

Abstract
Background:
Hirsutism is defined as the growth of terminal hair in a male pattern in women; it affects 5-15% of women.
Objective:
The aim of this study is evaluation of only the chin or lower abdomen for predicting hirsutism.
Materials and Methods:
In this cross-sectional diagnostic study, we randomly selected 695 women aged 15-45 years. The examiners scored the subjects on a scale of 0 - 4 for terminal hair growth on nine different body areas according to the Ferriman-Gallwey (FG) scoring system in a form given to the examiners before the examination. An FG score of 8 or more was considered diagnostic of hirsutism. If the sum of the FG scores for the chin or lower abdomen was 2 or more, the test result was assumed to be positive. Statistical analysis was performed using the MacNemar test, and a P value of less than 0.05 was considered to be statistically significant.
Results:
The age group with the highest prevalence rate was 21-25 years. From the 695 subjects examined, 81 subjects (11.7%) had an FG score of 8 or more with a resultant prevalence rate of 11.7% for hirsutism. In our study population, 39% of the patients had an FG score of 2 or more for the chin or lower abdomen, and 61% of the patients had an FG score of less than 2 for the chin or lower abdomen.
Conclusion:
Evaluating terminal hair growth on the chin or lower abdomen for predicting hirsutism seems to be an acceptable screening method.
Keywords: Evaluation, Ferriman-gallwey score, hirsutism
INTRODUCTION
Hirsutism is defined as the growth of terminal hair in a male pattern in women; it affects 5-15% of women. In most cases of hirsutism, hyperandrogenism is the underlying disease, and polycystic ovarian syndrome is the most common cause.[1,2,3,4,5,6,7,8,9,10,11,12,13] Most researchers determine the presence of hirsutism by using a modified version of the Ferriman-Gallwey (FG) scoring system. In this method, the FG score aids in subjectively evaluating the density of hair present on nine different body areas.[1,2,3,4,5,6,7,8,9,10,11,12,13] However, there are some problems with this method, i.e., (a) it is time consuming and (b) it requires patients to disrobe and thus is invasive of privacy. As a result, this method has had a significant negative impact on the completion of epidemiological or genetic studies performed on hirsutism. Thus, there is a need for a simpler and more applicable screening method for hirsutism. The results of previous studies show that the use of some other methods can resolve these problems. One of the methods proposed for screening is evaluation of either the chin or the lower abdomen for excessive terminal hair growth, but there is not enough evidence to support the use of this method.[14] Hence, we decided to compare the efficacy of this method with that of the standard FG scoring system in 695 women.
MATERIALS AND METHODS
In this cross-sectional diagnostic study, we randomly selected 695 women aged 15-45 years during 2001-2003 from the internal medicine ward of Khatam-al-Anbia hospital, Zahedan. The importance of hirsutism and the method to be used for examination was explained to the subjects, and the women who did not agree to be examined were excluded. The ethical review board of Zahedan University of Medical Sciences has approved the study proposal and informed consent was obtained from all subjects. Furthermore, the subjects who had taken any drug for hirsutism were also excluded.
All the subjects underwent examination by two different examiners (1 endocrinologist and 1 internal medicine resident) to reduce inter-individual variability. The examiners scored the subjects on a scale of 0 - 4 for terminal hair growth on nine different body areas according to the FG scoring system in a form given to the examiners before the examination. Any differences between the scores given bythe examiners resulted in the exclusion of that patient. The scores were transferred to a computerized database after the forms were coded. An FG score of 8 or more was considered diagnostic of hirsutism.[1,2,3,4,5,6,7,8,9,10,11,12,13] If the sum of the FG scores for the chin or lower abdomen was 2 or more, the test result was assumed to be positive.[14]
Statistical analysis was performed using the McNemar test, and a P value of less than 0.05 was considered to be statistically significant. The sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and the accuracy of the scoring system were calculated.
RESULTS
The prevalence of hirsutism among different age groups is shown in Figure 1. The age group with the highest prevalence rate was 21-25 years. From the 695 subjects examined, 81 subjects (11.7%) had an FG score of 8 or more with a resultant prevalence rate of 11.7% for hirsutism. In our study population, 39% of the women had an FG score of 2 or more for the chin or lower abdomen, and 61% of the women had an FG score of less than 2 for the chin or lower abdomen.
Figure 1.
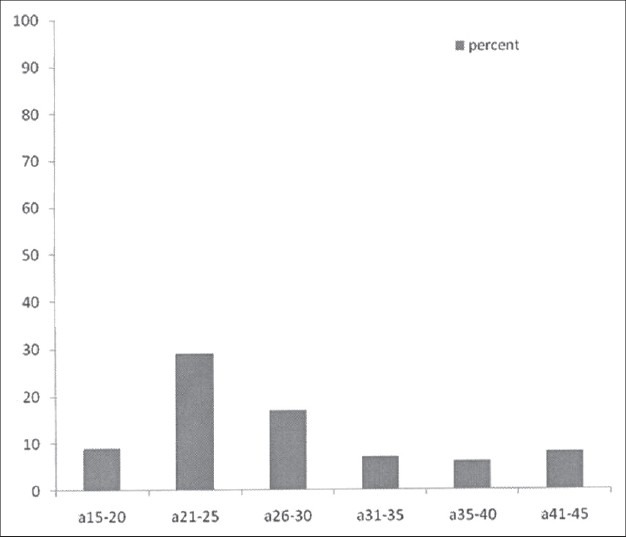
Prevalence rate of hirsutism among different age groups in women aged 15-45 years
Each of the 81 subjects with an FG score of 8 or more had an FG score of 2 or more for the chin or lower abdomen. From the 614 subjects with an FG score of less than 8, the FG score for the chin or lower abdomen was less than 2 in 424 subjects and was 2 or more in 190 subjects. There was no significant difference between total FG score 8 or more and FG score of 2 or more for the chin or lower abdomen after Mcnemar test (P = 0.44). Considering the FG scoring system to be the gold standard, the sensitivity and specificity of the chin or lower abdomen method was considered to be 100% and 69.1%, respectively. The PPV and NPV were 29.9% and 100%, respectively.
DISCUSSION
Our study shows that evaluation of terminal hair growth on the chin or lower abdomen has a high sensitivity for predicting hirsutism. In clinical settings, most examiners use a modified version of the FG score for predicting hirsutism. Because of being time-consuming and invasive of privacy, which has a negative impact on the compliance of patients participating in clinical studies and the resultant bias in estimating the prevalence of hirsutism, we decided to propose a simpler and more applicable method. We used evaluation of terminal hair growth on only the chin or lower abdomen as the method of examination to predict hirsutism in our study population. Our results showed 100% sensitivity, but the specificity and PPV were proportionally lower. Knochenhauer et al. Proposed evaluation of terminal hair growth on only the chin or lower abdomen for predicting hirsutism in women showing clinical features of this condition.[14] The sensitivity of this method in their study was the same as that in our study, but the specificity reported in their study was lower than that reported in our study.[14] This difference may be due to two factors: (1) We tried to eliminate inter-individual variability by using two different examiners, and (2) the prevalence rate of hirsutism in our study population was near normal as compared to that in the study performed by Knochenhauer et al., which evaluated only those patients who showed clinical features of hyperandrogenism. However, because of its very low PPV, this screening method is virtually useless in populations where the hirsutism frequency is expected to be low, about 5%.[14] In a similar study, Zhao et al. evaluated 11 sites on the body for hirsutism, of which the lip, chest, and lower abdomen were the main sites for determining the hirsutism status of women, with the latter 2 sites being more specific for hirsutism due to polycystic ovarian syndrome. They also proposed that the FG score for the forearm and leg may be indicative of the hirsutism status to some degree but is not specific and sensitive for hirsutism due to polycystic ovarian syndrome.[15] Cook et al. showed scoring terminal hair growth only on the chin and abdomen can serve as a reliable predictor of total body hirsutism.[16] The low specificity observed in our study and the study by Knochenhauer et al. can be attributed to the fact that terminal hair is more frequently distributed on the chin and lower abdomen than on the other body parts that are considered in the FG scoring system, as reported in previous studies on either normal populations or on hirsute women. Further, the normal hair distribution in androgen-sensitive areas shows normal variation across population, and hence, higher specificity values can probably be achieved for our method in such populations.[14,15,16,17,18,19]
In our study, the underlying causes of hirsutism were not analyzed further. The FG scores given by the endocrinologist and the internal medicine resident were considered to be the same. Furthermore, in order to devise a method with the intended characteristics, we need to compare the FG scores for terminal hair growth at other body sites–singly or in combination.
As seen in the results of previous studies, evaluating terminal hair growth on the chin or lower abdomen for predicting hirsutism seems to be an acceptable screening method. However, because of the low prevalence of hirsutism in our study, PPV is very low.
Future studies should include a hormone profile and analysis of other body sites-singly or in combination for predicting hirsutism.
Footnotes
Source of Support: Zahedan University of Medical Sciences, Zahedan, Iran
Conflict of Interest: None declared
REFERENCES
- 1.Ferriman D, Gallwey JD. Clinical assessment of body hair growth in women. J Clin Endocrinol Metab. 1961;21:1440–7. doi: 10.1210/jcem-21-11-1440. [DOI] [PubMed] [Google Scholar]
- 2.McKnight E. The prevalence of “hirsutism” in young women. Lancet. 1964;1:410–3. doi: 10.1016/s0140-6736(64)92789-8. [DOI] [PubMed] [Google Scholar]
- 3.Hatch R, Rosenfield RL, Kim MH, Tredway D. Hirsutism: Implications, etiology, and management. Am J Obstet Gynecol. 1981;140:815–30. doi: 10.1016/0002-9378(81)90746-8. [DOI] [PubMed] [Google Scholar]
- 4.Kirschner MA. Hirsutism and virilism in women. Spec Top Endocrinol Metab. 1984;6:55–93. [PubMed] [Google Scholar]
- 5.Derksen J, Moolenaar AJ, Van Seters AP, Kock DF. Semiquantitative assessment of hirsutism in Dutch women. Br J Dermatol. 1993;128:259–63. doi: 10.1111/j.1365-2133.1993.tb00168.x. [DOI] [PubMed] [Google Scholar]
- 6.Claman P, Graves GR, Kredentser JV, Sagle MA, Tan S, Tummon I, et al. Reproductive endocrinology infertility committee and executive committee and council, society of obstetricians and gynaecologists of Canada. SOGC clinical practice guidelines. Hirsutism: Evaluation and treatment. (77-9).J ObstetGynaecol Can. 2002;24:62–73. [PubMed] [Google Scholar]
- 7.Azziz R. The evaluation and management of hirsutism. Obstet Gynecol. 2003;101(5 Pt 1):995–1007. doi: 10.1016/s0029-7844(02)02725-4. [DOI] [PubMed] [Google Scholar]
- 8.Rosenfield RL. Clinical practice.Hirsutism. N Engl J Med. 2005;353:2578–88. doi: 10.1056/NEJMcp033496. [DOI] [PubMed] [Google Scholar]
- 9.Essah PA, Wickham EP, 3rd, Nunley JR, Nestler JE. Dermatology of androgen-related disorders. Clin Dermatol. 2006;24:289–98. doi: 10.1016/j.clindermatol.2006.04.004. [DOI] [PubMed] [Google Scholar]
- 10.Watts J. Understanding the causes and management of hirsutism. Nurs Times. 2006;102:26–8. [PubMed] [Google Scholar]
- 11.Lowenstein EJ. Diagnosis and management of the dermatologic manifestations of the polycystic ovary syndrome. Dermatol Ther. 2006;19:210–23. doi: 10.1111/j.1529-8019.2006.00077.x. [DOI] [PubMed] [Google Scholar]
- 12.Lee AT, Zane LT. Dermatologic manifestations of polycystic ovary syndrome. Am J Clin Dermatol. 2007;8:201–19. doi: 10.2165/00128071-200708040-00003. [DOI] [PubMed] [Google Scholar]
- 13.Bona G, Bozzola M, Buzi F, De Sanctis C, De Sanctis V, Radetti G, et al. Hirsutism. Minerva Pediatr. 2007;59:289–98. [PubMed] [Google Scholar]
- 14.Knochenhauer ES, Hines G, Conway-Myers BA, Azziz R. Examination of the chin or lower abdomen only for the prediction of hirsutism. Fertil Steril. 2000;74:980–3. doi: 10.1016/s0015-0282(00)01602-2. [DOI] [PubMed] [Google Scholar]
- 15.Zhao JL, Chen ZJ, Shi YH, Geng L, Ma ZX, Li Y, et al. Investigation of body hair assessment of Chinese women in Shandong region and its preliminary application in polycystic ovary syndrome patients. Zhonghua Fu Chan KeZaZhi. 2007;42:590–4. [PubMed] [Google Scholar]
- 16.Cook H, Brennan K, Azziz R. Reanalyzing the modified Ferriman-Gallwey score: Is there a simpler method for assessing the extent of hirsutism? Fertil Steril. 2011;96:1266–70. doi: 10.1016/j.fertnstert.2011.08.022. e1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Téllez R, Frenkel J. Clinical evaluation of body hair in healthy women. Rev Med Chil. 1995;123:1349–54. [PubMed] [Google Scholar]
- 18.Hines G, Moran C, Huerta R, Folgman K, Azziz R. Facial and abdominal hair growth in hirsutism: A computerized evaluation. J Am Acad Dermatol. 2001;45:846–50. doi: 10.1067/mjd.2001.117386. [DOI] [PubMed] [Google Scholar]
- 19.DeUgarte CM, Woods KS, Bartolucci AA, Azziz R. Degree of facial and body terminal hair growth in unselected black and white women: Toward a population definition of hirsutism. J Clin Endocrinol Metab. 2006;91:1345–50. doi: 10.1210/jc.2004-2301. [DOI] [PubMed] [Google Scholar]