

Abstract
The role of percutaneous nephrostomy tube for drainage after percutaneous nephrolithotomy (PCNL) procedure has come under scrutiny in recent years. The procedure has been modified to use of small diameter tubes, ‘tubeless’ PCNL, and even ‘totally tubeless’ PCNL. A review of the available literature confirms that the chosen method of drainage after PCNL has a bearing upon the post-operative course. It is generally recognized now that small tubes offer benefit in terms of reduced post-operative pain and morbidity. Similarly, nephrostomy-free or ‘tubeless’ PCNL, using a double-J stent or ureteric catheter as alternative form of drainage, can be used with a favorable outcome in selected patients with the advantage of decreased postoperative pain, analgesia requirement, and hospital stay. Although the tubeless technique has been applied for extended indications as well, the available evidence is insufficient, and needs to be substantiated by prospective randomized trials. In addition, ‘totally tubeless’ approach has also been shown to be feasible in selected patients.
Keywords: Kidney stone, percutaneous nephrolithotomy, tubeless
INTRODUCTION
Since its introduction in 1976, percutaneous nephrolithotomy (PCNL) has evolved considerably as a result of continued search for improvement in technology and surgical skills toward minimizing postoperative pain and morbidity.[1] Postoperative placement of percutaneous drainage tube through the nephrostomy tract has been an integral part of the standard PCNL, under the belief that nephrostomy tube provides hemostasis along the tract, avoids urinary extravasation, and maintains adequate drainage of the kidney.[2] However, in recent years, it has been recognized that the purpose of the tube is only to maintain adequate drainage of the kidney. In addition, there has been a growing realization that substantial postoperative pain after PCNL is caused by nephrostomy tubes, leading to use of smaller tubes and introduction of “tubeless” approach which places a ureteral stent or catheter after PCNL in lieu of the nephrostomy tube. More recently, there have been several publications with “totally tubeless” approach, wherein no ureteral stent or catheter was employed. We performed a PUBMED database search to retrieve all published articles relating to nephrostomy tube in PCNL from 1976 till date, using the terms PCNL, tubeless, and nephrostomy tube. Cross-references from retrieved articles as well as articles from urology journals not indexed were also accessed.
LARGE-BORE VERSUS SMALL-BORE NEPHROSTOMY TUBE
Several studies have demonstrated the usefulness of small-bore nephrostomy tube (NT) in terms of reducing morbidity of percutaneous nephrolithotomy (PCNL).[3,4] Mini-PCNL was introduced with an aim to decrease morbidity associated with larger nephroscope and tubes.[5,6] Chan et al.[7] described mini-PCNL with 13 F nephroscope, followed by placement of 8 F NT.
Maheshwari et al.[8] performed a prospective study on 40 patients randomized between 28 F NT and 9 F pigtail catheter placed at the end of the procedure. They reported shorter duration of the urinary leak and hospital stay, with less pain and less need for analgesic support in pigtail nephrostomy group. In a meta-analysis of randomized controlled trials, Ni et al. found that the size of the NT correlates with postoperative discomfort.[9]
TUBELESS PCNL
Published data on tubeless PCNL is summarized in Table 1. Beginning as early as 1984, several reports have challenged the standard placement of a percutaneous drainage tube postoperatively. Wickham et al.[10] reported one-stage PCNL in 100 patients, where at the conclusion of case, no internal or external drainage tubes were used. However, Winfield et al.[11] subsequently reported two patients with complications after extraction of simple upper tract calculi. These patients experienced serious hemorrhage and urinary extravasation necessitating transfusion, internal stenting, and prolonged hospitalization. They recommended NT drainage during the first 24-48 h after percutaneous stone extraction, which was to become the standard practice subsequently.
Table 1.
Reports of tubeless PCNL
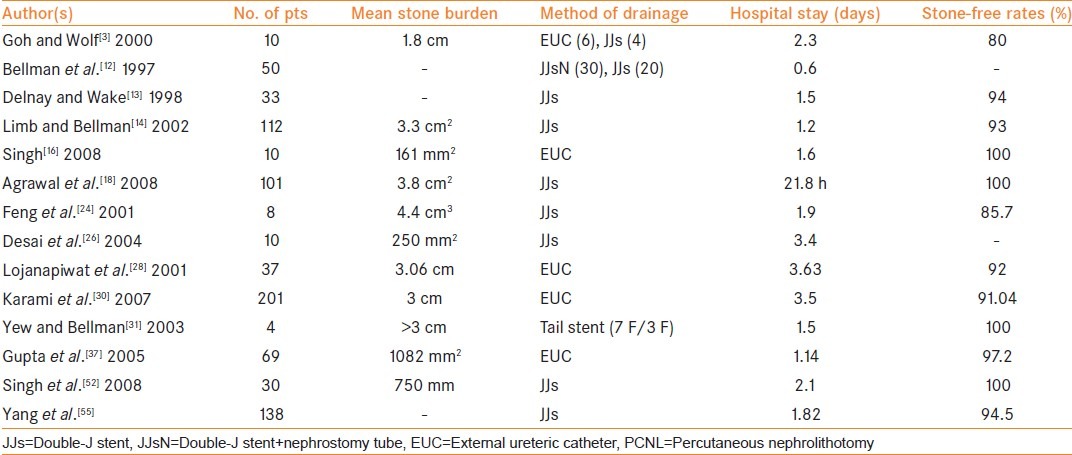
In 1997, Bellman et al.[12] presented “tubeless” percutaneous approach involving placement of an internal ureteral stent for drainage in place of NT. In their study, the hospitalization time, analgesia requirements, time to return to normal activity, and cost were significantly less with this new technique. Several subsequent reports confirmed the efficacy and safety of this technique. Delnay and Wake[13] reported a 94% stone-free rate with a mean length of stay of 1.5 days in 33 tubeless percutaneous procedures. In 2002, Limb and Bellman[14] reported a series of 112 patients who underwent tubeless percutaneous renal surgery using an internal ureteral stent. Patients stayed in the hospital for an average of 1.25 days and 93% stone-free rate was achieved.
Gupta et al.[15] found tubeless PCNL to be effective and safe in a study of 69 patients who underwent tubeless PCNL. Singh et al.,[16] in a study of 60 patients, found tubeless PCNL to be associated with minimal morbidity, shorter hospital stay, and less pain and analgesia requirement as compared to standard PCNL, without compromising effectiveness and safety. Shah et al.[17] reported feasibility of tubeless PCNL is in a study of 25 patients with a history of open renal surgery.
In the largest prospective randomized trial published yet, in 202 patients treated at our center, tubeless PCNL was found to have significant advantages over standard PCNL in terms of postoperative pain, morbidity, hospital stay, and period of convalescence.[18] The difference in average blood loss and urinary infection for the two groups was not statistically significant. The average hospital stay in the tubeless group was less than 24 h (21.8 ± 3.9 h) and was significantly shorter than that of the standard PCNL group (54.2 ± 5 h) (P > 0.01).
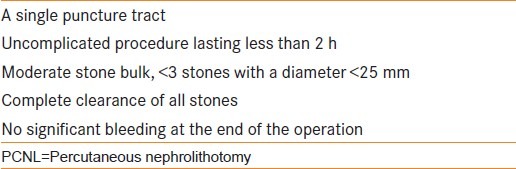
In most of these studies, the tubeless technique was applied on the basis of criteria that included careful selection of cases, no intraoperative complications, minimal bleeding, and complete clearance at the end of the procedure [Table 2]. In several single-center studies, the technique has also been reported successful in obese patients, children, recurrent stones, solitary kidneys, deranged renal function, and in staghorn stones requiring multiple access tracts, supracostal puncture, or bilateral simultaneous PCNL.[19,20,21,22] Degree of obstruction, anatomic variation of renal shape and position, and elevated serum creatinine were also not considered contraindications to tubeless PCNL.[23] However, for all these extended indications, the available evidence is insufficient, and needs to be substantiated by prospective randomized, preferably multi-centric trials.
Table 2.
Standard indications for tubeless PCNL
TUBELESS PCNL VERSUS SMALL-BORE TUBE
In a prospective randomized trial by Feng et al.[24] between standard PCNL, “mini-perc,” and tubeless PCNL, the tubeless technique was found to be associated with the least amount of morbidity and the greatest cost efficiency. Shah et al.[25] compared the outcome of tubeless PCNL with small-bore (8 F) nephrostomy drainage after PCNL. Although tubeless PCNL offered the advantages of decreased postoperative pain, analgesic requirement, and hospital stay, it was associated with stent-related discomfort in 39% of patients.
Desai et al.[26] compared postoperative outcomes among tubeless, small-bore, and large-bore nephrostomy drainage following PCNL in a prospective randomized study in 30 patients. There were 10 patients in each study group. They conclude that small-bore nephrostomy drainage may be a reasonable option in patients to avoid the incidence of stent dysuria.
A meta-analysis done by Shen et al.[27] compared the clinical efficacy and safety of NT-free and standard PCNL. Nine studies involving 547 patients were included. Patients were divided into four groups: NT-free group, small tube group (8-9 F), middle tube group (16-18 F), and large tube group (20-24 F). This meta-analysis showed that with regard to hospital stay and visual analog scale scores for postoperative pain on day 1, there was no significant difference between the NT-free group and the small tube group, but there were differences between the NT-free group versus the middle and large tube groups. No significant difference was found with regard to transfusion, fever, or infection, and the operative time between NT-free group and the other groups.
TUBELESS PCNL WITH OTHER MODIFICATIONS
A significant disadvantage of the technique of tubeless PCNL is the need for postoperative cystoscopy to remove the internal ureteral stent. Stent-induced dysuria is another problem associated with this procedure. To avoid these problems, additional variations of the tubeless procedures have been described.
Lojanapiwat et al.[28] and Mouracade et al.[29] reported tubeless procedure with placement of an external ureteral catheter in place of a double-J stent, and found significant reduction in the length of hospitalization and postoperative analgesic requirement, compared with control group of patients with routine placement of NT. Karami et al.[30] found tubeless PCNL with only an externalized ureteral catheter to be safe, effective, and economical with reduced postoperative discomfort. However, in tubeless PCNL using externalized ureteral catheter, it is difficult to keep ureteric catheter for long periods, as the discomfort of indwelling urethral and ureteric catheter may negate the benefits of a tubeless procedure.
To avoid the need for cystoscopy afterward, Bellman et al.[31] presented a modified tubeless procedure by placing a double-J stent with a tether exiting per urethra, which was used to pull the stent out in office setting. However, several patients removed their stents prematurely by inadvertently pulling on the tether. In a randomized trial comparing tubeless percutaneous nephrolithotomy with tailed stent with small-bore NT, Choi et al.[32] found that tubeless and small-bore procedure causes similar postoperative discomfort with somewhat quicker recovery in tubeless group. However, they also reported inadvertent dislodgment of stent in some of the patients in the tailed stent group.
TUBELESS PCNL WITH DOUBLE-J STENT WITH A PROXIMAL TETHER
A further modification of the technique involves placement of a double-J ureteral stent with a tether, which is attached to the proximal end of the stent placed in the renal pelvis, exiting the nephrostomy tract.[33] This allows the stent to be removed directly from the flank in the office setting without the need for cystoscopy.
The principle of the tether exiting from the flank also takes care of another limitation of tubeless PCNL, namely access to pelvi-calyceal system in case of need of a second-look procedure. At the time of the second-look procedure, the tether is used to pull the proximal end of the stent to the level of the skin, and a guidewire passed antegrade into the ureter, re-establishing access through the previous nephrostomy tract.
TOTALLY TUBELESS PCNL
Reports of totally tubeless PCNL are presented in Table 3. Totally tubeless approach was first reported by Wickham and coworkers.[9] After Winfield's unsuccessful trial with totally tubeless PCNL in two cases in 1986, this procedure was given up.[10] In recent years, there have been several successful reports of totally tubeless PCNL.[34,35,36,37,38]
Table 3.
Reports of totally tubeless PCNL
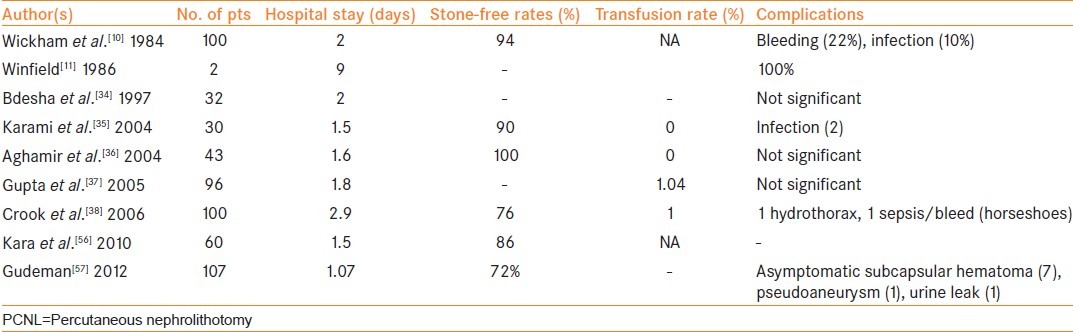
Crook et al.[38] performed a randomized controlled trial comparing totally tubeless PCNL with standard NT placement in 25 patients, and reported no differences in hemorrhage, infection, and other parameters. Mean length of stay was 2.3 versus 3.4 days (P > 0.05). Mandhani et al.[39] compared the outcome of tubeless percutaneous nephrolithotomy with or without double-J stent in 52 patients. Mean pain score, analgesic requirement, hospital stay, and incidence of urinary leak were comparable in both the groups. These studies concluded that PCNL without NT or stent was a safe and well-tolerated procedure in selected patients.
EARLY TUBE REMOVAL VERSUS TUBELESS PCNL
In two recent studies, Mishra et al.[40] and El Nahas[41] proposed removal of NT on the first postoperative day after PCNL, and compared it with tubeless PCNL. According to these studies, early tube removal after PCNL results in an equivalent analgesic requirement, hospital stay, and clearance rates, lower incidence of early hematuria, and preserves the option of check nephroscopy in case of residual fragments.
HEMOSTASIS IN TUBELESS PCNL
Two hemostatic agents have been commonly used in PCNL: Gelatin matrix hemostatic sealant (GMHS)[42,43] and fibrin glue.[44] Nagele and Schilling et al.[45,46] reported use of gelatin-thrombin-hemostatic sealant following mini-PCNL in a tubeless setting. Mikhail et al.[47] were the first to use fibrin glue as a hemostyptic sealant in 20 patients during PCNL. Several other studies have used fibrin glue for good effect.[48,49,50] Because of experimental evidence of the lithogenic properties of hemostatic agents implanted in the collecting system, an occlusion balloon is placed in the collecting system to prevent hemostatic agents from entering and causing possible obstruction.
Aghamir et al.[51] did not find decreased bleeding or urinary extravasation with oxidized cellulose (Surgicel®) to seal the working nephrostomy tract in totally tubeless PCNL. Singh et al.[52] reported safety and efficacy of using absorbable gelatin tissue hemosealant (Spongostan®) in tubeless PCNL. They observed lower wound soakage/discomfort in the gelatin-assisted tubeless PCNL group as compared to controls.
Jou et al.,[53] Aron et al.,[54] and Mouracade et al.[29] reported diathermy coagulation of the intra-renal bleeders and tract in patients of tubeless PCNL and reported that fulguration of visible intra-renal and tract bleeders is a simple, safe, and effective hemostatic adjunct.
CONCLUSION
The chosen method of drainage after PCNL certainly has a bearing upon the postoperative course. There has been a definite shift away from the conventional large tube drainage, with the recognition that small tubes offer benefit in terms of reduced postoperative pain and morbidity.
Nephrostomy-free or tubeless PCNL, or one of its modifications using an alternative form of drainage, can be used with a favorable outcome in selected patients, with the potential advantages of decreased postoperative pain, analgesia requirement, and hospital stay. Similarly, totally tubeless approach has also been shown to be safe and effective in selected cases.[57]
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Jones DJ, Russell GL, Kellett MJ, Wickham JE. The changing practice of percutaneous stone surgery. Review of 1000 cases 1981-1988. Br J Urol. 1990;66:1–5. doi: 10.1111/j.1464-410x.1990.tb14852.x. [DOI] [PubMed] [Google Scholar]
- 2.Paul EM, Marcovich R, Lee BR, Smith AD. Choosing the ideal nephrostomy tube. BJU Int. 2003;92:672–7. doi: 10.1046/j.1464-410x.2003.04454.x. [DOI] [PubMed] [Google Scholar]
- 3.Wolf JS., Jr Nephrostomy tube after percutaneous nephrolithotomy: Large-bore or pigtail catheter.[editorial]? J Endourol. 2000;14:737. doi: 10.1089/end.2000.14.735. [DOI] [PubMed] [Google Scholar]
- 4.Pietrow PK, Auge BK, Lallas CD, Santa-Cruz RW, Newman GE, Albala DM, et al. Pain after percutaneous nephrolithotomy: Impact of nephrostomy tube size. J Endourol. 2003;17:411–4. doi: 10.1089/089277903767923218. [DOI] [PubMed] [Google Scholar]
- 5.Jackman SV, Docimo SG, Cadeddu JA, Bishoff JT, Kavoussi LR, Jarrett TW. The “mini-perc” technique: A less invasive alternative to percutaneous nephrolithotomy. World J Urol. 1998;16:371–4. doi: 10.1007/s003450050083. [DOI] [PubMed] [Google Scholar]
- 6.Jackman SV, Hedican SP, Docimo SG, Peters CA. Miniaturized access for pediatric percutaneous nephrolithotomy. J Endourol. 1997;11(Suppl 1):S133. [Google Scholar]
- 7.Chan DY, Jarrett TW. Mini-percutaneous nephrolithotomy. J Endourol. 2000;14:269–73. doi: 10.1089/end.2000.14.269. [DOI] [PubMed] [Google Scholar]
- 8.Maheshwari PN, Andankar MG, Bansal M. Nephrostomy tube after percutaneous nephrolithotomy: Larger bore or pigtail catheter? J Endourol. 2000;14:735–7. doi: 10.1089/end.2000.14.735. [DOI] [PubMed] [Google Scholar]
- 9.Ni S, Qiyin C, Tao W, Liu L, Jiang H, Hu H, et al. Tubeless percutaneous nephrolithotomy is associated with less pain and shorter hospitalization compared with standard or small bore drainage: A meta-analysis of randomized, controlled trials. Urology. 2011;77:1293–8. doi: 10.1016/j.urology.2010.10.023. [DOI] [PubMed] [Google Scholar]
- 10.Wickham JE, Miller RA, Kellett MJ, Payne SR. Percutaneous nephrostolithotomy: One stage or two? Br J Urol. 1984;56:582–5. doi: 10.1111/j.1464-410x.1984.tb06121.x. [DOI] [PubMed] [Google Scholar]
- 11.Winfield HN, Weyman P, Clayman RV. Percutaneous nephrostolithotomy: Complications of premature nephrostomy tube removal. J Urol. 1986;136:77–9. doi: 10.1016/s0022-5347(17)44733-1. [DOI] [PubMed] [Google Scholar]
- 12.Bellman GC, Davidoff R, Candela J, Gerspach J, Kurtz S, Stout L. Tubeless percutaneous renal surgery. J Urol. 1997;157:1578–82. [PubMed] [Google Scholar]
- 13.Delnay KM, Wake RW. Safety and efficacy of tubeless percutaneous nephrolithotomy. World J Urol. 1998;16:375–7. doi: 10.1007/s003450050084. [DOI] [PubMed] [Google Scholar]
- 14.Limb J, Bellman GC. Tubeless percutaneous renal surgery: Review of first 112 patients. Urology. 2002;59:527–30. doi: 10.1016/s0090-4295(01)01627-2. [DOI] [PubMed] [Google Scholar]
- 15.Gupta NP, Kesarwani P, Goel R, Aron M. Tubeless percutaneous nephrolithotomy. A comparative study with standard percutaneous nephrolithotomy. Urol Int. 2005;74:58–61. doi: 10.1159/000082711. [DOI] [PubMed] [Google Scholar]
- 16.Singh I, Singh A, Mittal G. Tubeless percutaneous nephrolithotomy: Is it really less morbid? J Endourol. 2008;22:427–33. doi: 10.1089/end.2007.0269. [DOI] [PubMed] [Google Scholar]
- 17.Shah HN, Mahajan AP, Hegde SS, Bansal M. Tubeless percutaneous nephrolithotomy in patients with previous ipsilateral open renal surgery: A feasibility study with review of literature. J Endourol. 2008;22:19–24. doi: 10.1089/end.2006.0480. [DOI] [PubMed] [Google Scholar]
- 18.Agrawal MS, Agrawal M, Gupta A, Bansal S, Yadav A, Goyal J. A randomized comparison of tubeless and standard percutaneous nephrolithotomy. J Endourol. 2008;22:439–42. doi: 10.1089/end.2007.0118. [DOI] [PubMed] [Google Scholar]
- 19.Shah HN, Kausik VB, Hegde SS, Shah JN, Bansal MB. Tubeless percutaneous nephrolithotomy: A prospective feasibility study and review of previous reports. BJU Int. 2005;96:879–83. doi: 10.1111/j.1464-410X.2005.05730.x. [DOI] [PubMed] [Google Scholar]
- 20.Malcolm JB, Derweesh IH, Brightbill EK, Mehrazin R, Diblasio CJ, Wake RW. Tubeless percutaneous nephrolithotomy for complex renal stone disease: Single center experience. Can J Urol. 2008;15:4072–6. [PubMed] [Google Scholar]
- 21.Falahatkar S, Khosropanah I, Roshani A, Neiroomand H, Nikpour S, Nadjafi-Semnani M, et al. Tubeless percutaneous nephrolithotomy for staghorn stones. J Endourol. 2008;22:1447–52. doi: 10.1089/end.2007.0285. [DOI] [PubMed] [Google Scholar]
- 22.Sofer M, Beri A, Friedman A, Aviram G, Mabjeesh NJ, Chen J, et al. Extending the application of tubeless percutaneous nephrolithotomy. Urology. 2007;70:412–7. doi: 10.1016/j.urology.2007.03.082. [DOI] [PubMed] [Google Scholar]
- 23.Rana AM, Mithani S. Tubeless percutaneous nephrolithotomy: Call of the day. J Endourol. 2007;21:169–72. doi: 10.1089/end.2006.0192. [DOI] [PubMed] [Google Scholar]
- 24.Feng MI, Tamaddon K, Mikhail A, Kaptein JS, Bellman GC. Prospective randomized study of various techniques of percutaneous nephrolithotomy. Urology. 2001;58:345–50. doi: 10.1016/s0090-4295(01)01225-0. [DOI] [PubMed] [Google Scholar]
- 25.Shah HN, Sodha HS, Khandkar AA, Kharodawala S, Hegde SS, Bansal MB. A randomized trial evaluating type of nephrostomy drainage after percutaneous nephrolithotomy: Small bore v tubeless. J Endourol. 2008;22:1433–9. doi: 10.1089/end.2007.0350. [DOI] [PubMed] [Google Scholar]
- 26.Desai MR, Kukreja RA, Desai MM, Mhaskar SS, Wani KA, Patel SH, et al. A prospective randomized comparison of type of nephrostomy drainage following percutaneous nephrostolithotomy: Large bore versus small bore versus tubeless. J Urol. 2004;172:565–7. doi: 10.1097/01.ju.0000130752.97414.c8. [DOI] [PubMed] [Google Scholar]
- 27.Shen P, Liu Y, Wang J. Nephrostomy tube-free versus nephrostomy tube for renal drainage after percutaneous nephrolithotomy: A systematic review and meta-analysis. Urol Int. 2012;88:298–306. doi: 10.1159/000332151. [DOI] [PubMed] [Google Scholar]
- 28.Lojanapiwat B, Soonthornphan S, Wudhikarn S. Tubeless percutaneous nephrolithotomy in selected patients. J Endourol. 2001;15:711–3. doi: 10.1089/08927790152596299. [DOI] [PubMed] [Google Scholar]
- 29.Mouracade P, Spie R, Lang H, Jacqmin D, Saussine C. Tubeless percutaneous nephrolithotomy: What about replacing the double-j stent with a ureteral catheter? J Endourol. 2008;22:273–5. doi: 10.1089/end.2007.0162. [DOI] [PubMed] [Google Scholar]
- 30.Karami H, Jabbari M, Arbab AH. Tubeless percutaneous nephrolithotomy: 5 Years of experience in 201 patients. J Endourol. 2007;21:1411–3. doi: 10.1089/end.2007.0406. [DOI] [PubMed] [Google Scholar]
- 31.Yew J, Bellman GC. Modified “tubeless” percutaneous nephrolithotomy using a tail stent. Urology. 2003;62:346–9. doi: 10.1016/s0090-4295(03)00461-8. [DOI] [PubMed] [Google Scholar]
- 32.Choi M, Brusky J, Weaver J, Amantia M, Bellman GC. Randomized trial comparing modified tubeless percutaneous nephrolithotomy with tailed stent with percutaneous nephrostomy with smallbore tube. J Endourol. 2006;20:766–70. doi: 10.1089/end.2006.20.766. [DOI] [PubMed] [Google Scholar]
- 33.Shpall AI, Parekh AR, Bellman GC. Tubeless percutaneous nephrolithotomy with antegrade stent tether: Clinical experience. J Endourol. 2007;21:973–6. doi: 10.1089/end.2006.9924. [DOI] [PubMed] [Google Scholar]
- 34.Bdesha AS, Jones CR, North EA, Pinfield J, Boyd PJ. Routine placement of a nephrostomy tube is not necessary after percutaneous nephrostolithotomy. Br J Urol. 1997;79(Suppl 4):1. [Google Scholar]
- 35.Karami H, Gholamrezaie HR. Totally tubeless nephrolithotomy in selected patients. J Endourol. 2004;18:475–6. doi: 10.1089/0892779041271580. [DOI] [PubMed] [Google Scholar]
- 36.Aghamir SM, Hosseini SR, Gooran S. Totally tubeless percutaneous nephrolithotomy. J Endourol. 2004;18:647–8. doi: 10.1089/end.2004.18.647. [DOI] [PubMed] [Google Scholar]
- 37.Gupta V, Sadasukhi TK, Sharma KK, Yadav RG, Mathur R. Tubeless and stentless percutaneous nephrolithotomy. BJU Int. 2005;95:905–6. doi: 10.1111/j.1464-410X.2005.05432.x. [DOI] [PubMed] [Google Scholar]
- 38.Crook TJ, Lockyer CR, Keoghane SR, Walmsley BH. Totally tubeless percutaneous nephrolithotomy. J Endourol. 2008;22:267–71. doi: 10.1089/end.2006.0034. [DOI] [PubMed] [Google Scholar]
- 39.Mandhani A, Goyal R, Vijjan V, Dubey D, Kapoor R. Tubeless percutaneous nephrolithotomy-should a stent be an integral part? J Urol. 2007;178:921–4. doi: 10.1016/j.juro.2007.05.021. [DOI] [PubMed] [Google Scholar]
- 40.Mishra S, Sabnis RB, Kurien A, Ganpule A, Muthu V, Desai M. Questioning the wisdom of tubeless percutaneous nephrolithotomy (PCNL): A prospective randomized controlled study of early tube removal vs tubeless PCNL. BJU Int. 2010;106:1045–8. doi: 10.1111/j.1464-410X.2010.09223.x. [DOI] [PubMed] [Google Scholar]
- 41.El-Nahas AR, Shokeir AA. Percutaneous nephrolithotomy: Keeping the bridge for one night. Urol Res. 2012;40:389–93. doi: 10.1007/s00240-011-0432-4. [DOI] [PubMed] [Google Scholar]
- 42.Lee DI, Uribe CA, Eichel L, Khonsari S, Basillote J, Park HK, et al. Sealing percutaneous nephrolithotomy tracts with gelatin matrix hemostatic sealant: Initial clinical use. J Urol. 2004;171:575–8. doi: 10.1097/01.ju.0000103501.98597.b7. [DOI] [PubMed] [Google Scholar]
- 43.Borin JF, Sala LG, Eichel L, Mcdougall EM, Clayman RV. Tubeless percutaneous nephrolithotomy using hemostatic gelatin matrix. J Endourol. 2005;19:614–7. doi: 10.1089/end.2005.19.614. [DOI] [PubMed] [Google Scholar]
- 44.Uribe CA, Eichel L, Khonsari S, Finley DS, Basillote J, Park HK, et al. What happens to hemostatic agents in contact with urine. An in vitro study? J Endourol. 2005;19:312–7. doi: 10.1089/end.2005.19.312. [DOI] [PubMed] [Google Scholar]
- 45.Nagele U, Schilling D, Anastasiadis AG, Corvin S, Seibold J, Kuczyk M, et al. Closing the tract of mini-percutaneous nephrolithotomy with gelatine matrix hemostatic sealant can replace nephrostomy tube placement. Urology. 2006;68:489–94. doi: 10.1016/j.urology.2006.03.081. [DOI] [PubMed] [Google Scholar]
- 46.Schilling D, Winter B, Merseburger AS, Anastasiadis AG, Walcher U, Stenzl A, et al. Use of a gelatine-thrombin matrix for closure of the access tract without a nephrostomy tube in minimally invasive percutaneous nephrolitholapaxy. Urologe A. 2008;47:601–7. doi: 10.1007/s00120-008-1673-x. [DOI] [PubMed] [Google Scholar]
- 47.Mikhail AA, Kaptein JS, Bellman GC. Use of fibrin glue in percutaneous nephrolithotomy. Urology. 2003;61:910–4. doi: 10.1016/s0090-4295(03)00112-2. [DOI] [PubMed] [Google Scholar]
- 48.Noller M, Baughman S, Morey A, Auge B. Fibrin sealant enables tubeless percutaneous stone surgery. J Urol. 2004;172:166–9. doi: 10.1097/01.ju.0000129211.71193.28. [DOI] [PubMed] [Google Scholar]
- 49.Shah HN, Kausik V, Hedge S, Shah JN, Bansal MB. Initial experience with hemostatic fibrin glue as adjuvant during tubeless percutaneous nephrolithotomy. J Endourol. 2006;20:194–8. doi: 10.1089/end.2006.20.194. [DOI] [PubMed] [Google Scholar]
- 50.Shah HN, Hegde S, Shah JN, Mohile PD, Yuvaraja TB, Bansal MB. A prospective, randomized trial evaluating the safety and efficacy of fibrin sealant in tubeless percutaneous nephrolithotomy. J Urol. 2006;176:2488–93. doi: 10.1016/j.juro.2006.07.148. [DOI] [PubMed] [Google Scholar]
- 51.Aghamir SM, Khazaeli MH, Meisami A. Use of surgicel for sealing nephrostomy tract after totally tubeless percutaneous nephrolithotomy. J Endourol. 2006;20:293–5. doi: 10.1089/end.2006.20.293. [DOI] [PubMed] [Google Scholar]
- 52.Singh I, Saran RN, Jain M. Does sealing of the tract with absorbable gelatin (spongostan®) facilitate tubeless PCNL. A prospective study? J Endourol. 2008;22:2485–94. doi: 10.1089/end.2008.0321. [DOI] [PubMed] [Google Scholar]
- 53.Jou YC, Cheng MC, Sheen JH, Lin CT, Chen PC. Cauterization of access tract for nephrostomy tube-free percutaneous nephrolithotomy. J Endourol. 2004;18:547–9. doi: 10.1089/end.2004.18.547. [DOI] [PubMed] [Google Scholar]
- 54.Aron M, Goel R, Kesarwani PK, Gupta NP. Hemostasis in tubeless PNL: Point of technique. Urol Int. 2004;73:244–7. doi: 10.1159/000080835. [DOI] [PubMed] [Google Scholar]
- 55.Yang RM, Bellman GC. Tubeless percutaneous renal surgery in obese patients. Urology. 2004;63:1036–41. doi: 10.1016/j.urology.2004.01.051. [DOI] [PubMed] [Google Scholar]
- 56.Kara C, Resorlu B, Bayindir M, Unsal A. A randomized comparison of totally tubeless and standard percutaneous nephrolithotomy in elderly patients. Urology. 2010;76:289–93. doi: 10.1016/j.urology.2009.11.077. [DOI] [PubMed] [Google Scholar]
- 57.Gudeman SR, Stroup SP, Durbin JM, Patino G, L’esperance JO, Auge BK. Percutaneous stone surgery using a tubeless technique with fibrin sealant: Report of our first 107 cases. BJU Int. 2012;110(11Pt C):E1048–52. doi: 10.1111/j.1464-410X.2012.11209.x. [DOI] [PubMed] [Google Scholar]