participants’ most distressing event from the TLEQ. Participants were asked to rate on a scale of 1 (not at all) to 5 (extremely) the degree to which they were bothered in the past month by each of 17 symptoms (e.g., “Repeated, disturbing memories, thoughts or images of the event?”). Scores on the 17 items were then summed for a total severity score. The PCL-C has demonstrated strong psychometric properties, including good internal consistency and test-retest reliability, as well as good diagnostic efficiency (.90 and .94) using a cutoff score for PTSD “caseness” of 44 (Blanchard et al., 1996; Ventureya et al., 2002; see Norris & Hamblen, 2004, for a review). In the present study, scores ranged from 17–71, and Cronbach’s alpha was .93. Participants were divided into 3 trauma symptom groups based on their PCL-C scores [i.e., low= 17–22 (N=220, M= 18.87, SD=1.87), medium: 23–43 (N= 178, M= 29.65, SD=5.20), high: 44–71 (N= 49, M=52.12, SD=7.00)]. Thus, the high trauma symptom group was populated only with participants who scored above the suggested cutoff for PTSD.
Results
Trauma prevalence and symptom severity
The majority (64%) of participants reported having experienced one of the potentially traumatic events listed (excluding on-time loss of a loved one). A sizeable minority (25%) reported having experienced at least 5 instances of potentially traumatic events. Trauma symptoms varied widely (range= 17–71), with a sample mean of 26.81.
Trauma symptom severity and worldview indicators
To assess whether greater trauma symptom severity was related to lower meaning and self-esteem, the two primary self-report indicators of worldview functioning, two one-way analyses of variance (ANOVAs) were conducted. Perceived life meaningfulness and self-esteem, were positively correlated (r= .30, p< .01), so the alpha level for significance was corrected to .025 for each. Trauma symptom groups differed as hypothesized on both perceived meaningfulness of life, F(2, 444)= 5.97, p< .01, and self-esteem, F(2, 444)= 14.79, p< .01 (Table 1).
Table 1.
Mean Life Meaning and Self-Esteem Scores by Trauma Symptom Group
| Life Meaning
|
Self- Esteem
|
||
|---|---|---|---|
| Trauma Symptom Group | High n= 49 |
24.47a (7.23) | 39.78c (3.59) |
| Medium n= 178 |
26.63b (5.33) | 41.75d (3.17) | |
| Low n= 220 |
27.42b (5.09) | 42.58e (3.37) |
Note: Values that share a superscript are equivalent.
Death-thought accessibility
To test the hypothesis that participants with significant trauma symptoms would evince the greatest degree of DTA, particularly in the proximal stage (i.e., no delay) following MS and TS primes, we conducted a 3 (trauma-symptom status: high vs. medium vs. low) × 3 [salience prime: mortality salience (MS) vs. trauma salience (TS) vs. control] × 2 (delay: yes vs. no) between-subjects analysis of variance (ANOVA).1,2 All cell means are given in Table 2.
Table 2.
Mean Number of Death Words Completed as a Function of Trauma Symptom Status, Salience Prime, and Delay Condition in Study 1
| Delay
|
No Delay
|
|||||||
|---|---|---|---|---|---|---|---|---|
| Salience Prime | Salience Prime | |||||||
| Control |
|
Trauma | Control |
|
Trauma | |||
| Mortality | Mortality | |||||||
| n= 95 | n= 84 | n= 79 | n= 63 | n= 62 | n= 64 | |||
|
|
|
|||||||
| Trauma Symptom Group | High | 1.54 (1.51) | 3.38 (2.07) | 1.80 (2.20) | High | 1.67 (1.41) | 5.20 (3.70) | 2.40 (2.07) |
| n= 30 | n= 11 | n= 9 | n= 10 | n= 19 | n= 9 | n= 5 | n= 5 | |
| Medium | 1.75 (1.23) | 2.40 (2.37) | 1.80 (1.70) | Medium | 1.80 (1.38) | 4.26 (2.30) | 2.14 (1.66) | |
| n= 105 | n= 36 | n= 30 | n= 39 | n= 73 | n= 25 | n= 19 | n= 29 | |
| Low | 1.50 (1.25) | 2.95 (2.05) | 2.10 (1.56) | Low | 1.90 (1.50) | 2.47 (1.89) | 2.03 (1.67) | |
| n= 123 | n= 48 | n= 45 | n= 30 | n= 97 | n= 29 | n= 38 | n= 30 | |
Contrary to our expectations, results revealed no main effect for trauma symptom status, F(2, 427)=5.23, p= .19, partial η2=.01. However, significant main effects of salience prime, F(2, 427)=23.93, p< .01, partial η2=.10, and delay condition, F(1, 427)= 5.74, p< .05, were noted. Specifically, post hoc tests with Bonferroni correction showed that DTA was significantly higher in the mortality salience (MS) condition (M= 3.07 words) than in the trauma salience (TS) condition (M= 2.04 words), p < .01. The TS condition did not significantly differ from the control condition (M= 1.69 words). Also, the main effect of delay showed that DTA was slightly higher in the no delay condition (M= 2.47 words) than in the delay and distract condition (M= 2.11 words), d= .16, a finding that runs counter to previous TMT research in which MS increases DTA only after a delay and distraction.
These main effects were qualified by the expected significant 3-way trauma-symptom status X salience condition X delay interaction, F(4, 427)= 2.68, p< .05, partial η2=.03, (Figure 1), in which the lack of immediate death-thought suppression for participants with high and medium trauma symptoms after MS was noted. To probe the 3-way interaction, simple effects tests (i.e., significance tests that include the total ANOVA MSerror and df) were conducted to compare DTA across salience primes within each delay condition/trauma group combination.
Figure 1.
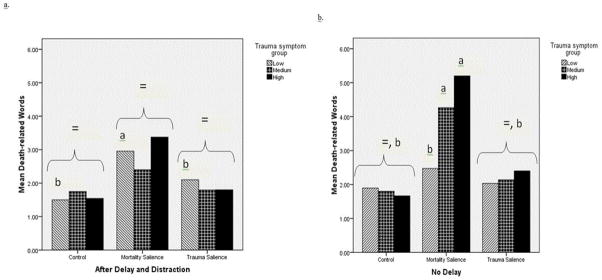
Figure 1a-b. Mean number of death words completed in the delay and distraction (a) and no delay (b) conditions. Figure components that share a superscript do not significantly differ from one another. Those with different subscripts differ significantly from one another. Bracketed components with an equality sign do not differ significantly from one another.
Focusing first on results that reflect the traditional TMT paradigm, in which DTA is elevated in the distal stage after MS, only participants with low trauma symptoms evince the traditional pattern. In the delay and distract condition, MS increased DTA only for the low trauma symptom group, F(2, 442)= 7.21, p< .01, adj. R2=.03. However, in the proximal stage, we found support for the hypothesis that death thought suppression is less successful in the high and medium trauma symptom groups after MS, but not after TS as we had expected. In the no delay condition, the effect of salience condition on DTA was significant for the high, F(2, 442)= 4.95, p< .01, adj. R2=.02, and medium, F(2, 442)= 9.73, p< .01, adj. R2=.04, trauma symptom groups only (low trauma symptom group, F(2, 442)< 1, n.s.). Follow-up simple contrasts showed that in the high trauma symptom group, participants in the MS condition reported significantly greater DTA than in the dental pain condition, t (442)= 2.39, p< .02, but DTA reported by participants in the TS and dental pain conditions did not differ, t (442)= .28, n.s. Similarly, in the medium trauma symptom group, participants in the MS condition reported significant greater DTA than in the dental pain condition, t (442)= 3.58, p< .01, but DTA reported by participants in the TS and dental pain conditions did not differ, t (442)= .80, n.s.
Worldview defense
Contrary to expectations, there were no effects of group, salience manipulation, or delay on the worldview defense measure. While we expected no worldview defense from those with high and medium trauma symptoms, previous research suggested that those with low trauma symptoms would engage in worldview defense in the distal stage.
Discussion
Study 1 tested whether individuals who report clinically significant trauma symptoms would exhibit evidence of anxiety buffer disruption. The results showed that both self-report indicators of worldview functioning (i.e., perceived meaning and self-esteem) were compromised in individuals with significant trauma symptoms, and that the degree of trauma symptoms that participants reported was inversely proportional to their perception of meaning and possession of self-esteem.
The results of Study 1 also showed evidence of impaired anxiety buffer functioning. Indeed, we found that immediately following reminders of mortality, participants with both moderate and high levels of trauma symptoms exhibited increased DTA while individuals with negligible trauma symptoms showed no such elevation in DTA. Moreover, the high trauma symptom group showed greater than twice the degree of DTA of the low trauma symptom group after MS in the proximal stage. Also, there was some indication of a dose-response effect, in that the high (i.e., clinical) symptom group showed a trend toward greater DTA than the medium (i.e., sub-clinical) group. After a delay and distraction following reminders of mortality (as in typical TMT studies), however, only the low trauma symptom group showed increased DTA after MS, and elevated DTA scores after MS did not differ as a function of trauma symptom group. This provides some preliminary evidence that the anxiety buffer (i.e., worldview) that facilitates immediate death-thought suppression does not operate as successfully after mortality reminders in individuals with significant trauma symptoms as it does for those without significant trauma symptoms. We also expected to find differences in worldview defense in the distal stage, as participants with low trauma symptoms were expected to exhibit worldview defense after a delay and distraction. However, we found no evidence that trauma symptom group, salience manipulation, or delay condition affected worldview defense.
We expected to find that reminding participants with significant trauma symptoms of their most traumatic event would result in those participants exhibiting increased DTA, but it did not. This runs counter to Abdollahi and colleagues’ (in press) results for reminders of the Iranian earthquake, in which earthquake reminders operated like MS primes. Because of the variety of ways that individuals responded to the trauma salience prompt (i.e., different trauma types, different narrative means of construing the event), it is difficult to know whether reminders of traumatic events in general truly do not operate as MS primes or if our prompt failed to elicit true reminders (e.g., perhaps some participants opted against writing about their feelings and detailed accounts of their most traumatic experience in favor of something less threatening).3
An important limitation of Study 1 was the lack of consideration of depression as a source of trauma symptom group differences. Not only do symptoms of depression and PTSD exhibit a substantial degree of overlap, and the disorders themselves are very often comorbid (Kessler, Sonnega, Bromet, & Hughes, 1995; O’Donnell, Creamer, & Pattison, 2004), but also increased thoughts about death are a diagnostic feature of depression (APA, 2004). These considerations are particularly important given that the fairly scant previous TMT research to directly assess psychological disorders has shown that participants with mild depression respond differently than non-depressed participants to reminders of mortality (i.e., they exhibit more vigorous worldview defense than non-depressed participants; Simon et al., 1996; 1998).
Another important limitation of Study 1 was the lack of a reliable measure of worldview defense. We believe that our non-significant worldview defense findings are due to the fact that, although some of the participants in Study 1 (particularly those without significant trauma symptoms in the MS/delay condition) likely engaged in worldview defense, we were unable to appropriately assess whether worldview defense occurred because we did not measure participants’ cultural/political identities with respect to the highly contentious issues we provided as opportunities for worldview defense. To illustrate this problem, previous research has shown that participants who identify as liberal in their political ideology respond differently to MS than do those who identify as conservatives (Greenberg, Simon, Solomon, Pyszczynski, & Chatel, 1992). In the present study, liberal and/or secular participants may have defended their liberal worldview by increased endorsement of abortion rights, liberal immigration policies, greater separation of church and state, and restrictions on teaching of intelligent design, while conservative and/or traditionally religious participants may have defended their worldview just as vigorously with opposite responses.
Finally, while we are confident that the increased DTA we observed in the high and medium trauma groups during the proximal period after MS represented evidence of a disruption in the anxiety-buffering capability of participants’ worldviews, likely due to the type of “shattering” suggested by Janoff-Bulman (1992) and others, we are also aware that lowered self-esteem may be a consequence of trauma (Darvez-Bornoz, Lepine, Choquet, Berger, Degiovanni, & Gaillard, 1998). Since self-esteem plays such an integral role in terror management processes, it is possible that the increased DTA we observed was not due to worldview disruption per se, but merely a byproduct of temporarily lowered self-esteem that co-occurs with trauma symptoms.
Study 2
The first aim of Study 2 was to replicate the finding from Study 1 that individuals with elevated trauma symptoms show weakened immediate death-thought suppression after MS in proportion to the severity of their trauma symptoms, and to extend the finding by controlling for symptoms of depression.
The second aim of Study 2 was to test whether, similar to individuals without trauma symptoms in previous studies, individuals with high trauma symptoms would show evidence of worldview defense when death-thoughts are highly accessible. If participants with substantial trauma symptoms were to show no evidence of worldview defense when death-thoughts are highly accessible, it would suggest that, indeed, the anxiety-buffering capability of their worldviews had been undermined. Study 2 addressed an important limitation of Study 1 by assessing worldview defense by measuring participants’ responses to anti-American sentiment using an established vignette technique. Many TMT studies have focused on American identity as an important and universally-defended (among Americans) domain of worldview (Pyszczynski, Greenberg, & Solomon, 1999). Unlike in Study 1, if we were to observe a lack of worldview defense on this type of worldview defense measure, the absence of worldview defense could be interpreted as further evidence of anxiety buffer disruption.
The third aim of Study 2 was to test whether temporarily increased self-esteem prior to MS would decrease DTA in participants with medium or high trauma symptoms immediately after MS, as it has been shown to in college students after a delay and distraction (e.g., Harmon-Jones et al, 1997). Previous research has also shown that temporary boosts to self-esteem help buffer anxiety after MS (Greenberg, Pyszczynski, Solomon, Pinel, Simon, & Jordan, 1993) and attenuate defensive responses to MS, including derogation of anti-American targets (Arndt & Greenberg, 1999) and DTA (Harmon-Jones et al., 1997). If diminished self-esteem (rather than underlying anxiety buffer disruption) were the reason that participants were unable to immediately suppress death-related thoughts in Study 1, then a manipulation that temporarily increased self-esteem prior to MS would decrease DTA immediately after MS in individuals with medium or high trauma symptoms. It should be noted that, were the self-esteem boost manipulation to succeed in attenuating DTA for participants with medium and high trauma symptoms, we would not expect to observe worldview defense in any group. If we were to observe no effect of temporarily bolstered self-esteem and no worldview defense in participants with significant trauma symptoms when DTA is high, we would interpret such a finding as evidence of anxiety-buffer disruption.
Method
Participants
Two hundred and ninety students (185 women and 105 men, mean age= 19) from the University of XXX participated in the study for partial credit for an introductory psychology course.
Procedure
Study 2 was conducted in the same space, using the same computer hardware and software, and the same recruitment and participant-experimenter interaction protocols as Study 1. However, Study 2 differed from Study 1 in that it introduced a self-esteem boost vs. self-esteem neutral manipulation, used only MS and control as salience manipulations, and DTA was measured only in the proximal stage (i.e., with no delay after MS or control). The procedure for Study 2 began with a MediaLab introduction in which participants were informed that they would be completing the Temperament and Character Inventory (Cloninger, Przybeck, Svrakic, & Wetzel, 1994), a personality test that has been shown to be a good predictor of “future life success.” Next, participants responded to 30 personality-related items such as, “I prefer variety to routine,” on a 7-point Likert scale anchored with “Strongly Disagree” and “Strongly Agree.” After completing the items, the computer screen briefly read, “Please wait while we calculate your score for the Temperament and Character Inventory.” The profiles that followed served as the self-esteem manipulation. Those profiles were the same as those used in prior studies of the influence of self-esteem boosts on terror management effects (e.g., Greenberg, Solomon et al., 1992). Based on assigned condition, participants received 1 of 2 versions of bogus feedback (self-esteem boost vs. neutral), ostensibly from scores on the Temperament and Character Inventory (Cloninger, 1994), in the form of a paragraph describing the individual’s personality, prospects for the future, and psychosocial adjustment relative to others. In the self-esteem boost condition, participants read statements such as, “While you may feel you have personality weaknesses, your personality is very strong,” and “You are generally self-sufficient.” While in the neutral condition, participants read, “You have a few personality weaknesses; however, you are able to compensate for most of them,” and “You are generally self-sufficient although you sometimes need others to like or admire you.”
Materials
After the self-esteem manipulation, the measures listed below were presented to participants in the order listed.
Salience manipulation
Participants completed 1 of 2 versions (MS or dental pain) of The Projective Life Attitude Assessment (Rosenblatt et al., 1989) described in Study 1.
Death-thought accessibility (DTA)
Immediately following the MS manipulation, DTA was assessed by the same word completion task as described in Study 1.
Worldview defense
Two vignettes adapted from the Multidimensional Social Transgression Scale (Florian & Mikulincer, 1997) were used to assess reactions to social transgressions motivated by anti-American sentiment. The first described a group of college students protesting U.S. foreign policy and burning an American flag. The second described an immigrant farm worker who destroyed a day’s worth of crops because of outrage at the lack of opportunity or sensitivity in America. Participants read each vignette and rated the severity of the offense and the degree of punishment the transgressor should receive on a scale from 1 (not at all severe/very light punishment) to 7 (very severe/very heavy punishment). The 4 ratings (2 severity, 2 punishment) were averaged together for a mean cultural transgression rating (α= .76).
Self-esteem
The Rosenberg Self-Esteem Scale (1965) was again used to assess self-esteem (α = .84).
Trauma symptoms
As in Study 1, PTSD Checklist-Civilian (PCL-C; Weathers, Litz, Herman, Huska, & Keane, 1993) was used to assess the presence and severity of trauma symptoms (α= .90). In Study 2, scores ranged from 17–73 (sample mean= 32.15). Participants were divided into low, medium, and high trauma symptom groups based on their PCL-C scores [i.e., low= 17–22 (n=54, mean= 19.83, SD=1.68), medium: 23–43 (n= 195, mean= 31.31, SD=5.80), high: 44–71 (n= 49, mean=52.39, SD=10.92)]; a PCL-C score of 44 or greater maximizes diagnostic prediction for PTSD (Blanchard et al., 1996).
Depression
The Center for Epidemiologic Studies-Depression Scale (CES-D; Radloff, 1977) is a psychometrically sound 20-item scale assessing frequency of depressive symptoms over the past week (Radloff, 1977) on a scale of 0 (rarely or none of the time) to 3 (most or all of the time). Responses were summed for a total depression score (α= .89).
Manipulation check
At the end of the study, participants were asked to write their recollections of the personality feedback they received. Experimenters coded the responses by counting the number of distinct phrases, then coding the valence of each as positive or negative. Agreement was acceptable for both positive statements (K= .78) and negative statements (K=.71). Separate sum scores were created for positive and negative phrases.
Results
Manipulation check
Compared to participants who received neutral personality feedback, participants who received the positive personality feedback remembered significantly more positive statements (mean positive statements= 2 vs. 1.6; t (276)= 2.61, p< .01, d= .31) and significantly fewer negative statements (mean negative statements= .83 vs. 1.3; t (276)= 4.25, p< .01, d= .51) at the conclusion of the study.
Impact of Self-esteem on DTA
To assess whether temporarily boosted self-esteem decreased DTA in individuals with medium or high trauma symptoms, we conducted a 3 (trauma-symptom status: high vs. medium vs. low) X 2 (salience prime: mortality salience (MS) vs. control) X 2 (self-esteem: self-esteem boost vs. neutral) analysis of covariance (ANCOVA) in which we entered the CES-D as a covariate to control for the influence of depression on DTA.3 All cell means are given in Table 3. Results suggested an effect of salience prime, F(1, 277)= 22.31, p< .01, partial η2=.08, such that participants completed more word stems with death-related words after MS (M= 2.62) than after the control (dental pain) prime (M = 1.58), and a 2-way salience prime X self-esteem manipulation interaction, F(1, 277)= 4.03, p< .05, partial η2=.01, in which participants completed more word stems with death-related words after the MS prime in the self-esteem boost condition than in the neutral self-esteem condition (mean self-esteem boost= 2.92, vs. mean neutral self-esteem= 2.30). There was no main effect of trauma symptom status, but there was a trend toward a 3-way salience prime X self-esteem manipulation X trauma symptom status interaction, F(2, 277)= 2.30, p= .10, partial η2=.02 (Figure 2).
Table 3.
Mean Number of Death Words Completed as a Function of Trauma Symptom Status, Self-Esteem Manipulation, and Salience Prime in Study 2
| Self-Esteem Boost
|
Neutral Self-Esteem
|
|||||
|---|---|---|---|---|---|---|
| Salience Prime
|
Salience Prime
|
|||||
| Control | Mortality | Control | Mortality | |||
| n= 75 | n= 73 | n= 76 | n= 66 | |||
|
|
|
|||||
| Trauma Symptom Group | High | 1.92 (1.44) | 3.57 (2.88) | High | 1.30 (1.33) | 2.83 (1.64) |
| n= 19 | n= 12 | n= 7 | n= 22 | n= 10 | n= 12 | |
| Medium | 1.63 (.93) | 2.80 (1.79) | Medium | 1.50 (1.53) | 2.33 (1.84) | |
| n= 102 | n= 46 | n= 56 | n= 93 | n= 54 | n= 39 | |
| Low | 1.12 (1.32) | 3.10 (1.37) | Low | 2.25 (1.91) | 1.80 (1.82) | |
| n= 27 | n= 17 | n= 10 | n= 27 | n= 12 | n= 15 | |
Figure 2.
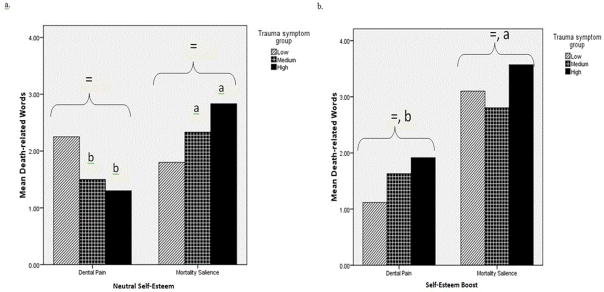
Figure 2a-b. Mean number of death words completed in the neutral self-esteem (a) and self-esteem boost (b) conditions. Figure components that share a superscript do not significantly differ from one another. Those with different subscripts differ significantly from one another. Bracketed components with an equality sign do not differ significantly from one another.
To probe the 3-way interaction trend, and in order to assess whether a pattern of DTA similar to that found in Study 1 in response to MS emerged in Study 2, we conducted a simple effects test (i.e., significance tests that include the total ANOVA MSerror and df) to assess a potential salience prime by trauma symptom group interaction within each self-esteem condition.
In the neutral self-esteem condition, as in Study 1, the salience prime X trauma symptom group interaction was significant, F(2, 287)= 3.98, p< .05, adj. R2=.02. Follow-up simple contrasts showed that the effect of MS on DTA was greater in the high trauma symptom group than in the low symptom group, t (287)= 1.89, p< .06, and that the effect of MS did not differ between the low and medium trauma symptom groups, t (287)= 4.53, p< .05. However, further simple effects tests revealed that DTA was greater after MS only in the high trauma symptom group, F(1, 287)= 4.53, p< .05, adj. R2=.01, and the medium trauma symptom group, F(1, 287)= 6.50, p= .01, adj. R2=.02, not in the low trauma symptom group, F(1, 287)< 1, n.s.
In the self-esteem boost condition, the salience prime X trauma symptom group interaction trend was significant, F(2, 287)= 3.67, p< .05, adj. R2=.02. Follow-up simple contrasts showed that MS increased DTA more in the low trauma symptom group than in the medium symptom group, t (287)= 2.59, p= .01, and that the effect of MS did not differ between the low and high trauma symptom groups, t (287)= 1.37, n.s. Further simple effects tests revealed that DTA was greater after MS in the high trauma symptom group, F(1, 287)= 2.84, p< .10, adj. R2=.01, the medium trauma symptom group, F(1, 287)= 13.33, p< .01, adj. R2=.04, and the low trauma symptom group, F(1, 287)= 9.38, p< .01, adj. R2=.03. Within the MS condition, the test of trauma symptom group on DTA scores reached significance, F(1, 287)= 3.07, p= .05, but simple contrasts showed no significant pairwise group differences. Between trauma symptom groups, significance tests may have been limited by the small number of participants in some cells (particularly the high symptom group).
Finally, within each trauma symptom group in both the dental pain and MS conditions, DTA levels were compared across self-esteem conditions using simple effects tests. The only effect of self-esteem condition was that DTA in response to MS was higher in the self-esteem boost condition in the low trauma symptom group, F(1, 287)= 4.10, p< .05, adj. R2=.01. This finding was unexpected, in that we expected no effect of self-esteem boost on DTA in the low trauma symptom group.
Worldview defense
In the neutral self-esteem condition, we conducted a 3 (trauma symptom status) X 2 (salience prime) ANOVA. We found no evidence of worldview defense in any group. Neither main effect, nor their interaction, was significant. Also, WVD scores did not differ by salience prime in any trauma group.
Discussion
Results of the neutral self-esteem condition of Study 2 replicated those of Study 1, in that DTA increased immediately following MS for both the medium and high trauma symptom groups, but not the low trauma symptom group, controlling for depression. Consistent with ABDT predictions, participants with substantial trauma symptoms, though they showed increased DTA in the MS condition, did not show increased reliance on an important worldview domain, American identity, to defend against death-related thoughts. This stands in contrast to numerous previous TMT studies that have shown that participants with functioning worldviews rely more heavily on those worldviews when DTA is high (i.e., the mortality salience hypothesis; Greenberg, Pyszczynski, Solomon, & Rosenblatt, 1990; see Solomon, Greenberg, Pyszczynski, & Koole, 2004, for a review). This finding corresponds to the Study 1 finding that participants with significant trauma symptoms report lower perceptions of life’s meaningfulness. Thus, participants with significant trauma symptoms appear to possess worldviews that fail to provide a sense of meaning that can be relied on to defend against thoughts about death.
We found no evidence that our self-esteem boost manipulation attenuated the immediate DTA increase experienced by medium and high trauma symptom groups following MS. To the contrary, the self-esteem manipulation increased DTA slightly after MS across trauma symptom groups. The finding that the self-esteem boost did not confer DTA protection is not surprising, given the lack of worldview defense observed in Study 2. According to TMT, self-esteem, insomuch as it operates as a “death anxiety buffer,” works because it is an indicator that the individual (a) possesses a functioning worldview that provides a sense of meaning, and (b) is meeting the standards of value set out by that worldview. Thus, the fact that our self-esteem boost failed to decrease DTA in individuals with significant trauma symptoms after reminders of mortality can be interpreted as support for the notion that the anxiety buffering functions of those participants’ worldviews are compromised.
General Discussion
Both ABDT and shattered assumptions theory (Janoff-Bulman, 1992) hold that the primary function of worldviews is to provide perceptions of meaning, order, controllability, and personal invulnerability in order to keep individuals from becoming fully aware of their own vulnerability and mortality (Janoff-Bulman & Yopyk, 2004). However, we argue that the anxiety buffer disruption hypothesis may have advantages compared to the shattered assumptions hypothesis because it allows researchers to directly observe worldview functioning as opposed to relying on participants’ self-report of theoretically unconscious worldview content. The theoretical differences are largely a function of emphasis, since the disruption of worldview’s anxiety buffering capabilities may well be due to worldview “shattering.” However, until a valid way of assessing worldview content, traumatic appraisals, and discrepancies between the two simultaneously is offered (Park, 2010), we believe that ABDT is the way forward for probing worldview-based theories of PTSD.
In Study 1, we found support for the hypothesis that participants with high trauma symptoms possess worldviews that are incapable of buffering anxiety. Those with high symptoms reported low levels of the two indicators of worldview functioning that are available to consciousness (i.e., perception of life’s meaningfulness and self-esteem). Study 1 also provided some preliminary support for the anxiety buffer disruption hypothesis using a directly observable indicator of worldview functioning, DTA. Individuals with significant trauma symptoms displayed a lack of proximal defense against incursions of death-related thoughts, suggesting a weakened worldview. Further, the effect followed a dose-response pattern by trauma symptom severity. A great deal of research using TMT has shown that the primary psychological function of worldviews is to keep thoughts of death at bay (Solomon et al., 2004), and these findings connect worldview-based models of PTSD to this broader literature, in that they are the first to provide experimental evidence that the core function of worldviews (i.e., suppression of death-thoughts) is compromised in individuals with significant trauma symptoms.
TMT research also provides a roadmap for probing the precise sources of anxiety buffer disruption. Previous studies have shown that functioning worldviews keep death thoughts unconscious by (a) providing meaning structures that can be reaffirmed after reminders of death (i.e., worldview defense) and (b) providing self-esteem as an indicator of progress toward immortality. Thus, in Study 2, we sought to test whether participants with significant trauma symptoms would rely on a commonly used worldview defense strategy, and if a temporary boost to self-esteem would allow them to keep thoughts of death at bay.
Results of Study 2 replicated those of Study 1, in that both participants with trauma symptoms above the suggested cutoff for PTSD “caseness” and those with subclinical trauma symptoms showed evidence of anxiety buffer disruption, in that they showed increased DTA immediately following MS. Unlike previous TMT studies, however, they showed no evidence of worldview defense when death-thoughts were accessible. This finding agrees with previous research on ABDT, which showed that participants lack of worldview defense after MS was predictive of both concurrent and subsequent (i.e., 2 years later) PTSD symptoms (Abdollahi et al., in press). Not only did participants with significant trauma symptoms not engage in worldview defense, but they also did not respond to the temporary boost in self-esteem with decreased DTA. Previous TMT research has shown that individuals with functioning worldviews show no increase in DTA after MS when they are first provided with self-esteem boosting information (Harmon-Jones et al., 1997).
These findings provide preliminary evidence for an assertion common to both shattered assumptions theory and ABDT: that the core problem of trauma in relation to PTSD symptoms lies in the fact that the experience of trauma leaves some individuals defenseless against the terrifying realization of vulnerability in the face of mortality. A preponderance of research into terror management processes have shown that in the course of daily living, individuals must manage the potential terror that can accompany subtle reminders of mortality (e.g., Landau, Johns, Greenberg, Pyszczynski, Martens, Goldenberg, & Solomon, 2004). The present research suggests that individuals with significant trauma symptoms may be stripped of this fundamental cognitive ability that is theorized to have evolved through the course of human history to deal with these threats. While previous research has shown that trauma survivors often describe this new awareness of mortality and vulnerability (Falsetti et al., 2003), this is the first research to observe that awareness experimentally. Further, this research is among the first to bridge theoretical positions on the link between mortality awareness and trauma symptoms and connect worldview-based models of PTSD to the larger literature on the core functions of worldviews.
Limitations
Two findings, in particular, give us pause. First, the theoretical foundations of TMT suggest that the terror associated with the human awareness of death is constantly in the background of consciousness, and that worldviews are always operating to keep terror at bay. In the present studies, however, we found no difference between trauma symptom groups on DTA in the control condition (i.e., dental pain). It seems as though participants with worldviews whose anxiety buffering functions are disrupted should exhibit a higher baseline degree of DTA even when thinking about an aversive topic such as dental pain, given that short-term, targeted, and non-traumatic challenges to worldview yield increased DTA in the absence of MS (Hayes et al., 2008; Schimel, Hayes, Williams, & Jahrig, 2007).
A more problematic result is that we found no difference between trauma symptom groups on DTA after reminders of their most stressful or traumatic experience, nor any differences between reminders of traumatic experiences and dental pain. If the experience of a traumatic event damages an individual’s worldview because it creates a discrepancy between the pre-existing worldview and the new information implied by the event (Park & Folkman, 1997), then reminding participants of that event should have increased DTA in the same way as overt reminders of mortality did. Further, in Abdollahi and colleagues’ (in press) study, participants responded to reminders of the Iranian earthquake in a manner similar to the traditional MS prime. This difference between the two studies’ findings may be due to the fact that Abdollahi et al.’s participants all responded to a reminder of the same, shared traumatic experience while the participants in this study were reminded of events that were specific to each individual and represented varying degrees of traumatic exposure. Future research should take up the question of which traumatic events serve as MS conditions, or under what circumstances they do so. Another plausible explanation is that participants in the trauma salience condition did not write about their true “most traumatic experience,” since we presented the traumatic event checklist after the salience manipulation. Had we used the checklist as the trauma salience condition, we may have found an effect of trauma salience.
Implications for worldview-based models of PTSD
The first and most important theoretical contribution of the present work for worldview-based models of PTSD is its provision of support for a premise first introduced in shattered assumptions theory (Janoff-Bulman, 1992): that existential concerns such as awareness of mortality are the source of anxiety in PTSD and the drivers of worldview reconstruction efforts such as intrusions and avoidance. The present study shows only that a core function of worldviews is undermined in individuals with significant trauma symptoms. However, by demonstrating that loss of functioning, the present work bridges worldview-based models of PTSD to the broader TMT literature. Further, by demonstrating the link between worldview functioning and trauma symptoms, this research opens the door for PTSD theory development that incorporates worldview functioning alongside (or in place of) trauma-related changes in worldview content.
Treatment implications
ABDT suggests that treatment designs should understand and take into account the two primary components of a functioning cultural worldview (i.e., belief in a meaningful and ordered world, self-esteem derived from meeting cultural standards of worth) in order to assess domains of each that are affected by traumatic experiences and to understand the connections between damage to the cultural worldview and subsequent distress. Fortunately, there is evidence to suggest that some researchers and practitioners have recognized the need to address existential issues in the context of PTSD treatment (Schnyder, 2005) and the practice of psychotherapy more generally (e.g., Keshen, 2006) and have begun to develop treatment approaches with that goal in mind (e.g., Hayes, Luoma, Bond, Masuda, & Lillis, 2006).
Conclusions
ABDT represents a theoretical synthesis of worldview-based models of PTSD and TMT that enriches both. The most important benefit for both theory development and future practical application is that long-held assumptions about the role of worldview functioning and the processes by which worldviews “shatter” and are reconstituted can now be empirically assessed via observable phenomena, such as DTA and worldview defense, that do not rely on retrospective reports of theoretically unconscious material.
Acknowledgments
This work was supported by a seed grant from Division 36 of the American Psychological Association. The first author’s contribution to this publication was made possible by Grant Number UL1 RR024156 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH), and NIH Roadmap for Medical Research. Its contents are solely the responsibility of the authors and do not necessarily represent the official view of NCRR or NIH. Information on NCRR is available at <http://www.ncrr.nih.gov/.> Information on Re-engineering the Clinical Research Enterprise can be obtained from <http://nihroadmap.nih.gov/clinicalresearch/overview-translational.asp.>
Biographies
Donald Edmondson, Ph.D., is an Associate Research Scientist at the Center for Behavioral Cardiovascular Health, Columbia University Medical Center. His research focuses on trauma, worldviews, and their influences on health.
Stephenie R. Chaudoir, PhD is an Assistant Professor of Psychology at Bradley University, where her program of research focuses on examining the psychological, behavioral, and health consequences of possessing a concealable stigmatized identity.
Mary Alice Mills, Ph.D., is a clinical research fellow at the Boston Consortium of Clinical Psychology, VA Boston Healthcare System, and the National Center for PTSD, and a teaching fellow in the Division of Psychiatry at Boston University School of Medicine. Working primarily with Veterans, her research focuses on risk and resilience factors for PTSD.
Crystal L. Park, Ph.D., is Professor of Clinical Psychology at the University of Connecticut, Storrs. She studies multiple aspects of coping, including the making of meaning in the context of traumatic events and life-threatening illnesses.
Julie Holub B.A. is the Research Coordinator for the Cocaine Research Clinic at Yale University School of Medicine. She works primarily with neuroimaging techniques in the study of substance abuse and dependence.
Jennifer M. Bartkowiak, B.A., is a graduate student in the Clinical Psychology program at the University of Hartford. Her previous research is in the area of Alzheimer’s Disease and Mild Cognitive Impairment.
Footnotes
To partially address concerns about participants disengaging from the trauma salience prompt, three independent raters coded each participant response to each prompt across salience prompts in the no delay condition on a scale of 1 (not at all engaged/did not follow instructions) to 3 (completely engaged/followed instructions). The three raters showed high agreement (ICC= .78), and the ratings were summed for a total engagement score. Only essays in the dental pain condition (control) differed from the MS and TS conditions (mean= 2.0 vs. 2.3 and 2.4, respectively), F(2, 179)= 9.42, p< .01. After controlling for task engagement/following directions, the pattern of results for death thought accessibility was unchanged. Thus, engagement was dropped from all further analyses.
To account for traumatic event type, participants’ responses to the TLEQ were dummy coded to reflect whether each participant had ever experienced an interpersonal trauma (i.e., 0 if no endorsement of a potentially traumatic interpersonal event; 1 if the participant endorsed any of the following: assault, child physical abuse, child sexual abuse, adult sexual abuse, threat of death, domestic violence). Interpersonal traumatic event endorsement was not a significant covariate in the model, so it was deleted from the model and all further analyses.
The inclusion of the CES-D did not significantly influence the results of either of the 3 (trauma symptom status) X 2 (salience prime) X 2 (self-esteem boost/neutral) ANCOVA models (predicting DTA or WVD). In neither was it a significant covariate in the model, nor did it influence the model R2 or the pattern of estimated means.
References
- Abdollahi A, Pyszczynski T, Maxfield M, Lusyszczynska A. Posttraumatic stress reactions as a disruption in anxiety-buffer functioning: Dissociation and responses to mortality salience as predictors of severity of post-traumatic symptoms. Psychological Trauma: Theory, Research, Practice, and Policy (in press) [Google Scholar]
- APA. Diagnostic and Statistical Manual of Mental Disorders. 4. Washington, D.C: APA; 2000. DSM-IV-TR. [Google Scholar]
- Arndt J, Cook A, Routledge C. The blueprint of terror management: Understanding the cognitive architecture of psychological defense against the awareness of death. In: Greenberg J, Koole S, Pyszczynski T, editors. Handbook of experimental existential psychology. New York: Guilford Press; 2004. pp. 35–53. [Google Scholar]
- Arndt J, Greenberg J. The effects of a self-esteem boost and mortality salience on responses to boost relevant and irrelevant worldview threats. Personality and Social Psychology Bulletin. 1999;25:1331–1341. [Google Scholar]
- Arndt J, Greenberg J, Solomon S, Pyszczynski T. Suppression, accessibility of death-related thoughts, and cultural worldview defense: Exploring the psychodynamics of terror management. Journal of Personality and Social Psychology. 1997;73:5–18. doi: 10.1037//0022-3514.73.1.5. [DOI] [PubMed] [Google Scholar]
- Becker E. The denial of death. New York: Free Press; 1973. [Google Scholar]
- Blanchard EB, Jones-Alexander J, Buckley TC, Forneris CA. Psychometric properties of the PTSD checklist (PCL) Behaviour Research and Therapy. 1996;34:669–673. doi: 10.1016/0005-7967(96)00033-2. [DOI] [PubMed] [Google Scholar]
- Cloninger C, Przybeck T, Svrakic D, Wetzel R. TCI—The temperament and character inventory: A guide to its development and use. St Louis (MO): Center for Psychobiology of Personality, Washington University; 1994. [Google Scholar]
- Drescher KD, Foy DW. Spirituality and trauma treatment: Suggestions for including spirituality as a coping resource. National Center for PTSD Clinical Quarterly. 1995;5:4–5. [Google Scholar]
- Elklit A, Shevlin M, Solomon Z, Dekel R. Factor structure and concurrent validity of the World Assumptions Scale. Journal of Traumatic Stress. 2007;20:291–301. doi: 10.1002/jts.20203. [DOI] [PubMed] [Google Scholar]
- Falsetti SA, Resick PA, Davis JL. Changes in religious beliefs following trauma. Journal of Traumatic Stress. 2003;16:391–398. doi: 10.1023/A:1024422220163. [DOI] [PubMed] [Google Scholar]
- Florian V, Mikulincer M. Fear of death and the judgment of social transgressions: A multidimensional test of terror management theory. Journal of Personality and Social Psychology. 1997;73:369–380. doi: 10.1037//0022-3514.73.2.369. [DOI] [PubMed] [Google Scholar]
- Greenberg J, Arndt J, Schimel J, Pyszczynski T, Solomon S. Clarifying the function of mortality salience-induced worldview defense: Renewed suppression or reduced accessibility of death-related thoughts? Journal of Experimental Social Psychology. 2001;37(1):70–76. [Google Scholar]
- Greenberg J, Arndt J, Simon L, Pyszczynski T, Solomon S. Proximal and distal defenses in response to reminders of one’s mortality: Evidence of a temporal sequence. Personality and Social Psychology Bulletin. 2000;26:91–99. [Google Scholar]
- Greenberg J, Pyszczynski T, Solomon S, Rosenblatt A. Evidence for terror management theory II: The effects of mortality salience on reactions to those who threaten or bolster the cultural worldview. Journal of Personality and Social Psychology. 1990;58:308–318. doi: 10.1037//0022-3514.57.4.681. [DOI] [PubMed] [Google Scholar]
- Greenberg J, Pyszczynski T, Solomon S, Pinel E, Simon L, Jordan K. Effects of self-esteem on vulnerability-denying defensive distortions: Further evidence of an anxiety-buffering function of self-esteem. Journal of Experimental Social Psychology. 1993;29:229–251. [Google Scholar]
- Greenberg J, Simon L, Solomon S, Pyszczynski T, Chatel D. Terror management and tolerance: Does mortality salience always intensify negative reactions to others who threaten one’s worldview? Journal of Personality and Social Psychology. 1992;63:212–220. doi: 10.1037//0022-3514.63.2.212. [DOI] [PubMed] [Google Scholar]
- Greenberg J, Solomon S, Pyszczynski T, Rosenblatt A, Burling J, Lyon D, Simon L. Assessing the terror management analysis of self-esteem: Converging evidence of an anxiety-buffering function. Journal of Personality and Social Psychology. 1992;63:913–920. doi: 10.1037//0022-3514.63.6.913. [DOI] [PubMed] [Google Scholar]
- Harmon-Jones E, Simon L, Greenberg J, Pyszczynski T. Terror management theory and self-esteem: Evidence that increased self-esteem reduced mortality salience effects. Journal of Personality and Social Psychology. 1997;72:24–36. doi: 10.1037//0022-3514.72.1.24. [DOI] [PubMed] [Google Scholar]
- Hayes J, Schimel J, Faucher EH, Williams TJ. Evidence for the DTA hypothesis II: Threatening self-esteem increases death-thought accessibility. Journal of Experimental Social Psychology. 2008;44(3):600–613. [Google Scholar]
- Janoff-Bulman R. Assumptive worlds and the stress of traumatic events: Applications of the schema construct. Social cognition. 1989;7:113–136. [Google Scholar]
- Janoff-Bulman R. Shattered assumptions: Towards a new psychology of trauma. New York: Free Press; 1992. [Google Scholar]
- Janoff-Bulman R, Yopyk DJ. Random outcomes and valued commitments: Existential dilemmas and the paradox of meaning. In: Greenberg J, Pyszcznski T, Koole SL, editors. Handbook of experimental existential psychology. New York: Guilford Press; 2004. [Google Scholar]
- Kaler ME, Frazier PA, Anders SL, Tashiro T, Tomich P, Tennen H, Park CL. Assessing the psychometric properties of the World Assumptions Scale. Journal of Traumatic Stress. 2008;21:326–332. doi: 10.1002/jts.20343. [DOI] [PubMed] [Google Scholar]
- Kessler R, Sonnega A, Bromet E, Hughes M, Nelson C. Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry. 1995;52:1048. doi: 10.1001/archpsyc.1995.03950240066012. [DOI] [PubMed] [Google Scholar]
- Kubany ES, Haynes SN, Leisen MB, Owens JA, Kaplan A, Burns K. Development and preliminary validation of the traumatic life events questionnaire (TLEQ) Psychological Assessment. 2000;12:210–224. doi: 10.1037//1040-3590.12.2.210. [DOI] [PubMed] [Google Scholar]
- Landau MJ, Johns M, Greenberg J, Pyszczynski T, Martens A, Goldenberg JL, et al. A function of form: Terror management and structuring the social world. Journal of Personality and Social Psychology. 2004;87:190–210. doi: 10.1037/0022-3514.87.2.190. [DOI] [PubMed] [Google Scholar]
- Norris FH, Hamblen JL. Standardized self-report measures of civilian trauma and PTSD. In: Wilson JP, Keane TM, editors. Assessing psychological trauma and PTSD. New York: Guilford Press; 2004. pp. 63–102. [Google Scholar]
- O’Donnell ML, Creamer M, Pattison P. Posttraumatic stress disorder and depression following trauma: Understanding comorbidity. American Journal of Psychiatry. 2004;161:1390–1396. doi: 10.1176/appi.ajp.161.8.1390. [DOI] [PubMed] [Google Scholar]
- Ozer EJ, Best SR, Lipsey TL, Weiss DS. Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin. 2003;129:52–73. doi: 10.1037/0033-2909.129.1.52. [DOI] [PubMed] [Google Scholar]
- Ozer EJ, Weiss DS. Who develops posttraumatic stress disorder? Current Directions in Psychological Science. 2004;13:169–172. [Google Scholar]
- Park CL. Making sense of the meaning literature: An integrative review of meaning making and its effects on adjustment to stressful life events. Psychological Bulletin. 2010;136:257–301. doi: 10.1037/a0018301. [DOI] [PubMed] [Google Scholar]
- Park CL, Folkman S. Meaning in the context of stress and coping. Review of General Psychology. 1997;1:115–144. [Google Scholar]
- Pyszczynski T, Greenberg J, Solomon S. A dual-process model of defense against conscious and unconscious death-related thoughts: An extension of terror management theory. Psychological Review. 1999;106:835. doi: 10.1037/0033-295x.106.4.835. [DOI] [PubMed] [Google Scholar]
- Pyszczynski T, Greenberg J, Solomon S, Arndt J, Schimel J. Why do people need self-esteem? A theoretical and empirical review. Psychological Bulletin. 2004;130:435–468. doi: 10.1037/0033-2909.130.3.435. [DOI] [PubMed] [Google Scholar]
- Pyszczynski T, Kesebir P. Anxiety buffer disruption theory: A terror management account of Posttraumatic Stress Disorder. Anxiety, Stress, and Coping. doi: 10.1080/10615806.2010.517524. (in press) [DOI] [PubMed] [Google Scholar]
- Radloff LS. The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement. 1977;1:385–401. [Google Scholar]
- Rosenberg M. Society and the adolescent self-image. Princeton, NJ: Princeton University Press; 1965. [Google Scholar]
- Rosenblatt A, Greenberg J, Solomon S, Pyszczynski T. Evidence for terror management theory: I. The effects of mortality salience on reactions to those who violate or uphold cultural values. Journal of Personality and Social Psychology. 1989;57:681–690. doi: 10.1037//0022-3514.57.4.681. [DOI] [PubMed] [Google Scholar]
- Schimel J, Hayes J, Williams T, Jahrig J. Is death really the worm at the core? Converging evidence that worldview threat increases death-thought accessibility. Journal of Personality and Social Psychology. 2007;92:789–803. doi: 10.1037/0022-3514.92.5.789. [DOI] [PubMed] [Google Scholar]
- Simon L, Arndt J, Greenberg J, Pyszczynski T, Solomon S. Terror management and meaning: Evidence that the opportunity to defend the worldview in response to mortality salience increases the meaningfulness of life in the mildly depressed. Journal of Personality. 1998;66:359–382. doi: 10.1111/1467-6494.00016. [DOI] [PubMed] [Google Scholar]
- Simon L, Greenberg J, Harmon-Jones E, Solomon S. Mild depression, mortality salience, and defense of the worldview: Evidence of intesified terror management in the mildly depressed. Personality and Social Psychology Bulletin. 1996;22:81–90. [Google Scholar]
- Solomon S, Greenberg J, Pyszczynski T. A terror management theory of social behavior: The psychological functions of self-esteem and cultural worldviews. Advances in Experimental Social Psychology. 1991;24:93–159. [Google Scholar]
- Solomon S, Greenberg J, Pyszczynski T, Koole SL. The cultural animal: Twenty years of terror management theory and research. In: Greenberg J, Koole S, Pyszczynski T, editors. Handbook of experimental existential psychology. New York: Guilford Press; 2004. p. 13. [Google Scholar]
- Weathers F, Litz B, Herman D, Huska J, Keane T. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. Paper presented at the Annual Convention of the International Society for Traumatic Stress Studies; San Antonio, TX. Oct, 1993. [Google Scholar]
- Wheeler MA, Stuss DT, Tulving E. Toward a theory of episodic memory: The frontal lobes and autonoetic consciousness. Psychological Bulletin. 1997;121:331–354. doi: 10.1037/0033-2909.121.3.331. [DOI] [PubMed] [Google Scholar]
- Wong PTP. Implicit theories of meaningful life and the development of the Personal Meaning Profile. In: Wong PTP, Fry PS, editors. The human quest for meaning: A handbook of psychological research and clinical applications. London: Erlbaum; 1998. pp. 111–140. [Google Scholar]