

Abstract
Patient: Male, 48
Final Diagnosis: Chordoma
Symptoms: —
Medication: —
Clinical Procedure: —
Specialty: Neurology
Objective:
Challenging differential diagnosis
Background:
Fluorodeoxyglucose positron emission tomography (FDG-PET) has been used in imaging and staging of malignancies including sacral chordomas.
Case Report:
The author’s report describes the coincident pathological diagnosis of sarcoidosis in a 48-year-old male patient with a recurrent sacral chordoma. Chordoma is a low grade malignancy with frequent systemic metastases in advanced disease. Both metastases and sarcoidosis may be high FDG uptake. Unexpected PET findings need to be biopsied in order to make appropriate clinical decision in the management of chordoma.
Conclusions:
Lymph nodes involvement in sarcoidosis and neoplastic disease can have similar FDG-PET manifestations.
Key Words: inflammation, imaging, granuloma, notochord
Background
FDG-PET has been used for diagnosis and staging of different malignancies including chordoma [1]. Chordoma is rare, highly recurrent, locally aggressive malignant tumor, originating from remnants of notochord. Metastases without local recurrence of primary neoplasm are extremely rare and most frequently seen at lungs (48%), bones (26%) and liver. Sporadic cases of metastases to CNS, lymphatic organs and skin have been reported [2]. Here, we report a rare case of 48-year-old Caucasian man with recurrent chordoma and lymph node involvement by sarcoidosis, which mimicked appearance of metastatic disease in PET-CT, scan.
Case Report
A 48-year-old man with a history of surgical resection for sacral chordoma in March 2011, presented to the clinic with recurrent sacrococcygeal pain in June 2012. Lumbosacral MRI was performed and showed a 0.5×0.8×1.0 cm, T2 hyper intense lesion, located in sacrococcygeal region, which was consistent with recurrent chordoma (Figure 1).
Figure 1.
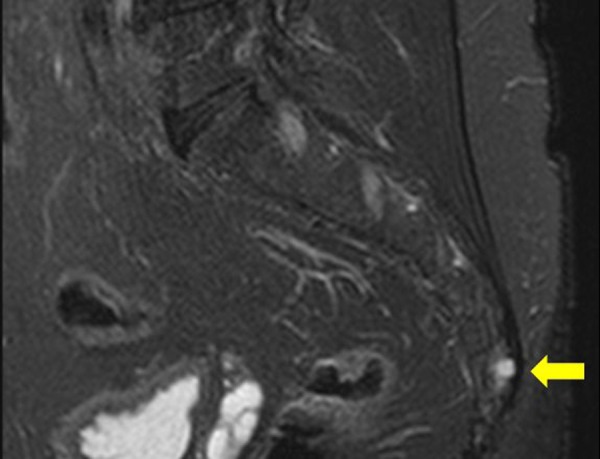
The sagittal T2 weighted MRI image of sacrococcygeal region, shows a small high signal lesion in the previous surgical site in the lower coccyx (arrow) consistent with recurrent chordoma.
Therefore, patient underwent a whole body PET-CT scan for staging. On PET-CT scan FDG avid lymph nodes in the left external iliac and bilateral femoral chains were detected (Figure 2).This raised the suspicions for a tumor metastasis to adjacent lymph nodes. The patient underwent open lymph node biopsy with pathology that unexpectedly revealed noncaseating epithelioid granuloma without evidence for malignant cells (Figure 3).
Figure 2.
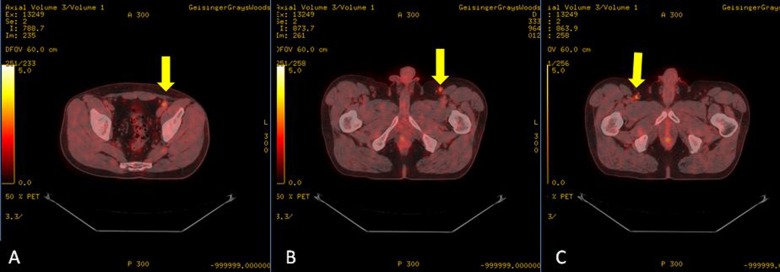
Axial FDG-PET/CT images of patient demonstrates high FDG uptake lymph nodes in the left iliac chain(SUV: 2.9) (A), the left femoral chain(SUV: 2.7) (B), and the right femoral chain (SUV: 2.9) (C).
Figure 3.
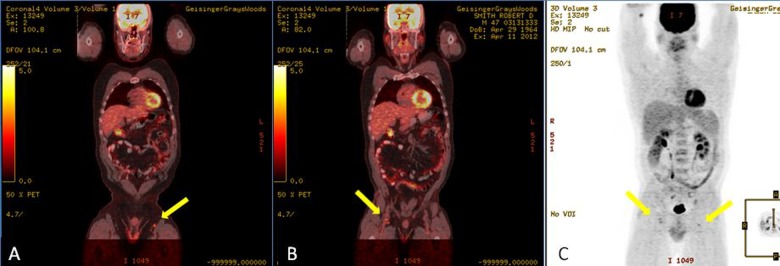
Sagittal FDG-PET/CT (A, B), and PET (C) images of the patient illustrate high FDG-uptake lymph nodes in the iliac and femoral chain of patient.
The patient underwent an en-bloc resection of soft tissue of the buttocks and peri-rectal region, with distal sacrectomy (S4–5). The surgical specimen pathology showed chordoma cells in the bone and further non-caseating epithelioid granulomas in the bone marrow consistent with diffuse sarcoidosis (Figure 4).
Figure 4.
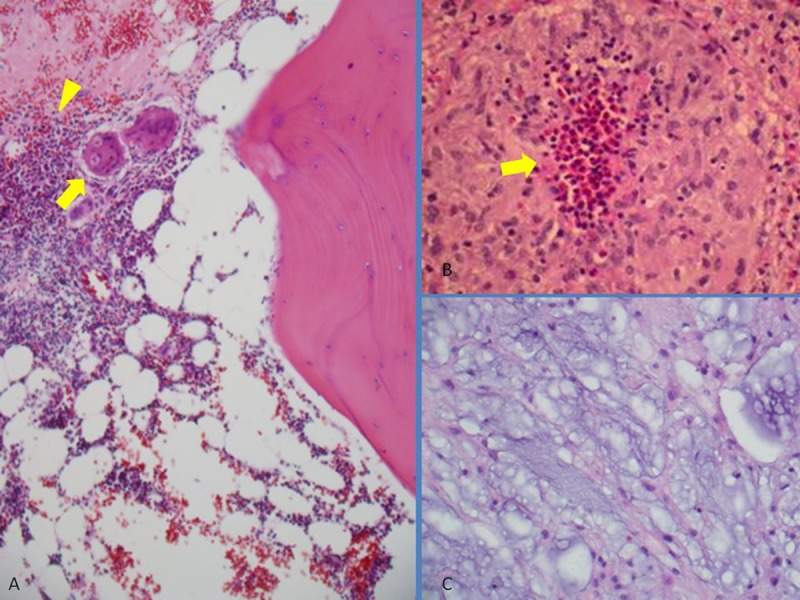
Photomicrographs of H&E staining images show: Astroid cells (arrow), and epithelioid granuloma (arrowhead) in the bone marrow (A), tumoral cells in the resected cocygeal bone (C), and epithelioid granuloma (arrow)in the resected lymph node (B).
Discussion
Two cases have been reported in the literature in which malignant tumor was accompanying by high FDG-uptake sarcoidosis lesions. The first was primary rectal cancer and accompanying high FDG-uptake sarcoidosis lesions in the bone [3], and the second was primary carcinoid tumor of the lung coincident with high FDG-uptake sarcoidosis of the bone marrow [4]. However, coincidence of chordoma and sarcoidosis has not yet been reported in the literature.
Sarcoidosis can be intensely FDG avid in PET scan, and thus, it may mimic the diagnosis of metastatic neoplastic disease. Combination of FDG-PET and FMT-PET(fluorine methyl tyrosine) scanning [5] or dual time point FDG-PET imaging [6] are reported as promising techniques in differentiating malignant from benign inflammatory diseases such as sarcoidosis.
Conclusions
Lymph node involvement in sarcoidosis is rare but can lead to false-positive appearance of metastatic disease in PET-CT scan.
Footnotes
Statement
This is no financial or material support to disclose and acknowledge.
References:
- 1.Thornton E, Krajewski KM, O’Regan KN, et al. Imaging features of primary and secondary malignant tumours of the sacrum. Br J Radiol. 2012;85:279–86. doi: 10.1259/bjr/25247602. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Walcott BP, Nahed BV, Mohyeldin A, et al. Chordoma: current concepts, management, and future directions. Lancet Oncol. 2012;13:e69–76. doi: 10.1016/S1470-2045(11)70337-0. [DOI] [PubMed] [Google Scholar]
- 3.Montini KM, Tulchinsky M. False-positive bone metastases on PET/CT secondary to sarcoidosis in a patient with rectal cancer. Clin Nucl Med. 2012;37:307–10. doi: 10.1097/RLU.0b013e31823eaaf0. [DOI] [PubMed] [Google Scholar]
- 4.Baldini S, Pupi A, Di Lollo S, et al. PET positivity with bone marrow biopsy revealing sarcoidosis in a patient in whom bone marrow metastases had been suspected. Br J Haematol. 2008;143:306. doi: 10.1111/j.1365-2141.2008.07288.x. [DOI] [PubMed] [Google Scholar]
- 5.Kaira K, Oriuchi N, Otani Y, et al. Diagnostic usefulness of fluorine-18-alpha-methyltyrosine positron emission tomography in combination with 18F-fluorodeoxyglucose in sarcoidosis patients. Chest. 2007;131:1019–27. doi: 10.1378/chest.06-2160. [DOI] [PubMed] [Google Scholar]
- 6.Cheng G, Torigian DA, Zhuang H, Alavi A. When should we recommend use of dual time-point and delayed time-point imaging techniques in FDG PET? Eur J Nucl Med Mol Imaging. 2013;40(5):779–87. doi: 10.1007/s00259-013-2343-9. [DOI] [PubMed] [Google Scholar]