

Abstract
Background:
In middle age people, hypercholesterolemia (HC) has been included as a risk factor for cardiovascular disease.
Objectives:
The main objective of this study was to evaluate the prevalence of HC and some related factors in the north of Iran.
Materials and Methods:
This was a population-based cross-sectional study that enrolled 1995 subjects (997 males and 998 females) in 25-65 year age using stratified cluster sampling. Interviewers recorded the data using a multidimensional questionnaire including anthropometric indexes. Plasma cholesterol was measured in the morning after a 12-hour fast and determined by an auto-analyzer. HC was defined by a total plasma total cholesterol level over 200 mg/dl. The SPSS.16 software was used to analyze data.
Results:
The mean age of the participant was 44.2 years and mean ± SD plasma total cholesterol level in men and women was 196.7 ± 39.11 and 209.4 ± 42.9, respectively. Generally, the prevalence of HC was 50.4% with a significant differences between men (44.7%) and women (57%) (P < 0.05). The mean plasma total cholesterol levels were significantly differenced among age groups, location area, BMI, and waist circumferences (P < 0.001). Women gender (OR = 1.64), 55-65 years old (OR = 2.79), BMI ≥40 kg/m2 (OR = 10.0), and abdominal obesity (OR = 2.47) were associated with increased risk of HC (P = 0.001 and 95%CI for all).
Conclusion:
HC is one of the most health problems in the northern Iran and it is more common in women than in men. General and abdominal obesity are the most common risk factors for HC.
Keywords: Hypercholesterolemia, Iran, obesity, socio-demographic, total cholesterol
INTRODUCTION
In middle age people, total cholesterol levels have been established as a risk factor for a cardiovascular disease (CVD) risk marker.[1] In Finland data have been shown that mortality rate from CVD among people high plasma total cholesterol level people (>300 mg/dl) is fivefold higher than other factors and reducing plasma total cholesterol level by 10% can reduce the mortality due to CVD up 30%.[2]
According to a survey in the USA, 50% of adults showed cholesterol level higher than 200 mg/dl, while 37 million people had levels higher than 240 mg/dl.[3] Framingham et al.[4] showed that the prevalence of mortality and morbidity due to CVD can be estimated by the determination of plasma cholesterol levels in young and adult people. Several other studies have shown that many factors such as lifestyle, diet, smoking, BMI, gender, physical activity, and age are correlated with mean plasma cholesterol level.[5,6,7]
Of 1.6 million people in Golestan province (northern Iran and south east of Caspian sea), 66.39% are 25-65 years old, whereas 43.9% and 56.1% are living in urban and rural area, respectively.[8] Agriculture is the main occupation in the rural area.
The main objective of this study was to determine the plasma total cholesterol status and some associated factors in people of urban and rural areas in northern Iran. This study may suggest the ways to decline or prevent the risk of CVD in this area.
MATERIALS AND METHODS
This was a population-based cross-sectional study conducted in Golastan Province (northern Iran). Regarding the previous study[3] and 95% confidence interval, 1995 subjects (997 males and 998 females) were chosen by the stratified cluster sampling method. From 11 districts, 100 clusters of 20 cases were randomly selected by family code in Primary Health Centers in rural areas and postal code in urban areas with equal proportions of genders. From each district, one team was trained to complete the questionnaire and measure anthropometric indexes. The questionnaire included demographic characteristics, residential area, educational level, and physical activity.
All family members in blocks who were in 25-65 years were included in the clusters. Pregnant women and those who were unwilling to participate in this study were excluded from the study. Weight was measured with light clothing without shoes and height was measured with standing up and head, back, and buttock on the vertical land of the height gauge.
Body mass index (BMI) was calculated as weight (kg)/height (m2) and using World Health Organization classification.[9] BMI of 25.0-29.9 kg/m2 was classified as overweight, BMI of 30.0-39.9 kg/m2 was classified as obese, and BMI ≥40 kg/m2 was classified as pathologic obese. Waist circumference higher than the normal range (men >102 and women >88 cm) was determined as abdominal obesity.[10]
Physical activity was categorized into five categories based on daily work and activity including no physical activities (without moving from one place to another), low physical activity (activity that requires extension of the muscular–skeletal system and moving from one place to another), moderate physical activity (activity that requires sometimes increased respiratory rate like cleanliness, gardening, building painting, etc.), high physical activity (activity that requires highly increased reparatory rate like manual labor, building labor, etc.), and very high activity (a combination of above activities).[11]
For measuring plasma total cholesterol level, blood was drowned from each subject after 12 hours fast in the morning. Plasma total cholesterol was measured with commercial kits (Pars Azmoon, Karaj, Iran) by an auto-analyzer. The plasma cholesterol level more than 200 mg/dl was diagnosed as hypercholesterolemia (HC).[12]
SPSS 16.0 software was used for the statistical analysis, the Chi-square test was used for comparing frequencies and the t-test and ANOVA were used for comparing the means. Logistic regression analysis was applied in order to estimate the odds ratio (OR) of HC considering the socio-demographic factors at 95% significant level. A P value <0.05 included significations. The reliability was assessed using Cronbach's alpha coefficient and was found to be 0.86. This study was approved by Ethical Research Committee and consent was received from all participants. Unwilling subjects and pregnant women were excluded from this study.
RESULTS
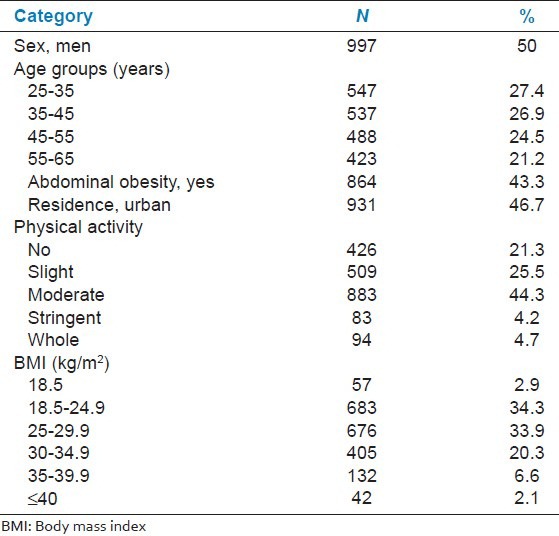
The mean and standard deviation of age was 44.2 ± 11.3 years. Of the 1995 subjects, 50%, 46.7%, 29%, and 43.3% were men, urban residence, general, and abdominal obese, respectively [Table 1].
Table 1.
Characteristics of study subjects (n=1995)
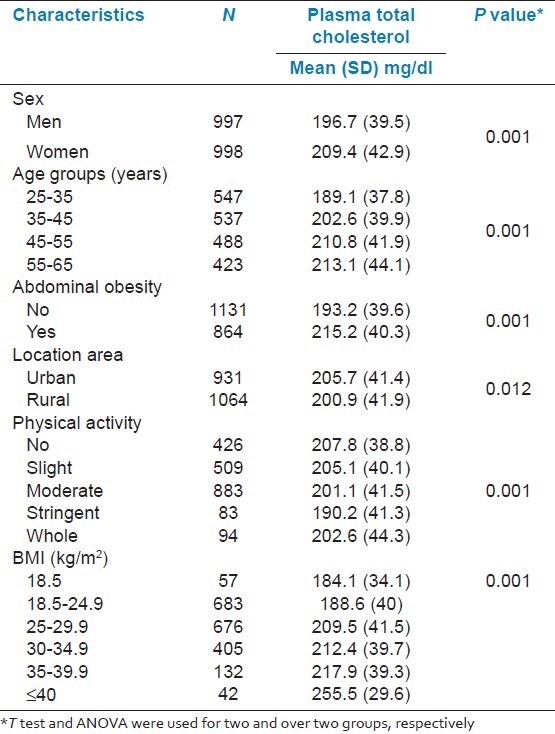
The mean and standard deviation of plasma total cholesterol levels were 203.6 ± 40.7 mg/dl and it was 12.7 mg/dl higher in women than in men. There was a positive significant correlation between age and plasma total cholesterol level (P = 0.001). Plasma total cholesterol level decreased with physical activity; the mean of plasma total cholesterol level in the low active group (205.1 mg/dl) was 14.9 mg/dl higher than in the very active group (190.2 mg/dl) which was statistically significant (P = 0.019). The plasma total cholesterol level had a positive correlation with BMI P = 0.001), and in the obese group (BMI ≤40 kg/m2) (255.5 mg/dl) it was 71.4 mg/dl higher than in the thin group (BMI <18.5 kg/m2) (184.1 mg/dl) [Table 2].
Table 2.
The mean and standard deviation of plasma total cholesterol levels based on some related factors
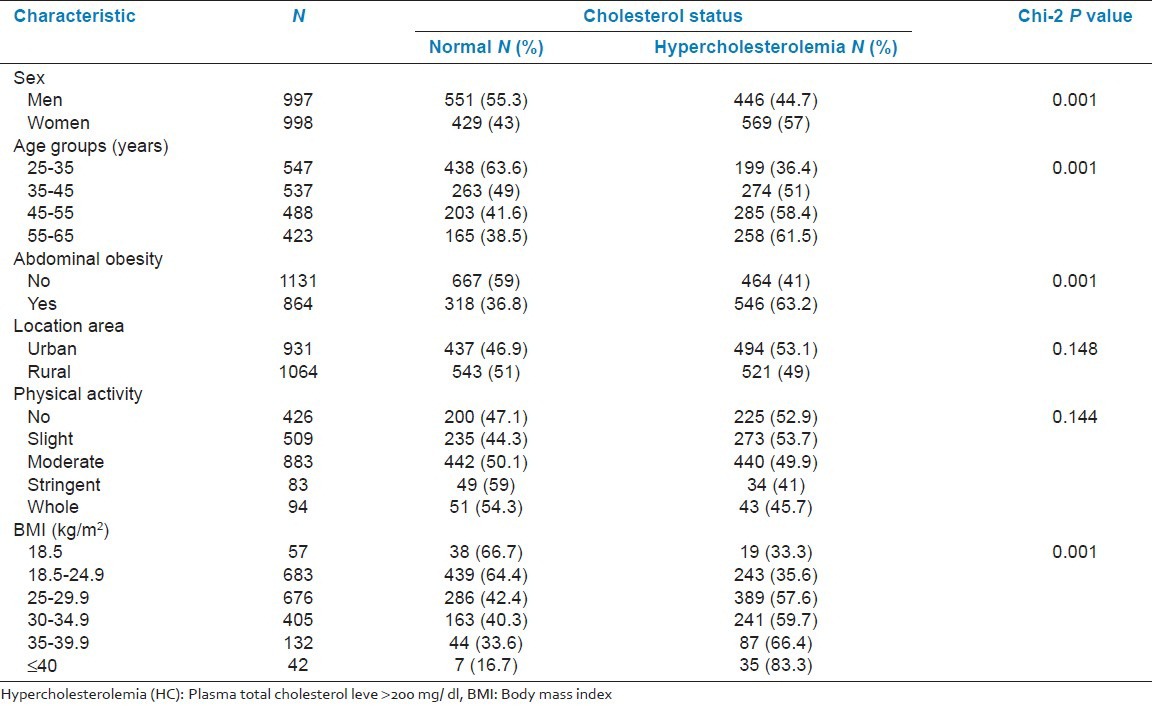
The overall prevalence of HC was 50.9% and it was up to 12.3% higher in women (57%) than in men (44.7%) (P = 0.001). The prevalence of HC was 25.1% among 55-65 years age participants (61.5%) higher than among that observed in the 25-35 years age group (36.4%). HC was significantly common in abdominal obese subjects (63.2%) higher than in normal subjects (41%) (P = 0.001) and in the urban area (53.1%) it was 4.1% higher than in the rural area (49%) without statistically significant difference [Table 3].
Table 3.
The prevalence of hypercholesterolemia based on some related factors
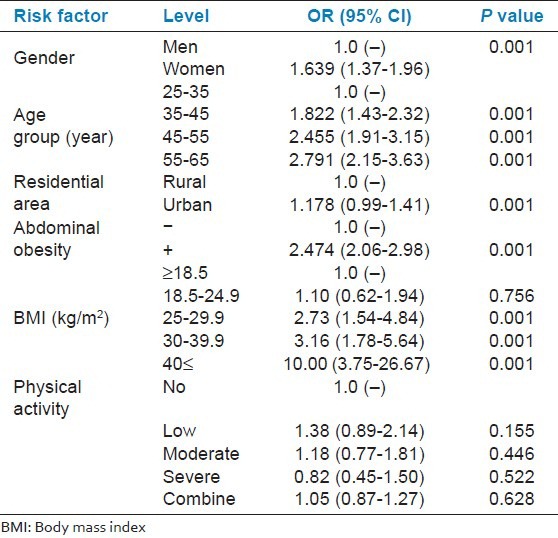
Multiple logistic regressions were used to identify variables that contribute to HC. The risk of HC was found to be 1.64 [95% CI: 1.31-1.99] in female compared to male; 2.79 [95% CI: 2.15-3.631] in 55-65 years subjects compared to 25-35 years; 10.00 [95% CI: 3.75-26.67] in BMI ≥40 compared to BMI ≤18.5 and 2.47 [95% CI: 2.06-2.98] in abdominal obesity compare to normal people. No significant differences were found among residential area and physical activities [Table 4].
Table 4.
Odds ratio and 95% CI obtained from logistic regression analysis for hypercholesterolemia
DISCUSSION
The results of this study show that half of adult population living in northern Iran is hypercholestrolomic. The prevalence of HC has been reported to be in Romania (70%), Northwest Mexico (52.6%), Indian rural (22.3%), Spain (24%), Western Samoa (36%), Koki (25%), and Saudi Arabia (54%).[6,13,14,15,16,17,18] HC prevalence in Tehran (capital of Iran) and in Arak (a capital city in central Iran) has been reported up to be 40.4% and 26.7%, respectively.[19] As like as mentioned studies[13,14,18] the prevalence of HC in the north of Iran is high and should be consider as the most common health problem in this area.
In our study, the prevalence of HC was seen to be higher in urban than in rural and higher in women than in men. There was a positive association between age, waist circumference, and BMI with plasma total cholesterol level.
Increasing HC in an urban population in the worldwide has been shown in some studies.[18,20,21] Similarly, women suffer from HC than man.[13,21,22,23,24] After menopause, estrogen has a positive role in serum cholesterol level, therefore, estrogen therapy has been recommended for the control of CVD.[22] In our study, half of the women were over 45 years, which may be used as a interfering factor for increased plasma total cholesterol level.
The correlation between plasma total cholesterol level and age, waist circumference, and BMI in our study is similar to the earlier reports.[13,23,25,26,27,28]
The influence of physical activity on the serum cholesterol level was not similar in all studies. Although the role of physical activity in decreasing plasma total cholesterol level has been shown in many studies,[29,30] there was not any correlation between them in another.[31] Physical activities decreased the plasma lipid profile with statistical significant differences in HDLc and ApoA1.[4,24]
We don’t know whether there is any signification between physical activity and HC, but it seems that other related factors which are not included in our study such as ethnicity and food behavior do have influence on the plasma total cholesterol level.
CONCLUSION
Our study showed that HC is a health problem in northern Iran and it is common in half the adult population. Socio-economic status, general, and abdominal obesity are predispose factors for HC. Screening and intervention programs for the prevention of HC are necessary. Further studies are necessary to examine the related factors such as life style, food behavior, ethnic differences, and awareness with HC.
ACKNOWLEDGMENTS
The authors would like to thank the medical and administrative staff in the Primary Health Care Centers of Golestan University of Medical Sciences for their valuable assistance during the field work. This paper was created from provincial incommunicable data study and supported by Health Office of Golestan University of Medical Sciences and based on 258888 official document justifying publication.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Kones R. Primary prevention of coronary heart disease: Integration of new data, evolving views, revised goals, and role of rosuvastatin in management. A comprehensive survey. Drug Des Devel Ther. 2011;5:325–80. doi: 10.2147/DDDT.S14934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ousilahti P. Serum cholesterol disease risk: Observations and predictions among middle aged population in eastern Finland. Circulation. 1998;97:1087–97. doi: 10.1161/01.cir.97.11.1087. [DOI] [PubMed] [Google Scholar]
- 3.Schaefer EJ. Hyperlipidemia and coronary artery disease. In: Becker KL, editor. Becker's principles and practice of endocrinology and metabolism. 2nd ed. Philadelphia: J B Lippincott Company; 1995. pp. 1378–80. [Google Scholar]
- 4.D’Agostino RB, Sr, Grundy S, Sullivan LM, Wilson P CHD Risk Prediction Group. Validation of the Framingham coronary heart disease prediction scores: Results of a multiple ethnic groups investigation. JAMA. 2001;286:180–7. doi: 10.1001/jama.286.2.180. [DOI] [PubMed] [Google Scholar]
- 5.Morikawa Y, Nakagawa H, Miura K, Soyama Y, Ishizaki M, Kido T, et al. Effect of shift work on body mass index and metabolic parameters. Scand J Work Environ Health. 2007;33:45–50. doi: 10.5271/sjweh.1063. [DOI] [PubMed] [Google Scholar]
- 6.Oancă ME, Azoicăi D, Manole A, Ivan A. Contributions to the knowledge of clinical and epidemiological features of essential arterial hypertension in Moldavia, Romania. Rev Med Chir Soc Med Nat Iasi. 2007;111:1012–6. [PubMed] [Google Scholar]
- 7.Kolovou GD, Anagnostopoulou KK, Damaskos DS, Mihas C, Mavrogeni S, Hatzigeorgiou G, et al. Gender influence on postprandial lipemia in heterozygotes for familial hypercholesterolemia. Ann Clin Lab Sci. 2007;37:335–42. [PubMed] [Google Scholar]
- 8.Statistical Center of Iran. Population and Housing Census. 2006. [Last accessed on 2011 May 23]. Available from: http://www.sci.org.ir .
- 9.Geneva: WHO; 2000. World Health Organization. Obesity: Prevention and managing the global epidemic. [Google Scholar]
- 10.Molarius A, Seidell JC, Visscher TL, Hofman A. Misclassification of high-risk older subjects using waist action levels established for young and middle-aged adults-results from the Rotterdam Study. J Am Geriatr Soc. 2000;48:1638–45. doi: 10.1111/j.1532-5415.2000.tb03876.x. [DOI] [PubMed] [Google Scholar]
- 11.Ebrahimi M, Mansournia MA, Haghdoost AA, Abazari A, Alaeddini F, Mirzazadeh A, et al. Social disparities in prevalence, treatment and control of hypertension in Iran: Second national surveillance of risk factors of noncommunicable diseases 2006. J Hypertens. 2010;28:1620–9. doi: 10.1097/HJH.0b013e32833a38f2. [DOI] [PubMed] [Google Scholar]
- 12.Costa J, Borges M, Oliveira E, Gouveia M, Carneiro AV. Incidence and prevalence of hypercholesterolemia in Portugal: A systematic review. Part 3. Rev Port Cardiol. 2003;22:829–36. [PubMed] [Google Scholar]
- 13.Alemán-Mateo H, Esparza-Romero J, Romero RU, García HA, Pérez Flores FA, Ochoa Chacón BV, et al. Prevalence of malnutrition and associated metabolic risk factors for cardiovascular disease in older adults from Northwest Mexico. Arch Gerontol Geriatr. 2008;46:375–85. doi: 10.1016/j.archger.2007.05.010. [DOI] [PubMed] [Google Scholar]
- 14.Gupta R. Lipoprotein tipids and the prevalence of hyperlipidemia in rural India. J Cardiovasc Risk. 1994;1:179–84. doi: 10.1177/174182679400100213. [DOI] [PubMed] [Google Scholar]
- 15.Plans P, Pardell H, Salleras L. Epidemiology of cardiovascular disease risk factors in Catalonia (Spain) Eur J Epidemiol. 1993;9:381–9. doi: 10.1007/BF00157394. [DOI] [PubMed] [Google Scholar]
- 16.Hodge AM, Dowse GK, Tocluope P. The association of modernization with dyslipidemia and changes in lipid levels in the Polynesian population of western Samoa. Int J Epidemol. 1997;26:297–306. doi: 10.1093/ije/26.2.297. [DOI] [PubMed] [Google Scholar]
- 17.Erasmus RT, Sinh AK, Nathniel K. Serum lipid concentrations in the Koki community a preliminary report. Med J. 1993;36:306–10. [PubMed] [Google Scholar]
- 18.Al-Nozha MM, Arafah MR, Al-Maatouq MA, Khalil MZ, Khan NB, Al-Marzouki K, et al. Hyperlipidemia in Saudi Arabia. Saudi Med J. 2008;29:282–7. [PubMed] [Google Scholar]
- 19.Agheli N, Movahedi A. Serum Cholesterol level and its association with their fats and Cholesterol intake. J Med Fac Guilan Univ Med Sci. 2001;38-37:77–69. [Google Scholar]
- 20.Janghorbani M, Amini M, Gouya MM, Delavari A, Alikhani S, Mahdavi A. Nationwide survey of prevalence and risk factors of prehypertension and hypertension in Iranian adults. J Hypertens. 2008;26:419–26. doi: 10.1097/HJH.0b013e3282f2d34d. [DOI] [PubMed] [Google Scholar]
- 21.al-Nuaim AR, Mirdad S, al-Rubeaan K, al-Mazrou Y, al-Attas O, al-Daghari N, et al. Population-based epidemiological study on characteristics of risk factors of hypercholesterolemia in Saudi Arabia. Int J Cardiol. 1997;31(62):47–54. doi: 10.1016/s0167-5273(97)00164-2. [DOI] [PubMed] [Google Scholar]
- 22.Gast GC, Grobbee DE, Pop VJ, Keyzer JJ, Wijnands-van Gent CJ, Samsioe GN, et al. Menopausal complaints are associated with cardiovascular risk factors. Hypertension. 2008;51:1492–8. doi: 10.1161/HYPERTENSIONAHA.107.106526. [DOI] [PubMed] [Google Scholar]
- 23.Karimi F, Rayani M, Akbarzadeh S, Khakzad M, Tahmasebi R, Arab J, et al. Prevalence of hy1perlipidemias in adult population (=>19 years) of Bushehr port, 1999. Iranian South Med J. 2001;2:106–98. [Google Scholar]
- 24.Panagiotakos DB, Pitsavos C, Chrysohoou C, Skoumas J, Zeimbekis A, Papaioannou I, et al. Effect of leisure time physical activity on blood lipid levels: The ATTICA study. Coron Artery Dis. 2003;14:533–9. doi: 10.1097/00019501-200312000-00003. [DOI] [PubMed] [Google Scholar]
- 25.Kende M. Superiority of traditional village diet and lifestyle in minimizing cardiovascular disease risk in Papua New Guineans. P N G Med J. 2001;44:135–50. [PubMed] [Google Scholar]
- 26.Oppert JM, Thomas F, Charles MA, Benetos A, Basdevant A, Simon C. Leisure-time and occupational physical activity in relation to cardiovascular risk factors and eating habits in French adults. Public Health Nutr. 2006;9:746–54. doi: 10.1079/phn2005882. [DOI] [PubMed] [Google Scholar]
- 27.Ko GT, Chan JC, Chan AW, Wong PT, Hui SS, Tong SD, et al. Low levels of awareness of suboptimal health conditions in a high-risk working population: The “better health for better Hong Kong” health promotion campaign. Int J Behav Med. 2007;14:63–9. doi: 10.1007/BF03004170. [DOI] [PubMed] [Google Scholar]
- 28.Williams PT, Hoffman K, La I. Weight-related increases in hypertension, hypercholesterolemia, and diabetes risk in normal weight male and female runners. Arterioscler Thromb Vasc Biol. 2007;27:1811–9. doi: 10.1161/ATVBAHA.107.141853. [DOI] [PubMed] [Google Scholar]
- 29.Remsberg KE, Rogers NL, Demerath EW, Czerwinski SA, Choh AC, Lee M, et al. Sex differences in young adulthood metabolic syndrome and physical activity: The Fels longitudinal study. Am J Hum Biol. 2007;19:544–50. doi: 10.1002/ajhb.20615. [DOI] [PubMed] [Google Scholar]
- 30.Chen JL, Wu Y. Cardiovascular risk factors in Chinese American children: Associations between overweight, acculturation, and physical activity. J Pediatr Health Care. 2008;22:103–10. doi: 10.1016/j.pedhc.2007.03.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Perkins GM, Owen A, Kearney EM, Swaine IL. Biomarkers of cardiovascular disease risk in 40-65-year-old men performing recommended levels of physical activity, compared with sedentary men. Br J Sports Med. 2009;43:136–41. doi: 10.1136/bjsm.2007.044420. [DOI] [PubMed] [Google Scholar]