

Abstract
Context:
Excessive ground reaction force when landing from a jump may result in lower extremity injuries. It is important to better understand how feedback can influence ground reaction force (GRF) and potentially reduce injury risk.
Objective:
To determine the effect of expert-provided (EP), self-analysis (SA), and combination EP and SA (combo) feedback on reducing peak vertical GRF during a jump-landing task.
Data Sources:
We searched the Web of Science database on July 1, 2011; using the search terms ground reaction force, landing biomechanics, and feedback elicited 731 initial hits.
Study Selection:
Of the 731 initial hits, our final analysis included 7 studies that incorporated 32 separate data comparisons.
Data Extraction:
Standardized effect sizes and 95% confidence intervals (CIs) were calculated between pretest and posttest scores for each feedback condition.
Data Synthesis:
We found a homogeneous beneficial effect for combo feedback, indicating a reduction in GRF with no CIs crossing zero. We also found a homogeneous beneficial effect for EP feedback, but the CIs from 4 of the 10 data comparisons crossed zero. The SA feedback showed strong, definitive effects when the intervention included a videotape SA, with no CIs crossing zero.
Conclusions:
Of the 7 studies reviewed, combo feedback seemed to produce the greatest decrease in peak vertical GRF during a jump-landing task.
Key Words: injury prevention, knee, feedback, landing biomechanics
Key Points.
All modes of feedback effectively reduced ground reaction force during a jump-landing task.
Combination feedback demonstrated the strongest effect sizes for reducing ground reaction force compared with expert-provided and self-analysis feedback.
More high-quality studies are needed to support the use of feedback interventions for altering lower extremity landing forces and decreasing lower extremity injury risk.
Landing is an essential athletic task used during many different sporting activities, including basketball, volleyball, and gymnastics.1–3 The act of jumping and landing during these different sporting activities involves different magnitudes of ground reaction forces (GRFs).4 The GRF magnitudes have been reported to be greatest during the landing phase of a jump when the knee is between 0° and 25° of flexion, a point at which the knee must resist a rapid change in kinetic energy.5 Excessive GRFs may result in lower extremity injuries.3,6–8
The knee is largely responsible for energy attenuation of the lower extremity when landing from a jump,9,10 so this joint may have increased susceptibility to injury during such a task. Researchers have identified the presence of damage to the subchondral bone, cartilage, and soft tissue due to extreme forces imposed on the lower extremity during selected landing activities.11 A positive moderate correlation between increased vertical GRF and increased anterior tibial acceleration when landing from a jump supports the hypothesis that individuals landing with greater impact loads could have an increased risk of anterior cruciate ligament (ACL) injury.12 Given that the main function of the ACL is preventing anterior translation of the tibia, landing with increased GRF and thus increased anterior tibial acceleration may place more strain on the ligament, increasing the likelihood of ligament rupture.
To reduce the risk of injury associated with increased GRF during landing, different interventions have been used to decrease GRF by altering lower extremity biomechanics during landing. To our knowledge, no researchers have evaluated whether reducing an individual's GRF decreases his or her risk of injury, but compelling data have suggested that higher GRF and other factors may increase the risk of substantially injuring the knee.13 Specifically, prospective data have shown that GRF during a jump-landing task was 20% higher in female athletes who sustained an ACL rupture than in athletes who did not.13 These data spark a compelling but unsubstantiated theory that reducing high GRFs may coincide with a decreased risk of knee injury. Clinical trials to evaluate the true prophylactic capabilities of reducing GRF to limit knee injuries are likely expensive and logistically difficult to conduct. Therefore, successfully identifying an intervention that can manipulate GRF is important before these studies are performed.
Various methods have been implemented to teach proper landing biomechanics to prevent future injury.14 For example, feedback is a modality used to prompt an individual to correct potentially harmful biomechanics and reduce high GRF. Feedback can be defined as sensory information made available to the participant during or after a task in an attempt to alter a movement.15 It can include information related to the sensations associated with the movement (eg, the feel or sound the participant experiences while performing the task) or related to the result of the action with respect to the environmental goal.15 Different modes of feedback have been reported and include (1) expert-provided (EP) feedback through oral correction,16 oral instruction,17,18 or visual demonstration16; (2) self-analysis (SA) feedback conducted with videotape correction19,20 or self-correction from previous trials17; and (3) combination (combo) feedback that uses both EP and SA feedback.19,21 Through EP feedback, professionals can analyze movements and provide various forms of oral and visual feedback to alter that task, whereas SA feedback requires the participant to identify movement characteristics that need to be altered and to adjust to change that specific task.
Recently, a surge of injury-prevention programs have been implemented to reduce the risk of ACL injury in athletes.22,23 These programs often incorporate feedback techniques and aim to reduce the risk of injury by teaching athletes to land properly to reduce stress on the lower extremity and potentially prevent acute and chronic lower extremity injuries.19 Altering the landing phase of a jump via various feedback methods could result in decreased GRFs and increased flexion angles at the knee, which may decrease the risk of lower extremity injury.
Although programs incorporating feedback are increasing in popularity, the magnitude of the effect that different types of feedback have on reducing GRF has not been evaluated systematically. Knowledge of the efficacy of feedback on reducing potentially harmful GRF may help clinicians determine whether feedback should be incorporated into jump-landing training programs. Therefore, the purpose of our study was to systematically evaluate the current literature to determine the magnitude of immediate and delayed effects of EP, SA, and combo feedback interventions on reducing peak vertical GRF during a jump-landing task in healthy individuals.
METHODS
Data Acquisition
We conducted a Web-based search using the Web of Science with the search terms landing biomechanics, ground reaction force, and feedback (Figure). We included all studies that were written in English and published between 1950 and July 1, 2011, and were investigations of the effects of oral or sensory feedback on peak vertical GRF. Studies including a comparison group or condition not receiving a feedback intervention and studies not including a comparison or control group were included in this review. Bibliographies from all relevant articles were cross-referenced for additional pertinent studies that would fit inclusion criteria. We evaluated the methodologic quality for all articles used in the final analysis. If articles had not been assessed by the Centre for Evidence-Based Physiotherapy (PEDro), 2 separate investigators (H.M.E. and B.G.P.) independently assessed each article, compared ratings, and if differences were present, conversed to agree on a PEDro score for each study. The body of feedback literature also was rated based on the Oxford Centre for Evidenced-Based Medicine–Levels of Evidence.24
Data Extraction
Authors of all studies included in this review investigated the effect of feedback on GRFs in healthy participants (Table 1). We separated the studies based on the type of feedback used: EP, SA, combo, and control (Table 1). We chose these categories based on how the feedback was delivered to the participants. Some overlap occurred among groups concerning how the feedback was processed (ie, oral, visual, cognitive), but we believed this was the most effective and clearest way to categorize these groups because the literature was so varied.
Table 1.
Study Characteristics
| Study Name |
Study Design |
Type of Feedback |
PEDro Score, Oxford Level of Evidence |
Methodologic Concerns |
Population |
Force Plate Used |
Landing Task |
| Herman et al, 200921 | Randomized controlled trial | Strength/ combo FB, combo FB | 6/10, 1b | No concealed allocation and no blinding of participants, therapists, or assessors | 58 healthy female recreational athletes | 2 Berteca 4060 A force plates collected at 1200 samples per channel per second | 4-step approach run, 2- footed landing onto force plate, and 2-footed takeoff for maximal height |
| Prapavessis et al, 200318 | Cohort study | EP immediate, EP 2 d, EP 4 d, EP 3 mo | 5/10, 2b | No concealed or random allocation and no blinding of participants, therapists, or assessors | 20 healthy male and 41 healthy female school-aged children | AMTIb force plate collected at 1000 Hz | 4 successive step-offs from a 300-mm box onto the force plate, landing in a balanced position on both feet |
| Prapavessis and McNair, 199917 | Randomized controlled trial | EP and SA | 6/10, 2b | No concealed allocation; no blinding of participants, therapists, or assessors; and no statement of outcome variables obtained for >85% of participants | 56 healthy male and 35 healthy female high school students | AG Kistlerc force plate collected at 1000 Hz | Jump from a 300-mm box, landing in a balanced position on both feet |
| Onate et al, 200120 | Randomized controlled trial | SA 2 min, SA 1 wk | 6/10, 2b | No concealed allocation and no blinding of participants, therapists, or assessors | 21 healthy male and 42 healthy female university students | 2 Bertec force plates collected at 540 Hz for 4 s | Maximal vertical jump with Vertec deviced |
| Onate et al, 200519 | Randomized controlled trial | EP, EP 1 wk, SA videotape, SA videotape 1 wk | 5/10, 2b | No concealed allocation; no blinding of participants, therapists, or assessors; and no statement of outcome variables obtained for >85% of participants | 51 healthy male and female university students | 2 Bertec analog force plates collected at 1000 Hz | 4-m running approach, starting take off with left foot contacting tape placed at 30% of maximal standing arm reach. Single-leg takeoff onto force plates, landing with 2 feet, jumping to simulate grabbing a basketball, and landing on the force plate with 2 feet |
| Cronin et al, 200816 | Case series | EP | 5/10, 4 | No concealed or random allocation and no blinding of participants, therapists, or assessors | 15 female NCAA Division I volleyball players | Bertec force plate collected at 500 Hz for 3 s | Volleyball spike, landing on both feet with 1 foot on the force plate |
| Walsh et al, 200725 | Randomized controlled trial | EP | 6/10, 2b | No concealed or random allocation and no blinding of participants, therapists, or assessors | 25 NCAA Division I basketball players | Bertec force plate collected at 1000 Hz | 3 drop jumps from a 30.5-cm box then jump for maximal height |
Abbreviations: combo, combination; EP, expert provided; FB, feedback; NCAA, National Collegiate Athletic Association; PEDro, Centre for Evidence-Based Physiotherapy; SA, self-analysis.
Bertec Corporation, Columbus, OH.
AMTI, Watertown, MA.
Kistler Instrument Corp, Novi, MI.
Sports Imports, Columbus, OH.
We defined EP feedback as feedback provided by an expert either orally or through demonstration. An expert was defined as one who is knowledgeable in proper landing biomechanics and can demonstrate such to a participant during a jump-landing task. The expert provided sensory feedback through visual or auditory modes; the participant then cognitively absorbed the feedback. We defined SA feedback as feedback conducted through videotape or SA of the participant's own previous performance during a jump-landing task. Some participants were instructed to use their previous experience to land more softly,17,20 whereas other participants were instructed to analyze videotape of their past performances on their own without further feedback.19 Self-analysis feedback required the participant to use visual, auditory, and cognitive modes to absorb the feedback. Combo feedback was defined as feedback delivered both from an expert and using videotape or SA. It required visual, auditory, and cognitive modes. Different control interventions were used for each study. Some control participants19 received no feedback, whereas other participants classified as controls18,20 were instructed to “try to land as softly as possible.” We believed the control groups that were given some type of prejump instruction, such as “try to land as softly as possible,” were not true control groups; therefore, we chose to include only control groups that received no prejump instruction. Furthermore, some researchers16,17,21 did not include a nonfeedback control group.
We further separated the studies based on the timing of the feedback: immediate postfeedback effects and delayed postfeedback effects (range, 2 days to 3 months). Effects were categorized as immediate if the postintervention testing occurred immediately after the intervention. Effects were categorized as delayed if the postintervention testing occurred more than 1 day after the intervention took place.
Data Analysis
From each study, we collected means and standard deviations of peak vertical GRF preintervention and postintervention as well as the number of participants. The researchers did not provide the number of participants in 1 study,18 but we obtained this information from the authors via e-mail. Investigators provided a figure of means and standard deviations but did not publish specific values in another study.26 We attempted to contact the authors of this study via e-mail but could not obtain the information; therefore, we excluded the article from this review. Standardized effect sizes (ES) were calculated for 32 data sets, which incorporated interventions from all 7 articles. The ES evaluated the magnitude of the treatment effects (Cohen d = [postfeedback − prefeedback] / pooled SD) and were interpreted using previous recommendations (0.2 = small, 0.5 = moderate, and 0.8 = large).27 In addition, 95% CIs were calculated to assess associated variability around the ES point measure.
RESULTS
In the initial search, we found 731 articles (Figure). Ten articles were included after reading the titles. Four of those were excluded after reading the abstracts. After cross-referencing the remaining 6 articles, we found 1 other article21 that fit the inclusion criteria and included it. Therefore, we included 7 studies in this analysis (Figure; Table 1).16–21,25
Figure. .

Study inclusion and exclusion flowchart.
Methodologic Assessment
The mean PEDro scoring for the articles included in this review was 5.57 ± 0.53 (range, 5 to 6 out of a possible 10). Based on the Oxford Centre for Evidence-Based Medicine,24 levels of evidence for individual studies ranged from 1b (randomized control trial with narrow CIs) to 4 (case series) (Table 1).
Expert-Provided Feedback
We used 10 data sets from 5 articles in this comparison and found a homogeneous negative effect for those receiving EP feedback, indicating a reduction in GRF during the jump landing (Table 2). Nine of 10 data sets in the EP group had moderate to strong ES (Cohen d range, −0.26 to −1.49). Four of 10 data sets18,19,25 had CIs that crossed zero, indicating that a definitive effect in the reduction of the GRF may not be present within all of the data sets (Table 2).
Table 2.
Expert-Provided Feedback
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Walsh et al, 200725 | Expert-provided feedback, females | −0.8 (−1.91, 0.43) |
| Walsh et al, 200725 | Expert-provided feedback, males | −0.26 (−1.38, 0.89) |
| Cronin et al, 200816 | Expert-provided feedback | −0.88 (−1.61, −0.11) |
| Onate et al, 200519 | Expert-provided feedback | −0.85 (−1.65, 0.02) |
| Prapavessis et al, 200318 | Expert-provided feedback, immediate | −1.49 (−2.03, −0.91) |
| Prapavessis and McNair, 199917 | Expert-provided feedback | −0.73 (−1.17, −0.27) |
| Prapavessis et al, 200318 | Expert-provided feedback, 2 d | −0.92 (−1.43, −0.38) |
| Prapavessis et al, 200318 | Expert-provided feedback, 4 d | −1.2 (−1.72, −0.64) |
| Prapavessis et al, 200318 | Expert-provided feedback, 3 mo | −0.48 (−0.97, 0.03) |
| Onate et al, 200519 | Expert-provided feedback, 1 wk | −0.94 (−1.74, −0.06) |
Self-Analysis Feedback
We used 5 data sets from 3 articles in this comparison and found a homogeneous negative effect, indicating a reduction in GRF for those receiving SA feedback (Table 3). Self-analysis feedback showed strong, definitive ES (Cohen d = −3.32 and −4.37) with no CI crossing zero if the intervention included a videotape SA.19 Conversely, SA feedback interventions that did not include a video analysis of the previous jumps had weak ES (Cohen d range, −0.11 to −0.41) (Table 3).17,20
Table 3.
Self-Analysis Feedback
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Prapavessis and McNair, 199917 | Self-analysis feedback | −0.11 (−0.5, 0.28) |
| Onate et al, 200120 | Self-analysis feedback, 2 min | −0.15 (−0.86, 0.57) |
| Onate et al, 200519 | Self-analysis feedback videotape | −3.32 (−4.41, −2.0) |
| Onate et al, 200519 | Self-analysis feedback videotape, 1 wk | −4.37 (−5.66, −2.78) |
| Onate et al, 200120 | Self-analysis feedback, 1 wk | −0.41 (−1.12, 0.32) |
Combination Feedback
We used 6 data sets from 3 articles in this comparison and found a homogeneous negative effect for those receiving combo feedback, again indicating a reduction in GRF during the jump-landing task due to the combo intervention (Table 4).19–21 Moderate ES (Cohen d = −0.6 and −0.66) with CIs that did not cross zero were calculated for data sets of Herman et al21 representing combination feedback and combination feedback and strength training. The data sets of Onate et al20 representing combination feedback and combination feedback 1 week showed strong ES (Cohen d = −0.99 and −0.8) with CIs that did not cross zero. The 2 data sets of Onate et al19 representing combination feedback and combination feedback 1 week showed strong ES (Cohen d = −1.53 and −0.8) with CIs that did not cross zero.
Table 4.
Combination Expert-Provided and Self-Analysis Feedback
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Herman et al, 200921 | Combination feedback and strength training | −0.66 (−0.16, −1.15) |
| Herman et al, 200921 | Combination feedback | −0.6 (−0.1, −1.08) |
| Onate et al, 200120 | Combination feedback, 2 min | −0.99 (−0.26, −1.68) |
| Onate et al, 200519 | Combination feedback | −1.53 (−0.61, −2.35) |
| Onate et al, 200519 | Combination feedback, 1 wk | −1.78 (−2.62, −0.82) |
| Onate et al, 200120 | Combination feedback, 1 wk | −0.8 (−1.48, −0.08) |
Control
We used 6 data sets from 4 articles in this comparison. The results of the control data showed a heterogeneous effect on altering GRF (Table 5). Two data sets representing control and control 1 week in the study by Onate et al19 had strong ES (Cohen d = −1.59 and −1.35) and CIs that did not cross zero. Four of the 6 control group data sets had weak ES18,20,25 with wide CIs that crossed zero.
Table 5.
Control Groups
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Onate et al, 200519 | Control | −1.59 (−0.7, −2.38) |
| Onate et al, 200120 | Control, 2 min | −0.18 (0.55, −0.89) |
| Walsh et al, 200725 | Control, females | 0.09 (−1.05, 1.21) |
| Walsh et al, 200725 | Control, males | 0.12 (−1.03, 1.24) |
| Onate et al, 200519 | Control, 1 wk | −1.35 (−2.13, −0.49) |
| Onate et al, 200120 | Control, 1 wk | −0.03 (−0.72, 0.67) |
Immediate Effects of Feedback
We used 13 data sets from 7 articles in this comparison. This included data sets from the EP, SA, and combo groups investigating the immediate effects of the feedback intervention. A homogeneous negative effect was found immediately after all types of feedback, with most data sets having moderate to strong ES (Table 6). Three of the data sets17,20,25 had small ES with nondefinitive CIs crossing zero. Two EP feedback interventions19,25 had strong immediate effects (Cohen d = −0.85 and −0.8) with nondefinitive CIs that crossed zero.
Table 6.
Immediate Effects of Feedback Training
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Walsh et al, 200725 | Expert-provided feedback, females | −0.8 (−1.91, 0.43) |
| Walsh et al, 200725 | Expert-provided feedback, males | −0.26 (−1.38, 0.89) |
| Herman et al, 200921 | Combination feedbacka and strength training | −0.66 (−1.15, −0.16) |
| Herman et al, 200921 | Combination feedback | −0.6 (−1.08, −0.1) |
| Prapavessis and McNair, 199917 | Expert-provided feedback | −0.73 (−1.17, −0.27) |
| Prapavessis and McNair, 199917 | Self-analysis feedback | −0.11 (−0.5, 0.28) |
| Cronin et al, 200816 | Expert-provided feedback | −0.88 (−1.61, −0.11) |
| Onate et al, 200519 | Expert-provided feedback | −0.85 (−1.65, 0.02) |
| Onate et al, 200519 | Self-analysis feedback, videotape | −3.32 (−4.41, −2.0) |
| Onate et al, 200519 | Combination feedback | −1.53 (−2.35, −0.61) |
| Onate et al, 200120 | Combination feedback, 2 min | −0.99 (−1.68, −0.26) |
| Onate et al, 200120 | Self-analysis feedback, 2 min | −0.15 (−0.86, 0.57) |
| Prapavessis et al, 200318 | Expert-provided feedback | −1.49 (−2.03, −0.91) |
Combination feedback combines expert-provided and self-analysis feedback.
Delayed Effects of Feedback
We used 8 data sets from 3 articles in this comparison. Strong effects were seen in data sets from each of the 3 groups (EP, SA, combo). The delayed effects of feedback also had a homogeneous negative effect, suggesting a reduction in GRF (Table 7). Most of the data sets showed moderate to high ES. Three of the 8 data sets showed weak ES and had CIs that crossed zero.18,20
Table 7.
Delayed Effects of Feedback Training
| Authors |
Data Set |
Effect Size (95% Confidence Interval) |
| Onate et al, 200519 | Expert-provided feedback, 1 wk | −0.94 (−1.74, −0.06) |
| Onate et al, 200519 | Self-analysis feedback, videotape, 1 wk | −4.37 (−5.66, −2.78) |
| Onate et al, 200519 | Combinationa feedback, 1 wk | −1.78 (−2.62, −0.82) |
| Onate et al, 200120 | Combination feedback, 1 wk | −0.43 (−0.36, 1.19) |
| Onate et al, 200120 | Self-analysis feedback, 1 wk | −0.41 (−1.12, 0.32) |
| Prapavessis et al, 200318 | Expert-provided feedback, 2 d | −0.92 (−1.43, −0.38) |
| Prapavessis et al, 200318 | Expert-provided feedback, 4 d | −1.2 (−1.72, −0.64) |
| Prapavessis et al, 200318 | Expert-provided feedback, 3 mo | −0.48 (−0.97, 0.03) |
Combination feedback combines expert-provided and self-analysis feedback.
DISCUSSION
The presence of excessive GRF may result in lower extremity injury.3,6–8 To reduce GRF during jump landing, different injury-prevention programs have been implemented to teach individuals how to use safer landing biomechanics. Feedback given either orally or through demonstration has been incorporated in these injury-prevention programs. Researchers have shown that if participants are instructed to perform a soft landing (ie, one with lower GRF), their muscles can absorb up to 19% more kinetic energy than if they perform a hard landing (ie, one with higher GRF).9 If the muscular system can absorb some of the kinetic energy, the structures of the joints, specifically the knee joint, may not have to attenuate as much energy, which may reduce the risk of knee injury.
The methodologic quality of the current literature regarding the effect of feedback on reduction of GRF is moderate. The highest PEDro score was 6 out of 10, with an average of 5.43 ± 0.53 (Table 8). The authors of the included studies did not conceal group allocation and did not use any level of blinding to decrease bias. Given the nature of these studies and the methods used to perform the intervention, blinding participants, assessors, or therapists to their groups is very difficult. Given the protocol of providing different types of feedback, blinding participants and therapists to the type of feedback is difficult, and points were lost in these categories using the PEDro scoring system. Therefore, one should consider this when assessing the methodologic quality of these studies. Two studies17,19 lost points for not stating whether outcome measures were obtained for more than 85% of the participant population initially included. Levels of evidence ranged from 1b to 4 based on the recommendations from the Oxford Centre for Evidence-Based Medicine.24 The wide CIs for ES in the included randomized controlled trials and cohort designs prevented these studies from being classified as higher-tier levels of evidence (Table 1).
Table 8.
Feedback and Control Interventions
| Study Name |
Intervention Timing |
Feedback Intervention |
Instructions Given |
Control Intervention |
|
| Immediate |
Long-Term |
||||
| Herman et al, 200921 | Prefeedback test, postfeedback test | NA | Combo: 9-wk strength intervention, then prefeedback data collection. Participants performed 2 stop-jump tasks and watched their own trials and 2 trials of an expert. Each trial was watched once at normal speed and once with trial paused at moment of foot contact. Participants were given a checklist for landing. After feedback, they performed 5 stop-jump trials then a repeat feedback protocol for a total of 3 feedback sessions. No feedback was given during the jump task. | Checklist: Did you land (1) with both feet at the same time? (2) in a neutral knee valgus/varus position? (3) with feet shoulder-width apart? (4) on forefoot and rolling toward rearfoot? and (5) with optimal knee and hip flexion at initial contact? | Participants refrained from strength training for 9 wk, then same feedback data collection. No nonfeedback control. |
| Prapavessis et al, 200318 | Prefeedback test, postfeedback test | 2 d, 4 d, 3 mo | EP: During sessions immediate and 2 d, 4 d, and 3 mo postfeedback, intervention groups were given specific oral instructions. During the 3-mo postfeedback session, participants were instructed to land as softly as possible and to recall as many of the instructional points as possible. | The instructions for landing: “When you do your next jump, position yourself on the balls of your feet with bent knees just prior to landing, then lower the heels slowly to the ground and bend your knees until well after the landing. Use the sound to your landing to tell you how softly you have landed.” | Participants were instructed to land as softly as possible. No other feedback was given. |
| Prapavessis and McNair, 199917 | Prefeedback test, postfeedback test | NA | EP: Participants were instructed to land as softly as possible and given instructions. SA: Participants were instructed to land as softly as possible, given instructions, and directed to use the experience of their first jump to land in a manner that would minimize the stress of their next landing. They were not given further instruction. | EP: “We want you to jump off box and land in a manner that will minimize the stress of the landing.” “When doing your next jump, position yourself on the balls of your feet with bent knees just prior to landing. On landing, lower the heels slowly to the ground and bend the knees until well after landing.” SA: “We want you to jump off this box and land in a manner that will minimize the stress of the landing.” | NA |
| Onate et al, 200120 | Prefeedback test, postfeedback test | 1 wk | Combo: Participants were given oral and visual feedback for 2 min using videotape of their own jumps to determine how to land more softly with maximal jump height. Participants were instructed to document what they could do to land more softly and instructed to jump 5 more times after reading instructions A and B. SA: Participants had 2 min to self-analyze their jumps using internal experience to determine how to land more softly while maintaining maximal jump height. Participants were instructed to document what they could do to land more softly and to jump 5 more times after reading instructions A and B. | All groups read and were read aloud the following: “(A) You are not to take any steps before jumping, but you may squat or swing your arms to aid in jumping. (B) The goal of the takeoff is to jump as high as you can by hitting the Verteca vanes with your dominant hand (the hand you chose to throw a ball with) and to land as softly as you can back onto the force plate with both feet landing on the force plate.” | Control 1: Participants were given 2 min to relax and were not given feedback about the jumps. They were instructed to jump 5 more times after reading instructions A and B. Control 2: Participants were not given feedback about the jumps. |
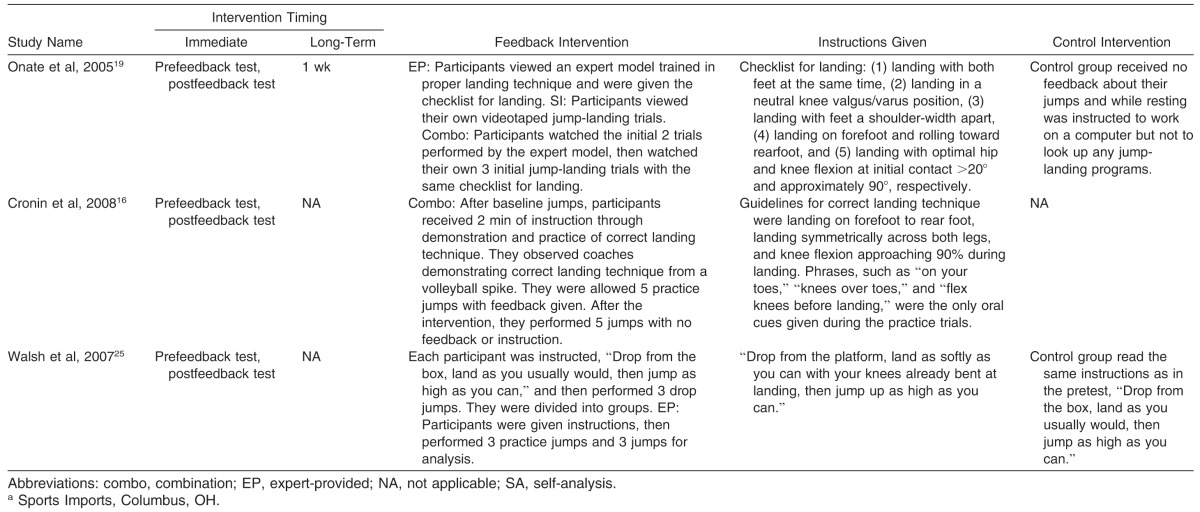
| Onate et al, 200519 | Prefeedback test, postfeedback test | 1 wk | EP: Participants viewed an expert model trained in proper landing technique and were given the checklist for landing. SI: Participants viewed their own videotaped jump-landing trials. Combo: Participants watched the initial 2 trials performed by the expert model, then watched their own 3 initial jump-landing trials with the same checklist for landing. | Checklist for landing: (1) landing with both feet at the same time, (2) landing in a neutral knee valgus/varus position, (3) landing with feet a shoulder-width apart, (4) landing on forefoot and rolling toward rearfoot, and (5) landing with optimal hip and knee flexion at initial contact >20° and approximately 90°, respectively. | Control group received no feedback about their jumps and while resting was instructed to work on a computer but not to look up any jump-landing programs. |
| Cronin et al, 200816 | Prefeedback test, postfeedback test | NA | Combo: After baseline jumps, participants received 2 min of instruction through demonstration and practice of correct landing technique. They observed coaches demonstrating correct landing technique from a volleyball spike. They were allowed 5 practice jumps with feedback given. After the intervention, they performed 5 jumps with no feedback or instruction. | Guidelines for correct landing technique were landing on forefoot to rear foot, landing symmetrically across both legs, and knee flexion approaching 90% during landing. Phrases, such as “on your toes,” “knees over toes,” and “flex knees before landing,” were the only oral cues given during the practice trials. | NA |
| Walsh et al, 200725 | Prefeedback test, postfeedback test | NA | Each participant was instructed, “Drop from the box, land as you usually would, then jump as high as you can,” and then performed 3 drop jumps. They were divided into groups. EP: Participants were given instructions, then performed 3 practice jumps and 3 jumps for analysis. | “Drop from the platform, land as softly as you can with your knees already bent at landing, then jump up as high as you can.” | Control group read the same instructions as in the pretest, “Drop from the box, land as you usually would, then jump as high as you can.” |
Abbreviations: combo, combination; EP, expert-provided; NA, not applicable; SA, self-analysis.
Sports Imports, Columbus, OH.
Our systematic review provides evidence that feedback interventions effectively reduce GRF during a jump-landing task. Some differences existed in the jump-landing tasks used in each study (Table 1), but when evaluating the ES, we found all types of feedback (EP, SA, combo) had a homogeneous effect in reducing GRF. The combo feedback seemed to produce the greatest decrease in peak vertical GRF during a jump-landing task, with all data sets having moderate to large ES and no CIs crossing zero. This indicates that a reduction in GRF and a potential reduction in risk of injury may be better obtained through the combo feedback. This could include an expert demonstrating the proper landing mechanics, an expert giving oral feedback to the participant, the participant viewing previous jump-landing trials, or the participant being instructed to use his or her experience in previous jumps to make alterations to reduce GRF while landing. We believe that combo feedback may have had the greatest effect on decreasing GRF because it affected neuromuscular control patterns via inputs from a wide variety of stimuli. This may have allowed the participants to individually select the most influential stimuli or combination of stimuli to best alter their biomechanics.
The results of the EP group showed mostly moderate to strong ES, with only 4 of 10 data sets having CIs that crossed zero (Table 2). This provides evidence for the effectiveness of EP feedback in reducing GRF during a jump-landing task. In the EP groups, the feedback was given through demonstration by an expert, oral feedback, or a combination of both.
We found differences in the outcomes between SA interventions that included and did not include videotape SA (Table 3). However, these results should be interpreted cautiously because the videotape SA was from 1 study.19 This appears to suggest that the use of videotape provides a greater reduction in GRF than SA feedback without the use of videotape analysis; however, further research is needed to strengthen this argument.
The ES representing the SA interventions using videotape were large and more comparable to the ES representing the EP interventions. This could suggest that any intervention using videotape or demonstration in which the participants can see either themselves or an expert performing the task may be more beneficial in decreasing GRF during a jump-landing task. In the future, researchers should investigate the effect of a participant watching an expert demonstrate the task and a participant watching his or her own trials of the task on reducing GRF.
We classified feedback in different categories, but some overlap of the sensory systems used to absorb the feedback may exist. For example, the SA feedback method requires the participants to rely mainly on cognitive information to absorb the feedback, whereas with the EP feedback method, more emphasis is placed on sensory processing through visual or auditory means. We recognize that the EP feedback method also includes some cognitive element working in conjunction with the sensory information being provided to the participant. For the purpose of our review, we classified studies based on how the feedback was delivered and not necessarily on how it was being processed because we wanted to determine the most effective way to deliver the feedback to reduce GRF during a jump-landing task.
Most of the data sets representing the control groups showed weak, negative ES with CIs that crossed zero, indicating small and inconclusive effects for control interventions. However, 2 control data sets in 1 study had strong ES (Cohen d = −1.59 and −1.35) and CIs that did not cross zero.19 These specific control participants did not receive feedback during the jump-landing trials, and they were instructed to work on a computer but not to investigate anything concerning jump-landing programs.19 The control group possibly improved in this 1 study due to a learning effect created from participating in the pretest.19 The authors of this study also used a different jump-landing task that involved a running approach. It is possible that the nature of the running approach allowed control participants to implement strategies to reduce GRF during landing that were different from the strategies participants used with the jump-landing task in the other studies. As mentioned, we did not include control groups that received prejump instruction, such as “try to land as softly as possible,” which may have changed their landing. We believed excluding these control groups allowed for a more accurate representation of a true control group that received no feedback or instruction before completing the task. Overall, the data for the control group had inconclusive results, likely due to the variety of methods used within the various study designs.
Making a definitive conclusion about the delayed effects of feedback is difficult because the included studies18–20 had different timeframes for follow-up (range, 2 days to 3 months). Given these results, we cannot definitively conclude which feedback intervention may have sustainable effects in reducing GRF during a jump landing. None of the authors investigated the effect of multiple feedback sessions over an extended period on the reduction of GRF. Researchers who investigated the effect of feedback on GRF over time conducted only 1 feedback session and had the participants return for a posttest (range, 2 days to 3 months).18–20 Although good results may have been demonstrated with 1 feedback session, we do not know the proper dosage and frequency of feedback that should be administered for optimal results to be elicited. Therefore, future researchers may investigate the effects of multiple feedback interventions over an extended period.
Whereas the physiologic mechanisms surrounding the possible beneficial effect of feedback are poorly understood, the modality can be explained as a means of instruction that supplies extrinsic information to the participant to improve motor learning.20 The participants receiving feedback are being given information about how to change their landing mechanics to decrease their GRF. Some participants may be unaware of proper landing mechanics or the potential detrimental effects of increased GRF during landing. Feedback is education and insight given to encourage the participants to become aware of how they are landing and to make positive changes to decrease their risks for lower extremity injury.
The cost-effectiveness of both EP and SA feedback may be different depending on the clinical setting. The SA feedback may be best administered using videotape SA, which may cost money and requires space for proper setup; yet, EP feedback requires substantial time commitments by trained professionals with jump-landing experience. Although the combo feedback seems to provide the strongest effects for GRF reduction, clinicians need to determine which type of feedback is more cost- and time-effective for their individual settings.
Limitations
Our study had limitations. The studies reviewed included different cohorts of people for their participant populations, which may make comparisons across studies more difficult (Table 1). The authors of each study also used different jump-landing techniques, including a running approach jump,19,21 a maximal vertical jump,20 a volleyball spike,16 and jumping or stepping off a box at a height of 300 mm.17,18,25 Although the differences in the landing tasks themselves may not be limitations, the various methods may limit our ability to make comparisons among studies.
Another possible limitation was that the included studies had unique ways of providing feedback to the participants during the jump-landing task, which made categorization of the groups more difficult. Each study delivered the feedback similarly, and the results revealed a homogeneous negative effect, showing a reduction in GRF across all types of feedback. The authors also defined their control groups differently, and some researchers did not include control groups. Another difference observed in each study was the timeframe for follow-up. As mentioned, researchers used many different timeframes for delayed follow-up, which made it difficult to derive a strong conclusion on the effects of feedback over time.
We recognize that these types of feedback could be categorized in several different ways, including how the feedback is delivered (EP or SA), how the feedback is processed (cognitive, visual, or oral), and the focus of the feedback (knowledge of performance or knowledge of results). We categorized the feedback by how it was delivered to investigate the most effective method of delivery to achieve the desired result, which was a reduction in GRF during a jump-landing task. Thinking about other ways to categorize feedback may be important, but we believed this was a good way to represent the data so they could be interpreted easily and important conclusions could be drawn.
Although limitations and differences existed among the studies reviewed, we still provided a meaningful analysis regarding the magnitude of the effect of different types of feedback on GRF reduction. Our results suggest the best way to provide feedback to reduce GRF during a jump-landing task is to include combo feedback during the task.
Recommendations for Future Research
Given the limited number of available studies, more research on the effects of feedback on GRF during a jump-landing task clearly is needed. Further research and clinical interventions to decrease vertical GRF during a jump-landing task should involve combo feedback. Emphasis should be placed on determining the most effective way to orally deliver EP feedback along with SA feedback. More information is needed on different cohorts of participants and which may be the best jump-landing task to study the effects of feedback. In the future, researchers also should try to determine a more definitive conclusion about the delayed effects of feedback and to define a timeframe for the lasting effects of feedback. Time should be devoted to determining whether a long-term feedback training program with multiple feedback sessions will produce substantial long-term changes in landing forces.
CONCLUSIONS
The studies in our review provided support for the use of both EP and SA feedback in reducing GRF during a jump-landing task. All studies showed a homogeneous negative effect, meaning GRF was reduced after the feedback was administered. Our findings suggest that although all types of feedback showed some reduction in GRF, combo feedback may be most effective in reducing GRF and possibly reducing the risk of injury. More high-quality research studies are needed in this area to further support the use of feedback techniques for altering lower extremity landing forces.
Table 8.
Continued
REFERENCES
- 1.Hrysomallis C. Relationship between balance ability, training and sports injury risk. Sports Med. 2007;37(6):547–556. doi: 10.2165/00007256-200737060-00007. [DOI] [PubMed] [Google Scholar]
- 2.Marshall SW, Covassin T, Dick R, Nassar LG, Agel J. Descriptive epidemiology of collegiate women's gymnastics injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):234–240. [PMC free article] [PubMed] [Google Scholar]
- 3.Dufek JS, Bates BT. Biomechanical factors associated with injury during landing in jump sports. Sports Med. 1991;12(5):326–337. doi: 10.2165/00007256-199112050-00005. [DOI] [PubMed] [Google Scholar]
- 4.Yeow CH, Lee PV, Goh JC. Regression relationships of landing height with ground reaction forces, knee flexion angles, angular velocities and joint powers during double-leg landing. Knee. 2009;16(5):381–386. doi: 10.1016/j.knee.2009.02.002. [DOI] [PubMed] [Google Scholar]
- 5.Podraza JT, White SC. Effect of knee flexion angle on ground reaction forces, knee moments and muscle co-contraction during an impact-like deceleration landing: implications for the non-contact mechanism of ACL injury. Knee. 2010;17(4):291–295. doi: 10.1016/j.knee.2010.02.013. [DOI] [PubMed] [Google Scholar]
- 6.Johnson K. Tears of cruciate ligaments of the knee: US Armed Forces: 1990–2002. Med Surveillance Monthly Rep. 2003;9:2–6. [Google Scholar]
- 7.Kirkendall DT, Garrett WE., Jr The anterior cruciate ligament enigma: injury mechanisms and prevention. Clin Orthop Relat Res. 2000;372:64–68. doi: 10.1097/00003086-200003000-00008. [DOI] [PubMed] [Google Scholar]
- 8.Frobell RB, Roos HP, Roos EM, et al. The acutely ACL injured knee assessed by MRI: are large volume traumatic bone marrow lesions a sign of a severe compression injury? Osteoarthritis Cartilage. 2008;16(7):829–836. doi: 10.1016/j.joca.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 9.Devita P, Skelly WA. Effect of landing stiffness on joint kinetics and energetics in the lower extremity. Med Sci Sports Exerc. 1992;24(1):108–115. [PubMed] [Google Scholar]
- 10.Hargrave MD, Carcia CR, Gansneder BM, Shultz SJ. Subtalar pronation does not influence impact forces or rate of loading during a single-leg landing. J Athl Train. 2003;38(1):18–23. [PMC free article] [PubMed] [Google Scholar]
- 11.Mizrahi J, Susak Z. Analysis of parameters affecting impact force attenuation during landing in human vertical free fall. Eng Med. 1982;11(3):141–147. doi: 10.1243/emed_jour_1982_011_039_02. [DOI] [PubMed] [Google Scholar]
- 12.McNair PJ, Marshall RN. Landing characteristics in subjects with normal and anterior cruciate ligament deficient knee joints. Arch Phys Med Rehabil. 1994;75(5):584–589. [PubMed] [Google Scholar]
- 13.Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading on the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. doi: 10.1177/0363546504269591. [DOI] [PubMed] [Google Scholar]
- 14.Hewett TE, Lindenfeld TN, Riccobene JV, Noyes FR. The effect of neuromuscular training on the incidence of knee injury in female athletes: a prospective study. Am J Sports Med. 1999;27(6):699–706. doi: 10.1177/03635465990270060301. [DOI] [PubMed] [Google Scholar]
- 15.Winstein CJ. Knowledge of results and motor learning: implications for physical therapy. Phys Ther. 1991;71(2):140–149. doi: 10.1093/ptj/71.2.140. [DOI] [PubMed] [Google Scholar]
- 16.Cronin JB, Bressel E, Fkinn L. Augmented feedback reduces ground reaction forces in the landing phase of the volleyball spike jump. J Sport Rehabil. 2008;17(2):148–159. doi: 10.1123/jsr.17.2.148. [DOI] [PubMed] [Google Scholar]
- 17.Prapavessis H, McNair PJ. Effects of instruction in jumping technique and experience jumping on ground reaction forces. J Orthop Sports Phys Ther. 1999;29(6):352–356. doi: 10.2519/jospt.1999.29.6.352. [DOI] [PubMed] [Google Scholar]
- 18.Prapavessis H, McNair PJ, Anderson K, Hohepa M. Decreasing landing forces in children: the effect of instructions. J Orthop Sports Phys Ther. 2003;33(4):204–207. doi: 10.2519/jospt.2003.33.4.204. [DOI] [PubMed] [Google Scholar]
- 19.Onate JA, Guskiewicz KM, Marshall SW, Giuliani C, Yu B, Garrett WE. Instruction of jump-landing technique using videotape feedback: altering lower extremity motion patterns. Am J Sports Med. 2005;33(6):831–842. doi: 10.1177/0363546504271499. [DOI] [PubMed] [Google Scholar]
- 20.Onate JA, Guskiewicz KM, Sullivan RJ. Augmented feedback reduces jump landing forces. J Orthop Sports Phys Ther. 2001;31(9):511–517. doi: 10.2519/jospt.2001.31.9.511. [DOI] [PubMed] [Google Scholar]
- 21.Herman DC, Onate JA, Weinhold PS, et al. The effects of feedback with and without strength training on lower extremity biomechanics. Am J Sports Med. 2009;37(7):1301–1308. doi: 10.1177/0363546509332253. [DOI] [PubMed] [Google Scholar]
- 22.Hewett TE, Myer GD, Ford KR. Reducing knee and anterior cruciate ligament injuries among female athletes: a systematic review of neuromuscular training interventions. J Knee Surg. 2005;18(1):82–88. doi: 10.1055/s-0030-1248163. [DOI] [PubMed] [Google Scholar]
- 23.Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes: decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765–773. doi: 10.1177/036354659602400611. [DOI] [PubMed] [Google Scholar]
- 24.Phillips B, Ball C, Sackett D. Oxford Centre for Evidence-Based Medicine–Levels of Evidence (March 2009. http://222.cebm.net/?o=1025. Updated March 2009. Accessed December 4, 2012. [Google Scholar]
- 25.Walsh MS, Waters J, Kersting UG. Gender bias on the effects of instruction on kinematics and kinetic jump parameters of high-level athletes. Res Sports Med. 2007;15(4):283–295. doi: 10.1080/15438620701693306. [DOI] [PubMed] [Google Scholar]
- 26.McNair PJ, Prapavessis H, Callender K. Decreasing landing forces: effect of instruction. Br J Sports Med. 2000;34(4):293–296. doi: 10.1136/bjsm.34.4.293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Cohen J. Statistical power analysis for behavioral sciences. New York, NY: Academic Press;; 1977. pp. 20–27. [Google Scholar]