

Abstract
Even 32 years after its first introduction shockwave lithotripsy (SWL) remains a matter of discussion and controversy. Since the first SWL in 1980, millions of treatments have been performed worldwide. To this day SWL remains the least invasive of all stone treatments and is considered the treatment modality of first choice for the majority of urinary stones. Despite the massive scale on which SWL is performed in a wide range of indications, complication rate has always remained very low and usually limited to minor side effects and complications. The introduction of affordable multifunctional lithotripters has made SWL available to more and more departments of urology worldwide. Still many centers are disappointed with the treatment results and concerned about the adverse tissue effects. In this SWL proves to be the victim of its uninvasiveness and its apparent ease of practice. Urologists need proper skill and experience; however, to adequately administer shockwaves in order to improve outcome. This aspect is too often minimized and neglected. Apart from this the power of shockwaves often is underestimated by operators of shockwave machines. Basic knowledge of the physics of shockwaves could further reduce the already minimal adverse tissue effects. Good training and coaching in the administration of shockwaves would no doubt lead to a renaissance of SWL with better treatment results and minimal adverse tissue effects.
Keywords: ESWL, extracorporeal shockwaves, stone management
HISTORIC PERSPECTIVE
Stone disease has been known to mankind for thousands of years: The existence of bladder stones was already documented in ancient Egypt thousands of years BC.
Hippocrates’ oath (ca 460 – ca 370 BC) contains the phrase “I will not cut for the stone, even for the patients in whom the disease is manifest; I will leave this operation to be performed by practitioners”, indicating, that lithotomy for bladder calculi was the province of specialized surgeons.
In the Sushruta Samhita which dates from the 3rd or 4th century AD Sushruta discussed urinary stones, their varieties, signs and symptoms, surgical extraction of bladder stones and the complications associated with these interventions.
In medieval times (perineal) lithotomy for bladder stones was performed by often travelling lithotomists. In France many of them were monks.
Transurethral lithotripsy of a bladder calculus was first performed by Jean Civiale, a French surgeon (1792-1867).
For centuries open surgery and transurethral (endoscopic) surgery were the primary treatment modalities for urinary stones.
The almost simultaneous introduction in the 1980s of more sophisticated endourological techniques (URS, PNL) and extracorporeal shockwave lithotripsy (SWL) thoroughly revolutionized modern stone management.
Following extensive research that started as early as 1963, the first human extracorporeal lithtotripsy was performed on February 07, 1980 by Christian Chaussy, Bernd Forssmann and Dieter Jocham using a Dornier HM1 lithotriptor.[1,2,3]
In 1983 the First serial Dornier HM3 lithotriptor was installed in the Department of Urology of Prof. Dr. F. Eisenberger at the Katharinen Hospital in Stuttgart. In March 1984, Dr. Daniel M. Newman and Dr. James Lingeman started operating the first Dornier HM3 in the US at the Methodist Hospital in Indianapolis.[4].
The experience with this new treatment modality proved so successful that there was a rapid expansion of the indications and more and more Dornier HM3 lithotriptors were installed worldwide.
The Dornier HM3 was a large, expensive machine; however, with several drawbacks that limited extracorporeal lithtotripsy to specialized high volume stone centers:
High capital investment and high running costs
“dedicated” to stone treatment only → high cost per treatment
Important spacial requirements
Treatments under full anesthesia
Stones in the bony pelvis difficult or impossible to treat
Only bulky and expensive X-ray system to localize the stones
This prompted several companies to construct second and third generation lithotripters that remedied most of these drawbacks:
More modest capital investment and lower running costs
Less space needed
“anesthesia-free” treatments
Both ultrasound and fluoroscopy to localize stones
Versatile targeting and positioning to allow treatments at all levels of the tract
Multifunctionality: Constructed to also allow endourological interventions on the same machine
The introduction of multifunctional lithotripters suitable for both SWL and endourological procedures was a major breaktrough as it allowed high-quality multimodal treatment of urinary stones on the same equipment. This way modern stone management in all its aspects became feasible in smaller centers with an adequate patient load.
The rapid propagation of extracorporeal lithotripsy in more and more smaller centers; however, resulted in a reduction of the number of patients treated per center and/or per urologist.
This had and has a number of less desired consequences:
increased cost per treatment → tendency to invest in low cost technology
dilution of experience
less investment in proper training of urologists operating lithotriptors
poorer results with SWL
At the same time and also induced by to the often poorer results with SWL, in many centers interest and training in endourological techniques (URS, PNL, RIRS) increased.[5,6]
These evolutions undermined the proper value of SWL in modern stone management, which, according to the guidelines of AUA and EAU, still remains based on a judicious combination of endourological techniques and SWL.
Therefore, a “rehabilitation” of SWL seems in order.[7]
EVOLUTION IN INDICATIONS
At its first introduction indications for extracorporeal lithotripsy were very limited:
A radio-opaque stone smaller than a cherry pip in the renal pelvis
Absence of obstruction in the urinary tract distal to the stone
Absence of urinary tract infection
Absence of comorbidities.
The indication area expanded rapidly and at present time stone therapy guidelines of international expert boards (AUA, EAU) consider SWL to be the primary treatment modality in most stone types. In some indications endourological techniques yield comparable or better results as compared to SWL. All guidelines, however, stress the complimentarity of both SWL and endourology in modern stone management.
Therefore, modern stone centers need to be proficient both in SWL and endourology.
Absolute contraindications remain pregnancy, untreated urinary tract infection, untreated obstruction distal to the stone treated and disorders of coagulation (uncorrected bleeding diathesis or use of anticoagulants).
EVOLUTION IN LITHOTRIPTER TECHNOLOGY[7,8]
The first lithotripters were “dedicated” lithotripters, meaning their use was limited to extracorporeal lithotripsy only.
This reserved their installation and use to high-volume stone centers.
As the initial experience proved SWL to be reproducible and safe, the marketplace demanded less expensive machines that ideally could also be used for other purposes than SWL. The industry answered with the construction of multifunctional machines that can be used both for SWL and the performance of endourological procedures.
SHOCKWAVE SOURCES
The original Dornier HM3 and several other first generation machines were equipped with an electrohydraulic shockwave source.
An electrohydraulic SW-source carries several disadvantages, the most important being:
Limited life span of the electrodes → increased running costs
Electrode wear leads to variations in energy output and focal instabilities ("jitter").[9]
To compensate both for electrode wear and for the “jitter” effect arising from electrode wear EDAP-TMS introduced the electroconductive shockwave generation. In this system the electrode is immersed in a highly conductive solution instead of degassed water and the interelectrode distance can be adjusted to compensate for electrode wear.[7,10] This electrode system has an extended lifespan of up to 40 000 shocks.
In an electrohydraulic SW-source the shockwaves are generated in the first focus of a semiellipsoid reflector which then focuses the shockwaves into the second focus (F2) of this semiellipsoid reflector. This F2 is the therapeutic focus.
Wolf and EDAP almost simultaneously developed a piezoelectric shockwave source.
In a piezoelectric SW-source several dozen to several thousand piezoceramic platelets are arranged on a dish that directs the energy of all ceramic elements toward the therapeutic focus.
A piezoelectric shockwave source is a direct focusing system (DFL = direct focusing lithotripsy). All ceramic elements are directed toward the therapeutic focus and the combined energy of their simultaneous discharge delivers the necessary energy to fragment a stone. To increase the energy output without the need to enlarge the dish the Wolf Piezolith 3000 has a double layer of piezoceramic elements.
Piezoelectric SW-sources have a small focus with high peak pressure. The retreatment rate with piezoelectric SW-sources is usually high with a correspondingly lower effectiveness quotient (EQ).[7,8]
The large diameter of the dish containing the piezoceramic elements makes its incorporation in a multifunctional machine difficult.
Most modern multifunctional lithotripters are equipped with an electromagnetic shockwave source. Apart from a performance that equals or even betters the performance of the Dornier HM3, still considered the “Gold Standard” in SWL, electromagnetic SW-sources have a number of added advantages:
Consistent quality of the SW throughout the lifetime of up to 1 000 000 shocks
Easily incorporated in a multifunctional machine
Anesthesia-free treatments
Low maintenance and running costs.
In the electromagnetic shockwave emitters (EMSE) of Dornier and Siemens, the shockwaves are focused by an acoustic lens. Storz uses an electromagnetic cylinder source with a parabolic reflector to focus the shockwaves.
Shockwaves are acoustic waves or pressure waves. They travel through media with alternating compression and decompression of these media. At interfaces between media with differences in acoustic impedance absorption, reflection or refraction of the travelling SW can occur.
The physics of shockwaves are quite complex.[11] and still not fully understood.
Important parameters are: Aperture Angle α, Peak Pressure p +, negative pressure phase p-, Focus Size (-6 dB Focus), Energy Flux Density (ED), Effective Energy (E12 mm).
All these parameters are interdependent.
A key determinant of a shockwave system is the Aperture Angle α which determines Maximum Peak Pressure p+, Focus Size and Energy Flux Density (ED) [Figure 1].
Figure 1.
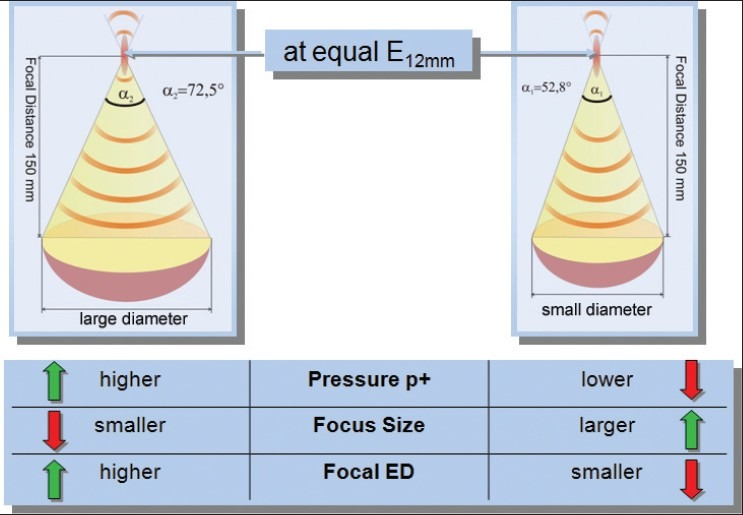
Aperture angle α and its relation to Pressure p+, Focus size and Focal Energy Denisity (ED).
The Peak Pressure p+ only represents the situation in the focus, which is a single point in an extended field. Peak Pressure is not a measure for the disintegration capacity of a lithotripter. The negative phase of the shockwave (p-) causes tensile stress and is the main cause of cavitation.
Energy Flux Density is an important factor in the occurrence of biological side effects of SW.
The Effective Energy E12 mm is the energy per shockwave pulse that is transmitted through a circular area of 12 mm in diameter. This 12-mm circular area refers to a typical stone of 12 mm diameter. There is a good correlation between E12 mm and the disintegration capacity of a lithotripter.
The ideal focus size of a lithotripter remains a controversial point.[12,13] The focus of current lithotripters is cigar shaped.
The ideal focus would be pherical with a size exactly matching the size of the stone treated. At this moment this is not possible technically. Some companies attempt to adapt the focus size to the stones. Storz introduced the Dual Focus Technology. The Wolf Piezolith 3000 features a Triple Focus.
The clinical relevance of the variable focus concepts still needs to be confirmed.
Shockwaves interact with stones through a combination of four different mechanisms: Hopkinson effect, cavitation, quasistatic squeezing and dynamic fatigue[8][Graph 1].
Graph 1.
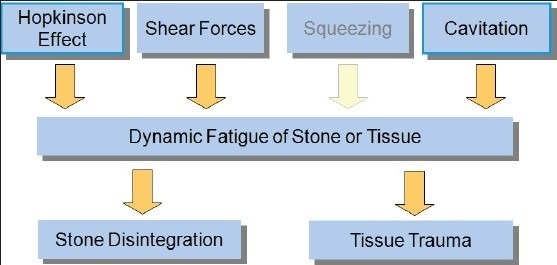
Bioeffects of shockwaves
Although important in the process of stone comminution, cavitation is considered the main culprit in the occurrence of adverse tissue effects caused by shockwaves.
The negative phase of the pressure wave (p-) produces a tensile wave that is considered the most important factor in cavitation.
In the Twinhead lithotripter (FMD, USA) dual shockwave sources are used to create the dual pulse technology.[14,15] The rationale in this concept is, that “filling” the negative part of the pressure wave with a positive pressure pulse would theoretically result in improved fragmentation and reduced cavitation with reduced parenchymal damage.
To enhance quasistatic squeezing Eisenmenger[16,17] pioneered the idea of large-focus/low-pressure lithotripters.[18] Also this idea remains in need of significant clinical data.
In a world with an ever increasing proportion of obese patients modern litotropters also need a shockwave source with a maximal treatment depth that will allow treatment of these obese patients. Ranging from 130 to 170 mm, a maximal treatment depth of at least 150 mm seems to become a necessity.
COUPLING
Coupling of the shockwave source is an extremely important issue.[7,11,18] At interfaces with different acoustic impedance the travelling shockwave is influenced by absorption, reflection or refraction.
Hence the total immersion of the patient in a waterbath (Dornier HM3) was the ideal coupling system as there is minimal difference in acoustic impedance between the human body and the surrounding degassed water.
Several experiments showed a dramatic reduction in fragmentation efficacy when air bubbles were included in the coupling area.[19,20,21,22]
It is generally advisable to use a proper amount of a low viscosity ultrasound gel and to remove air bubbles from the coupling area.[23]
Dornier is currently evaluating the use of a camera in the therapy head to observe the coupling area in order to adequately remove air bubbles from the coupling area.[19]
IMAGING
The success of SWL is largely dependent on adequate imaging.
High quality imaging is indispensable for localization and targeting of the stones, monitoring of treatment progress and identification of fragmentation. Apart from this treatment strategies are to an important extend defined by the available imaging modalities.
Modern multifunctional machines should be equipped with both fluoroscopy and ultrasound [Figure 2].
Figure 2.

Targeting a stone simultaneously using fluoroscopy and ultrasound
A large image intensifier (16”) or ideally a Flat Panel Detector (FPD) will offer excellent imaging both in SWL and endourologic procedures.
Ultrasonic targeting in SWL not only reduces radiation exposure but the great advantage of real time imaging is very useful in adequate adjustment of targeting and evaluation of fragmentation. A spectral Doppler signal (e.g., Dornier Gemini) can provide hit and miss information.[24]
PATIENT TABLE
In most stone centers a “dedicated” lithotripter no longer is economically feasible. Consequently most modern departments invest in a multifunctional machine. As one of the key components in the comfortable performance of endourological procedures the patient table of a multifunctional workstation needs to fulfill a number of requirements: Radio-translucent table top, high load capacity, maximal accessibility, isocentric Trendelenburg and anti-Trendelenburg positions, comfortable lowest position, etc.
EVOLUTION IN THE PRACTICE OF LITHOTRIPSY
For a very long time the complexity of shockwave administration has been underestimated. This underestimation by less experienced operators of the potentially destructive power of shockwaves and the proper techniques to administer them accurately and safely all too often results in disappointing results and a higher incidence of adverse tissue effects.
A better understanding of the complex physics of shockwaves now provides us a number of useful guidelines to improve results and reduce complications.
CONDITIONS FOR OPTIMIZED ENERGY TRANSFER
Imaging
In order to maximize the number of SW that actually hit the stone, adequate targeting using high quality imaging is of paramount importance.
Apart from an absence of radiation exposure ultrasound offers the great advantage of real time imaging with continuous monitoring of treatment progress.
Coupling
Good bubble-free coupling of the therapy head to the patient guarantees better energy transfer to the stone with improved fragmentation results. The importance of efficient coupling can not be emphasized too much. Poor coupling with inclusion of air bubbles probably is one of the more important causes of disappointing fragmentation results.
Analgesia[25,26]
By reducing the respiratory and bodily movements of the patient a good analgesia regimen increases the hit rate and thus improves outcome.
Main parameters in analgesia consumption are characteristics of the SW-source, number and energy level of SW, stone size and location, patient's age, sex and origin.
PULSE REPETITION FREQUENCY (PRF)
Although also indispensable in stone fragmentation, cavitation effects are considered the most important causes of adverse tissue effects.
A higher Pulse Repetition Frequency results in more cavitation bubbles and higher output energy of the lithotripter results in a longer lifespan of the cavitation bubbles.[27]
Several studies[28,29,30,31] demonstrate that a slower PRF improves outcome: Better fragmentation, better stone-free rates (SFR), reduced cavitation-related adverse tissue effects.
Apart from improving outcome a slower PRF also improves cost-effectiveness and overall efficiency.[32]
VOLTAGE STEPPING OR RAMPING
A gradual increase in the power output of the lithotripter ("voltage stepping or ramping") improves stone fragmentation and reduces collateral damage to the renal parenchyma.[33,34,35]
“Preloading” the kidney with a low energy dose of 100-500 SW prior to the actual ramping could also significantly reduce hemorrhagic lesions in the treated kidney[36].
A short treatment pause of 1-2 minutes following this preloading could further enhance this protective effect.
MEDICAL EXPULSIVE THERAPY (MET)
The administration of an α-blocker (Tamsulosin) is considered useful in enhancing stone fragment clearance following SWL.[37]
TRAINING
Despite the fact, that newer electromagnetic machines in experienced hands perform equally good or even better than the Dornier HM3 many centers are disappointed with the poorer results with their machine. A number of factors are responsible for this. First of all the complexity of SW-administration is often underestimated by new users. Where the Dornier HM3-users were extensively trained to operate their machine, newer machines are often considered “plug and play” and new users receive little or no training. It is therefore imperative, that lithotripter users have a basic knowledge of shockwave physics and receive extensive training in imaging, positioning and targeting, coupling, treatment strategies,…
They should also be aware of the mechanisms that lead to adverse tissue effects and the ways to avoid them.
LONG-TERM SIDE EFFECTS
An initial study by Krambeck et al. identified a higher risk of developing hypertension or diabetes mellitus in patients treated by SWL.[38] This was never confirmed in other studies.[39,40,41,42,43]
It is now suggested, that stone disease in itself and the metabolic disorders associated with it may be responsible for changes in blood pressure and the higher incidence of diabetes mellitus regardless of any stone treatment modality.[43]
PERFORMANCE OF LITHOTRIPTERS
It proves very difficult to compare the performance of lithotripters.
The Effectiveness Quotients (EQ, EQmod and EQext)[7,8,44] provide a useful quantification of stone free rate (SFR), auxiliary procedure rate and retreatment rate enabling an evaluation of the performance of a lithotripter.
Apart from these quantifiable parameters a number of other nonquantifiable parameters prove equally important in the final outcome: Stone location, stone burden, stone composition, imaging, coupling, analgesia regimen, PRF, treatment strategies, etc.
Last but not least, and after being disregarded for a very long time, experience and skill of the lithotripter operator are regarded as key factors in success.[45,46] This again emphasizes the importance of proper training.
By some the Dornier HM3 continues to be considered the “Gold Standard” in SWL.
The far better results with the newer electromagnetic machines, however, prove this to be nothing more than a myth of the past.[7]
Apart from performing equally good or even better than the Dornier HM3, newer electromagnetic machines offer several added advantages: Lower capital costs and lower maintenance and running costs, smaller footprint, easier handling, anesthesia-free SWL-treatments and above all multifunctionality through the integration of extracorporeal lithotripsy and endourology in one single system.
THE IDEAL LITHOTRIPTER
The ideal lithotripter for most centers nowadays would be a multifunctional machine with a high performance SW-source, excellent imaging systems both fluoroscopic and ultrasonic, versatile coupling possibilities and a urologist-friendly patient table suitable for endourological procedures.
The high performance SW-source would have to have an ideal focal geometry and size with sufficient disintegration power (E12 mm), a prolonged lifetime without variations in focal energy or position, a wide range of energy output and an adequate maximal treatment depth (minimum 150 mm).
At this moment only electromagnetic sources meet most of these demands.
In order to treat stones at all levels of the urinary tract versatile coupling positions of the therapy head (above and under table) are an important asset [Figure 3].
Figure 3.

Coupling positions of the therapy head both above and under table (Dornier Gemini)
Both excellent fluoroscopic (large image intensifier or FPD) and ultrasonic imaging are crucial both in SWL and endourological procedures.
The ideal patient table is accessible over 360°, has a completely radiotranslucent carbon fiber table top, and has a high load capacity (up to 250 kg) to accommodate the ever increasing number of obese patients.
Finally, a well-trained, experienced and interested urologist should operate this machine. [Graph 2].
Graph 2.
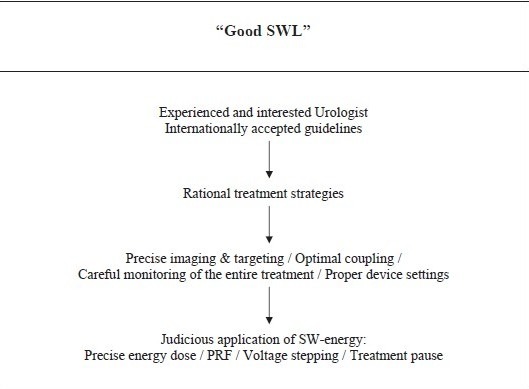
Principles of “Good SWL”
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Chaussy C, Brendel W, Schmiedt E. Extracorporeally induced destruction of kidney stones by shock waves. Lancet. 1980;2:1265–8. doi: 10.1016/s0140-6736(80)92335-1. [DOI] [PubMed] [Google Scholar]
- 2.Chaussy C, Schmiedt E, Jocham D, Brendel W, Forssman B, Walther V. First clinical experience with extracorporeally induced destruction of kidney stones by shock wave. J Urol. 1982;127:417–20. doi: 10.1016/s0022-5347(17)53841-0. [DOI] [PubMed] [Google Scholar]
- 3.Chaussy C, Schmiedt E, Jocham D, Eisenberger F, Walther V, Brendel W, et al. Extracorporeal shock wave lithotripsy-new aspect in the treatment of kidney stone disease. Basel: Karger; 1982. [Google Scholar]
- 4.Drach GW, Dretler S, Fair W, Finlayson B, Gillenwater J, Griffith D, et al. Report of the united states cooperative study of extracorporeal shock wave lithotripsy. J Urol. 1986;135:1127–33. doi: 10.1016/s0022-5347(17)46015-0. [DOI] [PubMed] [Google Scholar]
- 5.Knoll T, Alken P. Beyond SWL. New concepts for definitive stone removal. World J Urol. 2011;29:703–4. doi: 10.1007/s00345-011-0787-8. [DOI] [PubMed] [Google Scholar]
- 6.Knoll T, Fritsche HM, Rassweiler J. Medical and economic aspects of extracorporeal shock wave lithotripsy. Aktuelle Urol. 2011;42:363–7. doi: 10.1055/s-0031-1283805. [DOI] [PubMed] [Google Scholar]
- 7.Tailly GG. Lithotripsy systems. In: Smith AD, Preminger G, Badlani G, editors. Chapter 50 in Smith's Textbook of Endourology. Wiley: Blackwell; 2012. pp. 559–75. [Google Scholar]
- 8.Rasswelier JJ, Tailly GG, Chaussy C. Progress in Lithotriptor Technology. EAU Updates Series. 2005;3:17–36. [Google Scholar]
- 9.Rassweiler JJ, Bergsdorf T, Bohris C, Burkhardt M, Burnes L, Forssmann B, et al. Consensus: Shock wave technology and application - state of the art in 2010. In: Chaussy C, Haupt G, Jocham D, Köhrmann KU, editors. Therapeutic energy applications in urology II. Standards and recent developments. New York: Thieme Stuttgart; 2010. pp. 37–52. [Google Scholar]
- 10.Partheymüller P. Sonolth i-sys: The new standard in lithotripsy. In: Chaussy C, Haupt G, Jocham D, Köhrmann KU, editors. Therapeutic energy applications in urology II. Standards and recent developments. New York: Thieme Stuttgart; 2010. pp. 65–70. [Google Scholar]
- 11.Cleveland RO, McAteer JA. Physics of shockwave lithotripsy. In: Smith AD, Preminger G, Badlani G, Kavoussi L, editors. Chapter 49 in Smith's Textbook of Endourology. Wiley: Blackwell; 2012. pp. 529–58. [Google Scholar]
- 12.Wess O. Shock Wave Lithotripsy (SWL) and Focal Size. In: Chaussy C, Haupt G, Jocham D, Köhrmann KU, Wilbert D, editors. Applications in Urology: Standards and recent developments. Thieme Verlag: pp. 21–35. [Google Scholar]
- 13.Haecker A, Wess O. The role of focal size in extracorporeal shock wave lithotripsy. In: Loske A, editor. New Trends in Shock Wave Applications to Medicine and Biotechnology. Research Signpost. 2010. ISBN 978-81-308-0365-4. [Google Scholar]
- 14.Sheir KZ, Zabini N, Lee D, Teichman JM, Rehman J, Sundaram CP, et al. Evolution of synchronous twin-pulse technique for shockwave lithotripsy: Determination of optimal parameters for in vitro stone fragmentation. J Urol. 2003;170(6 Pt 1):2190–4. doi: 10.1097/01.ju.0000094188.69698.f8. [DOI] [PubMed] [Google Scholar]
- 15.Sheir KZ, Elhalwagy SM, Abo-Elghar ME, Ismail AM, Elsawy E, El-Diasy TA, et al. Evaluation of a synchronous twin-pulse technique for shock wave lithotripsy: A prospective randomised study of effectiveness and safety in comparison to standard single-pulse technique. BJU Int. 2007;101:1420–5. doi: 10.1111/j.1464-410X.2007.07357.x. [DOI] [PubMed] [Google Scholar]
- 16.Eisenmenger W. The mechanisms of stone fragmentation in SWL, Ultrasound. Med Biol. 2001;27:683–93. doi: 10.1016/s0301-5629(01)00345-3. [DOI] [PubMed] [Google Scholar]
- 17.Eisenmenger W, Du XX, Tang C, Zhao S, Wang Y, Rong F, et al. The first clinical results of “wide focus and low pressure” SWL. Ultrasound Med Biol. 2002;28:769–74. doi: 10.1016/s0301-5629(02)00507-0. [DOI] [PubMed] [Google Scholar]
- 18.Lingeman JE, McAteer JA, Gnessin E, Evan AP. Shock wave lithotripsy: Advances in technology and technique. Nat Rev Urol. 2009;6:660–70. doi: 10.1038/nrurol.2009.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bohris C, Roosen A, Dickmann M, Hocaoglu Y, Sandner S, Bader M, et al. Monitoring the coupling of the lithotripter head with skin during routine shock wave lithotripsy with a surveillance camera. J Urol. 2012;187:157–63. doi: 10.1016/j.juro.2011.09.039. [DOI] [PubMed] [Google Scholar]
- 20.Pishchalnikov YA, Neucks JS, VonDerHaar RJ, Pishchalnikova IV, Williams JC, Jr, McAteer JA. Air pockets trapped during routine coupling in dry head lithotripsy can significantly decrease the delivery of shock wave energy. J Urol. 2006;176(6 Pt 1):2706–10. doi: 10.1016/j.juro.2006.07.149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jain A, Shah TK. Effect of air bubbles in the coupling medium on efficacy of extracorporeal shock wave lithotripsy. Eur Urol. 2007;51:1680–7. doi: 10.1016/j.eururo.2006.10.049. [DOI] [PubMed] [Google Scholar]
- 22.Neucks JS, Pishchalnikov YA, Zancanaro AJ, VonDerHaar JN, Williams JC, Jr, McAteer JA, et al. Improved acoustic coupling for shock wave lithotripsy. Urol Res. 2008;36:61–6. doi: 10.1007/s00240-007-0128-y. [DOI] [PubMed] [Google Scholar]
- 23.Bergsdorf T, Chaussy C, Thüroff S. The relevance of coupling gel viscosity for efficient energy coupling in SWL. Poster (VP18-12) presented at the 27th WCE in. 2009:06–10. [Google Scholar]
- 24.Bohris C, Bayer T, Lechner C. Hit/miss monitoring of SWL by spectral Doppler ultrasound. Ultrasound Med Biol. 2003;29:705–12. doi: 10.1016/s0301-5629(02)00773-1. [DOI] [PubMed] [Google Scholar]
- 25.Tailly Poster MP15-09 presented at WCE Shanghai. 2008 [Google Scholar]
- 26.Chaussy, et al. Poster MP15-11 presented at WCE Shangai. 2008 [Google Scholar]
- 27.Huber P, Jochle K, Debus J. Influence of shock wave pressure amplitude and pulse repetition frequency on the lifespan, size and number of transient cavities in the field of an electromagnetic lithotripter. Phys Med Biol. 1998;43:3113–28. doi: 10.1088/0031-9155/43/10/029. [DOI] [PubMed] [Google Scholar]
- 28.Pishchalnikov YA, McAteer JA, Williams JC., Jr Effect of firing rate on the performance of shock wave lithotripters.2008 The Authors. BJU Int. 2008;102:1681–6. doi: 10.1111/j.1464-410X.2008.07896.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Chacko J, Moore M, Sankey N, Chandhoke PS. Does a slower treatment rate impact the efficacy of extracorporeal shock wave lithotripsy for solitary kidney or ureteral stones? J Urol. 2006;175:1370–4. doi: 10.1016/S0022-5347(05)00683-X. [DOI] [PubMed] [Google Scholar]
- 30.Weizer AZ, Zhong P, Preminger GM. Pearle MS, Guest, editors. New Concepts in Shock Wave Lithotripsy. Urologic Clinics of North America. 2007;34:375–82. doi: 10.1016/j.ucl.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 31.Skolarikos A, Alivizatos G, de la Rosette J. Extracorporeal shock wave lithotripsy 25 years later: Complications and their prevention. Eur Urol. 2006;50:981–90. doi: 10.1016/j.eururo.2006.01.045. [DOI] [PubMed] [Google Scholar]
- 32.Koo V, Beattie I, Young M. Improved cost-effectiveness and efficiency with a slower shockwave delivery rate. BJU Int. 2009;105:692–6. doi: 10.1111/j.1464-410X.2009.08919.x. [DOI] [PubMed] [Google Scholar]
- 33.Weizer AZ, Zhong P, Preminger GM. New concepts in shock wave lithotripsy. Urol Clin N Am. 2007;34:375–82. doi: 10.1016/j.ucl.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 34.Rassweiler JJ, Knoll T, Köhrmann KU, McAteer JA, Lingeman JE, Cleveland RO, et al. Shock wave technology and application: An update. Eur Urol. 2011;59:784–96. doi: 10.1016/j.eururo.2011.02.033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Maloney ME, Marguet CG, Zhou Y, Kang DE, Sung JC, Springhart WP, et al. Progressive increase of lithotripter output produces better in-vivo stone communution. J Endourol. 2006;20:603–6. doi: 10.1089/end.2006.20.603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Willis LR, Evan AP, Connors BA, Handa RK, Blomgren PM, Lingeman JE. Preventing of lithotripsy-induced renal injury by pretreating kidneys with low-energy shock waves. J Am Soc Nephrol. 2006;17:663–73. doi: 10.1681/ASN.2005060634. [DOI] [PubMed] [Google Scholar]
- 37.Losek RL, Mauro LS. Efficacy of tamsulosin with extracorporeal shock wave lithotripsy for passage of renal and ureteral calculi. Ann Pharmacother. 2008;42:692–7. doi: 10.1345/aph.1K546. [DOI] [PubMed] [Google Scholar]
- 38.Krambeck AE, Gettmann MT, Rohlinger AL, Lohse CM, Patterson DE, Segura JW. Diabetes mellitus and hypertension associated with shock wave lithotripsy of renal and proximal ureteral stones at 19 years of followup. J Urol. 2006;175:1742–7. doi: 10.1016/S0022-5347(05)00989-4. [DOI] [PubMed] [Google Scholar]
- 39.Sato Y, Tanda H, Kato S, Ohnishi S, Nakajima H, Nanbu A, et al. Shock wave lithotripsy for renal stones is not associated with hypertension and diabetes mellitus. Urology. 2008;71:586–91. doi: 10.1016/j.urology.2007.10.072. [DOI] [PubMed] [Google Scholar]
- 40.Eassa WA, Sheir KZ, Gad HM, Dawaba ME, El-Kenawy MR, Elkappany HA, et al. Prospective study of the long-tem effects of shock wave lithotripsy on renal function and blood pressure. J Urol. 2008;179:964–8. doi: 10.1016/j.juro.2007.10.055. [DOI] [PubMed] [Google Scholar]
- 41.Strohmaier WL, Schmidt J, Lahme S, Bichler KH. Arterial blood pressure following different types of urinary stone therapy. Eur Urol. 2000;38:753–7. doi: 10.1159/000020374. [DOI] [PubMed] [Google Scholar]
- 42.Krambeck AZ, LeRoy AJ, Patterson DE, Gettman MT. Longterm outcomes of percutaneous nephrolithotomy compared to shock wave lithotripsy and conservative management. J Urol. 2008;179:2233–7. doi: 10.1016/j.juro.2008.01.115. [DOI] [PubMed] [Google Scholar]
- 43.Chew BH, Zavaglia B, Sutton C, Masson RK, Chan SH, Hamidizadeh R, et al. Twenty-year prevalence of diabetes mellitus and hypertension in patients receiving shock-wave lithotripsy for urolithiasis. BJU Int. 2011;109:444–9. doi: 10.1111/j.1464-410X.2011.10291.x. [DOI] [PubMed] [Google Scholar]
- 44.Denstedt JD, Clayman RV, Preminger GM. Efficiency quotient as a means of comparing lithotripters. J Endourol. 1990;4(Suppl):S100. [Google Scholar]
- 45.Lorber G, Duvdevani M, Gofrit ON, Latke A, Katz R, Landau E, et al. What happened to shockwave lithotripsy during the past 22 years. A single-center experience? J Endourol. 2010;24:609–14. doi: 10.1089/end.2009.0152. [DOI] [PubMed] [Google Scholar]
- 46.Matlaga BR, Jansen JP, Meckley LM, Byrne TW, Lingeman JE. Treatment of ureteral and renal stones: A systematic review and meta-analysis of randomized, controlled trials. J Urol. 2012;188:130–7. doi: 10.1016/j.juro.2012.02.2569. [DOI] [PMC free article] [PubMed] [Google Scholar]