

Abstract
Objective:
To measure the arch width and Median mandibular flexure (MMF) values at relative rest and maximum jaw opening in young adults with Dolichofacial, Mesofacial, and Brachyfacial types and tested whether the variation in the facial pattern is related to the MMF values in South Indian population.
Materials and Methods:
This Prospective clinical study consisted of sample of 60 young adults. The subjects were grouped into 3 groups: Group 1: Brachyfacial, Group 2: Mesofacial and types, Group 3: Dolichofacial. Impressions were taken for all the 60 subjects and the casts were scanned and digitized. The intermolar width was measured for Dolichofacial, Mesofacial, and Brachyfacial subjects at relative rest (R) and maximum opening (O).
Results:
The statistical analysis of the observations included Descriptive and Inferential statistics. The statistical analysis was executed by means of Sigma graph pad prism software, USA Version-4. Kruskal wallis (ANOVA) followed by Dunns post hoc test was performed. Mann Whitney U-test was performed to assess the difference in MMF values between Males and Females of the three groups. The Mean (SD) Mandibular flexure in individuals with Brachyfacial type was 1.12 (0.09), Mesofacial type was 0.69 (0.21), and Dolichofacial type was 0.39 (0.08).
Conclusions:
The Mean intermolar width was maximum in Brachyfacial type and minimum in Dolichofacial type. MMF was maximum at the maximum mouth opening position and was maximum in individuals with Brachyfacial type.
Keywords: Brachyfacial, dolichofacial, median mandibular flexure, mesofacial
INTRODUCTION
Dental arch width and facial form are important factors for determining success and stability of orthodontic treatment. The size and shape of arches will have considerable implication in orthodontic diagnosis and treatment planning, affecting the space available, dental aesthetics, and stability of dentition. Arch form is the position and relationship of teeth to each other in all three dimensions.[1] Three basic types of facial morphology exists; short, average, and long. Those with long face have excessive vertical facial growth which is usually associated with an anterior open bite, increased sella-nasion mandibular plane angle, increased gonial angle, and increased maxillary/mandibular planes angle. The short face types have reduced vertical growth that is accompanied by a deep over bite, reduced facial heights, and reduced sella-nasion mandibular plane angle. Between the two types lies the average face.[2]
Median mandibular flexure (MMF) is the mandibular deformation characterized by decrease in the arch width during jaw opening and protrusive movements because of the functional contraction of the lateral pterygoid muscle causing high strain in the symphyseal region.[3] External pterygoids contract in an almost frontal plane during the opening and protrusion of the mandible pull the condyles together and this contraction causes flexure.[4] The influence of geometric facial factors on mandibular deformation is unclear as only a few measures have been found to be statistically significant. For example, some in vivo studies observed that the highest values of mandibular deformation occurred in subjects with lower symphysis height.[3,5] Also, Chen et al.[6] found that subjects with larger mandibular length, lower gonial angle, and smaller symphysis area had the highest mandibular deformation. Osbourne and Tomalin[7] in an in vivo study proved the changes in arch width during forced opening and protrusion and also demonstrated that the degree of flexure depends on the opening of the mouth. There is a lack of data from Indian populations on mandibular deformation in relation to vertical facial pattern.
The purpose of this study is to measure the arch width and MMF values at relative rest and maximum jaw opening in young adults with Dolichofacial, Mesofacial, and Brachyfacial types and tested whether the variation in the facial pattern is related to the MMF values in South Indian population.
MATERIALS AND METHODS
The Sample in this cross-sectional prospective study consisted of 60 individuals who visited the Department of orthodontics Narayana Dental College, Nellore. Inclusion criteria: Patient who were to begin orthodontic treatment for whom the radiographs are routinely taken. Male and Female subjects between 20 to 30 years of age. Exclusion criteria: Growth abnormality, Bleeding disorder, Patients on any long-term medication. The grouping of the sample was done on the basis of cephalometric measurements done using five mandibular measurements (mandibular plane, facial depth, anterior facial height, facial axis, and mandibular arch)[8] and were grouped into:
Group 1: With low mandibular plane angle with short vertical facial height and Horizontal growth pattern, Group 2: With average mandibular plane angle and average vertical facial height and Average growth pattern, Group 3: With high mandibular plane angle and long vertical facial height and Vertical growth pattern [Figure 1]. The kappa statistic was used to measure interexaminer and intraexaminer reliability at 0.794 and 0.824, respectively. There was no statistically significant difference between the examiners’ readings. Both examiners independently staged all tracings, and, if there was disagreement, they were recalibrated regarding the Group in conflict; then, the tracings were reviewed again and remeasured by both examiners until consensus was reached. For every subject, impressions of the incisal and occlusal thirds of the mandibular teeth were obtained using a polyvinyl siloxane putty material (3M Empress) [Figure 2]. The impressions were obtained in three positions of the mandible, during the relative rest position of the mandible, minimum opening of mouth and maximum opening [Figure 3]. The impressions were poured under vacuum with Ultra Rock Die stone with the electronically weighed water powder ratios. The casts obtained were scanned along with a scale to digitalize the image and scanning was done to avoid any errors due to magnification. Using Coral Draw software, anatomical reference points on the contralateral first molars were selected for the images. MMF was measured by calculating the variation of the intermolar distance from rest (R) to maximum opening (O) using impression technique.[9] Intermolar distance was measured [Figure 4] in triplicate for each image and then averaged.
Figure 1.
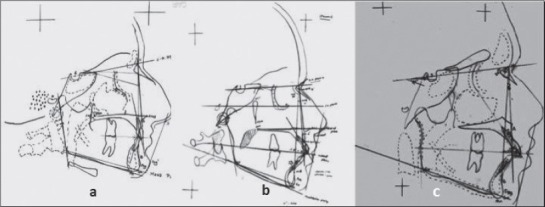
Brachyfacial, mesofacial and dolicofacial types
Figure 2.

3M empress Putty Material, Impressions in three positions of the mandible
Figure 3.
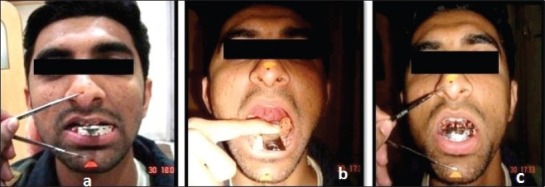
Relative rest position of the mandible, Minimum opening and Maximum opening of mouth
Figure 4.
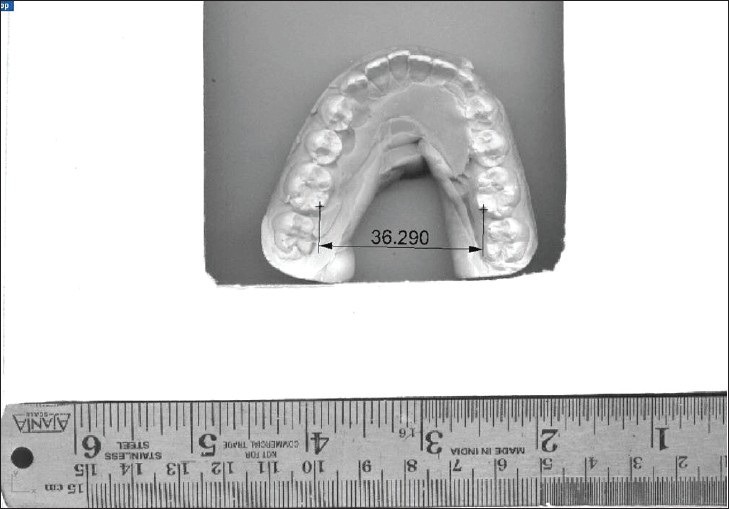
Measurement of inter molar width
RESULTS
The statistical analysis of the observations included Descriptive and Inferential statistics. The statistical analysis was executed by means of Sigma graph pad prism software, USA Version-4.
Continuous data were presented as mean, median, range, and standard deviation. Between group analyses were carried out by using Kruskal walls (ANOVA) followed by Dunns post hoc test. Mann Whitney U-test was performed to assess the difference in MMF values between Males and Females of the three groups.
Table 1 illustrates the intermolar distance recorded for the 3 groups: Group 1: Brachyfacial, Group 2: Mesofacial, Group 3: Dolichofacial at relative rest and maximum opening of the mouth and the difference between the values at maximum opening of mouth and rest position for each individual in all the groups.
Table 1.
Observations of median median mandibular flexure values of the 3 groups at rest and maximum mouth opening with the difference between the values
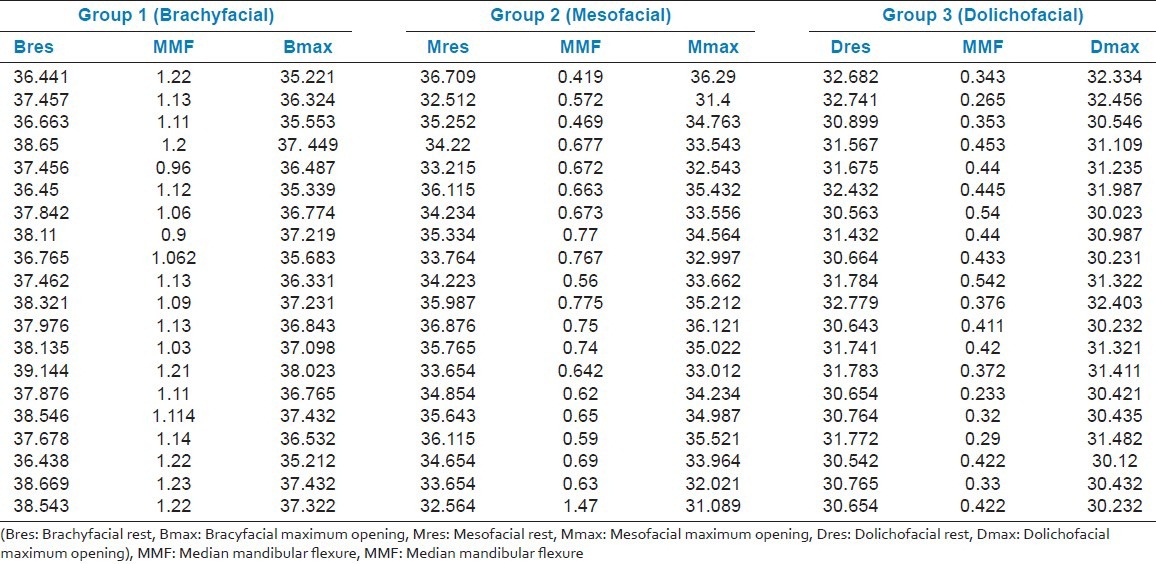
Table 2 illustrates the Mean (SD) intermolar distance for the Group 1 (Brachyfacial) that was 37.73 mm (0.83) at relative rest and 36.61 mm (0.84) at maximum opening with Mean MMF of 1.12 mm (0.09). The Mean intermolar distance for Group 2 (Mesofacial) was 34.77 mm (1.31) at relative rest and 33.92 mm (1.49) at maximum mouth opening with Mean MMF of 0.69 mm (0.21) and the Mean intermolar distance for Group 3 (Dolichofacial) was 31.4 mm (0.79) at relative rest and 31.04 mm (0.80) at maximum mouth opening with Mean MMF of 0.39 mm (0.08).
Table 2.
Descriptive statistics

Kruskal walls (ANOVA) followed by Dunns test was used to assess any significant difference in the between the three groups [Table 3].
Table 3.
Inferential statistics
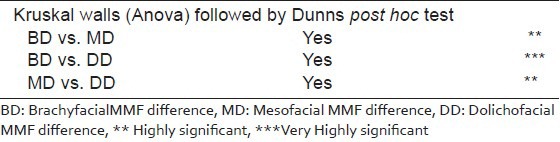
There is significant difference in the Mean MMF values between the three groups. There was no significant difference in the Mean MMF values between males and females in Group 1 and 2 but Group 3 shows significant difference in the MMF values [Table 4 and Figure 5].
Table 4.
Mann Whitney test (difference between Median mandibular flexure values of males and females in the 3 groups)
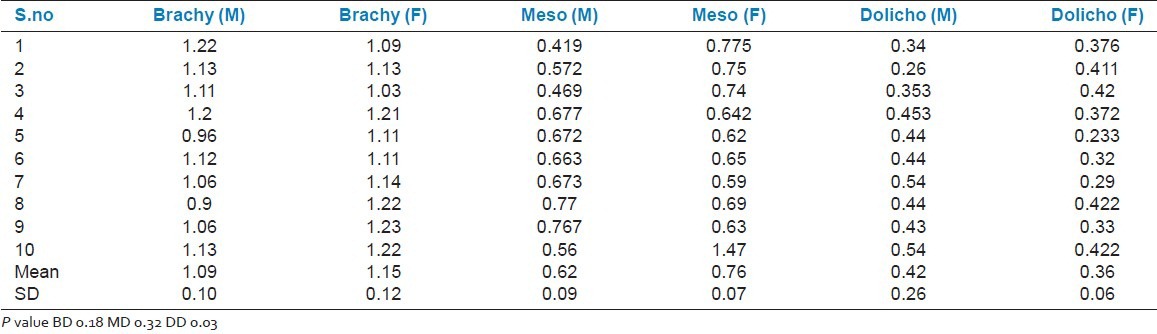
Figure 5.
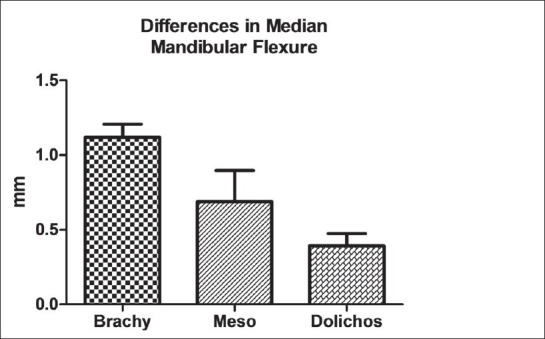
Difference between Mean MMF values of 3 Groups
DISCUSSION
The results of the study indicate that Mean (SD) intermolar distance for the Group 1 (Brachyfacial) was 37.73 mm (0.83) with Mean MMF of 1.12 mm (0.09). The Mean intermolar distance for Group 2 (Mesofacial) was 34.77 mm (1.31) with Mean MMF of 0.69 mm (0.21) and the Mean intermolar distance for Group 3 (Dolichofacial) was 31.4 mm (0.79) with Mean MMF of 0.39 mm (0.08). The Mean intermolar distance was maximum in the Brachyfacial type of individuals. The results in this study were similar to that of Nasby et al.[10] He demonstrated narrower intermolar widths in high-angle children.
The study suggests that MMF is maximum in Brachyfacial type and minimum in Dolichofacial type and maximum values of MMF are seen in Maximum opening of the jaw as compared to relative rest in all the 3 groups. Musculature can be considered as the possible link in this close relationship between the transverse dimension and vertical facial morphology. A number of studies[11,12,13] have illustrated the influence of masticatory muscles on craniofacial growth.
The general consensus[14] is that individuals with strong or thick mandibular elevator muscles tend to exhibit wider transverse head dimensions. Strong masticatory musculature is often associated with a brachyfacial pattern (short face). This muscular hyperfunction causes an increased mechanical loading of the jaws. This in turn may cause an introduction of sutural growth and bone apposition which then results in increased transverse growth of the jaws and bone bases for the dental arches.
Spronsen et al.[15] found that long-faced subjects have significantly smaller masseter and medial pterygoid muscles than normal subjects. Fikret Satirglu[13] et al. ultrasonographically measured masseter muscle thickness. They found that individuals with thick masseter had a vertically shorter facial pattern and individuals with thin masseter have a long face. Their results showed a significant association between vertical facial pattern and masseter muscle thickness. These results are in agreement with previous studies done by Weijis et al., Kiliardis and Kalebo, Benington et al., and Raadsheer et al.[16,17,18] Hence, there is enough evidence to substantiate the fact that the strong musculature of the Mandible has an influence on the mandible to bring about the flexure.
CONCLUSION
The Mean intermolar width is maximum for Brachyfacial type and average for Mesofacial type and minimum for Dolichofacial type of facial pattern in South Indian population with a tendency of broad arch forms in Brachyfacial and narrow archforms in Dolichofacial pattern
The Mean Mandibular Flexure values are maximum at maximum jaw opening position in all Brachyfacial, Mesofacial, and Dolichofacial type of facial pattern in South Indian population
The Mean Mandibular Flexure Values are maximum for Brachyfacial type and least for Dolichofacial type of facial pattern indicating the strong influence of musculature on the facial Pattern
There is no sex difference in the Mean MMF values between Males and Females.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Lee RT. Arch width and form: A review. Am J Orthod Dentofacial Orthop. 1999;115:305–13. doi: 10.1016/S0889-5406(99)70334-3. [DOI] [PubMed] [Google Scholar]
- 2.Abu Alhaija ES, Al Zo’ubi IA, Al Rousan ME, Hammad MM. Maximum occlusal bite forces in Jordanian Individuals with different dentofacial vertical skeletal patterns. Eur J Orthod. 2010;32:71–7. doi: 10.1093/ejo/cjp069. [DOI] [PubMed] [Google Scholar]
- 3.Abdel-Latif HH, Hobkirk JA, Kelleway JP. Functional mandibular deformation in edentulous subjects treated from with dental implants. Int J Prosthodont. 2000;13:513–9. [PubMed] [Google Scholar]
- 4.Du Brul EL, Sicher H. Springfield III: Charles.C Thomas Publisher; 1954. The adaptive chin. [Google Scholar]
- 5.Hobkirk JA, Schwab J. Mandibular deformation in subjects with osseointegratedimplants. Int J Oral Maxillofac Implants. 1991;6:319–28. [PubMed] [Google Scholar]
- 6.Chen DC, Lai YL, Chi LY, Lee SY. Contributing factors of mandibular deformation during mouth opening. J Dent. 2000;28:583–8. doi: 10.1016/s0300-5712(00)00041-5. [DOI] [PubMed] [Google Scholar]
- 7.Osborne J, Tomalin HR. Medial convergence of mandible. Br J. 1964;117:112–4. [Google Scholar]
- 8.Rickets RM, Roth RH, Chaconnas SJ. Orthodontic diagnosis and planning, Rocky mountain Data systems. 1982:53–118. [Google Scholar]
- 9.CanabarroSde A, Shinkai RS. Median mandibular flexure and maximum occlusal force in dentate subjects. Int J Prosthodont. 2006;19:177–82. [PubMed] [Google Scholar]
- 10.Nasby JA, Isaacson RJ, Worms FW, Speidel TM. Orthodontic extractions and the facial pattern. Angle Orthod. 1972;42:116–22. doi: 10.1043/0003-3219(1972)042<0116:OEATFS>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 11.Tsunori M, Mashita M, Kasai K. Relationship between facial types and tooth and bone characteristics of the mandible obtained by CT scanning. Angle Orthod. 1998;68:557–62. doi: 10.1043/0003-3219(1998)068<0557:RBFTAT>2.3.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Weijis WA, Hillen B. Relationship between masticatory muscle cross section and skull shape. J Dental Res. 1984;63:1154–7. doi: 10.1177/00220345840630091201. [DOI] [PubMed] [Google Scholar]
- 13.Satiroğlu F, Arun T, Işik F. Comparative data on facial morphology and muscle thickness using ultrasonography. Eur J Orthod. 2005;27:562–7. doi: 10.1093/ejo/cji052. [DOI] [PubMed] [Google Scholar]
- 14.Mathew CF, Elaine S, Chun-His C. Relationship between dental arch width and vertical facial morphology in un treated adults. Eur J Orthod. 2008;30:288–94. doi: 10.1093/ejo/cjm113. [DOI] [PubMed] [Google Scholar]
- 15.Van Spronsen PH, Weijs WA, Valk Prahl-Andersen JB, Van Ginkel FC. A Comparison of Jaw Muscle Cross-sections of Long-face and Normal Adults. J Dental Res. 1992;71:1279–85. doi: 10.1177/00220345920710060301. [DOI] [PubMed] [Google Scholar]
- 16.Kiliardis S, Kalebo P. Masseter muscle thickness measured by ultrasonography and its relation to facial morphology. J Dent Res. 1991;70:1262–5. doi: 10.1177/00220345910700090601. [DOI] [PubMed] [Google Scholar]
- 17.Weijs WA, Hillen B. Correlations between the Cross-Sectional Area of the Jaw Muscles and Craniofacial Size and Shape. Am J Phys Anthropol. 1986;70:423–31. doi: 10.1002/ajpa.1330700403. [DOI] [PubMed] [Google Scholar]
- 18.Benington PC, Gardener JE, Hunt NP. Masseter muscle volume measured byultrasonography and its relationship with facial morphology. Eur J Orthod. 1999;21:659–70. doi: 10.1093/ejo/21.6.659. [DOI] [PubMed] [Google Scholar]