An official website of the United States government
Here's how you know
Official websites use .gov
A
.gov website belongs to an official
government organization in the United States.
Secure .gov websites use HTTPS
A lock (
) or https:// means you've safely
connected to the .gov website. Share sensitive
information only on official, secure websites.
Some NLM-NCBI services and products are experiencing heavy traffic, which may affect performance and availability. We apologize for the inconvenience and appreciate your patience. For assistance, please contact our Help Desk at info@ncbi.nlm.nih.gov.
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with,
the contents by NLM or the National Institutes of Health.
Learn more:
PMC Disclaimer
|
PMC Copyright Notice
Address for Correspondence: Dr. Meeta, Tanvir Hospital, Plot No. 100, Phase-I, Kamalapuri Colony, Hyderabad - 500 073, India. E-mail: drmeeta919@gmail.com
*
This is a summary and recommendations from the detailed document on Clinical Practice Guidelines on Menopause published by Jaypees. (R-indicates Recommendation with Grading, the detailed references is listed in the main document. The text of the unpublished references can be procured from Dr. Meeta at drmeeta919@gmail.com)
This is an open-access article distributed under the terms of the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
For review on vitamin D: Michael F Holick, Professor of Medicine, Physiology and Biophysics and Molecular Medicine. Director, Vitamin D, Skin, and Bone Research Laboratory. Programme Director General Clinical Research Unit. Director, Biologic Effects of Light Research Centre, Director, Bone Healthcare, Boston.
External Review Board: A Muruganathan, Anil K Jain, Dinesh K Dhanwal, G R Sridhar, Hema Divakar, K V Radha Krishna, Prof Nihal Thomas, N S Neki, P K Shah, S K S Marya, Sandhya Kamath, Sarita Bajaj, Thomas Paul.
Advisory Board: Asha Kapadia, Atul Munshi, Duru Shah, Rama Vaidya, Saroj Srivastava, Sonia Malik, Sunila Khandelwal, Urvashi Prasad Jha. External Review Board: A Muruganathan, Anil K Jain, Dinesh K Dhanwal, G R Sridhar, Hema Divakar, K V Radha Krishna, Prof Nihal Thomas, N S Neki, P K Shah, S K S Marya, Sandhya Kamath, Sarita Bajaj, Thomas Paul.
Guidelines are a method of translating the best available evidence into clinical, communicable, organizational, and policy making statements in the hope of improving health care and or policies. Do we need country specific guidelines? Yes, we do. Given the fact that the model of health-care delivery system and the prevailing environment of one country may not be extrapolated to that of another.
“Working with what you have, where you are and not with what you wish for” – is the principle each one of us follow in the clinical practice to give the best to our patients. This guideline hopes to bridge the gap between evidence based practice, backed by scientific evidence and experience based practice based on the published and unpublished Indian data and expert opinions. Unlike protocols, guidelines are meant to aid the clinician in decision making. The target readers of this guideline are the adult women, members of the Indian Menopause Society (IMS), allied professionals, health-care providers, and policy makers.
India is a land of rich and diverse cultural heritage. It is a land of diversity in terms of, socioeconomic, religion, culture, beliefs, education, nutrition urban, rural, and geographical regions. The dilemmas and challenges are unique to different regions and solutions need to be planned accordingly. The specific issues pertaining to Indian women are an early age of natural menopause, genetic and environmental influences, nutritional deficiencies, and excesses resulting in physiologic differences. These factors contribute significantly to an increased incidence of diabetes, cardiovascular disease, osteoporosis, and thyroid dysfunction. Genetic components are likely to play a prominent role in these disorders for example, polymorphisms in estrogen receptors alpha and vitamin D receptor has been implicated in the pathogenesis of osteoporosis. The burden of morbidity from osteoporosis has significant medical, social, and financial implications. Osteoporotic fractures are preventable, yet diagnosed only after the event; a situation similar to the diagnosis of hypertension after myocardial infarction or stroke. It has a long incubation period and cost- effective treatment strategies currently available for this disease mandate that osteoporosis be diagnosed and treated early.
OBJECTIVES
To recognize post-menopausal osteoporosis (PMO) as a major health issue among health-care professionals, policy makers, and the public.
To assist health-care practitioners in providing optimal care to post-menopausal women with the available resources. Osteoporosis is a costly debilitating disease, hence it is important to instill preventive measures, diagnose early, encourage modifications of risk factors associated with osteoporosis. Counseling on nutritional factors, abuse of tobacco, heavy alcohol consumption, and on life-style should be mandatory. Treat with pharmacologic agents only when indicated.
To fill the lacunae of medical care after managing fragility fracture.
To aid primary care physicians to decide when to refer patients with difficult problems to the relevant specialists.
To stimulate interest in research on osteoporosis.
METHODS
The planning to publishing of the document took 24 months. The core committee was formed and a broad based multi-disciplinary list of experts were invited to write on the topic of their expertise. Majority of the reviews and deliberations wear by E-mail. A two day intensive contact program of the contributors was convened at Hyderabad on December 8th and 9th 2012. Each topic was presented and deliberated upon, and the consensus obtained by an automated response system. Later one day contact meeting of the Editorial Board was convened on January 11th, 2013. Finally, the document was validated by an External Review Board.
Data were sourced from the electronic database PubMed, MEDLINE, Cochrane Database of Systematic Reviews and published guidelines on PMO management. The appraisal of Guidelines Research and Evaluation,[1] instrument was used to appraise published guidelines. Abstracts from papers and posters presented at the National Indian Menopause Society Meetings, published and unpublished studies, expert opinion was considered. Cost-effectiveness of diagnosis and treatment is based on the available market value.
SYSTEM FOR GRADING: EVIDENCE USED IN THE DOCUMENT
The quality of evidence and the level of recommendation was carried out using the grades of recommendation, assessment, development, and evaluation (GRADE),[2] system.
Recommendations are based on strong evidence, suggestions on experience based evidence, this method is adapted to unite the diverse conditions of India with the best available data and the rich experience based evidence from the experts.
GRADE: Grades of evidence:
High quality – GRADE A: Further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality – GRADE B: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality – GRADE C: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality – GRADE D: We are very uncertain about the estimate.
In terms of the strength of the recommendation, strong recommendations use the phrase “recommend,” and weak recommendations use the phrase “suggest.”
Research questions are placed at the end of each chapter in the monogram of the book.
BENEFITS OF USING THE GUIDELINE
Benefits of using these guidelines are: (i) Improved early identification and better management of women at risk for fragility fractures; (ii) down grading the disease burden after an episode of fragility fracture by improving the assessment, management and follow-up of these women; (iii) understanding the urgent need of conducting preventive health programs by all stake holders related to women’s health; and (iv) in addition, in view of the paucity of Indian data it is hoped that this guideline will help stimulate interest in research in various aspects of PMO.
CONCLUSIONS
Osteoporosis has significant medical, social, and financial implications.
The onus is on the Government and Non-Government Organizations to develop specialty menopause and osteoporosis clinics akin to antenatal clinics in the private and public sectors besides developing management of menopause as a medical specialty within obstetrics and gynecology care. The aim of the guideline is to provide a resource documentss to aid the busy clinician to give optimal care to the ageing woman. Limitations are the paucity of robust research evidence in India. This is one of the endeavors of the Indian Menopause Society to work toward the slogan “Fit @ Forty, Strong @ Sixty, Independent @ Eighty”.
ACKNOWLEDGEMENTS
We thank the experts who took time out of their busy family life, academics, and work to contribute to the document on PMO in India. A special thanks to Dr. Hemant Zaveri for sourcing the data.
DISSEMINATION OF THE GUIDELINES
A free copy of the guideline is for the members of the IMS and Jaypee Publishers are making the monogram available widely for purchase by the health-care providers and policy makers. The Guideline is available on the IMS website www.indianmenopausesociety.org.com and is published in the Journal of Midlife, official publication of the IMS.
REVISION OF THE GUIDELINES
It is recommended that the guidelines are upgraded every 2 years.
EDITORIAL INDEPENENCE
The views expressed are independent of any extraneous influences.
REFERENCES
1.AGREE Next Steps Consortium, 2009. The AGREE II Instrument [Electronic version]. [Last accessed on 2012 Feb 10]. Available from: http://www.agreetrust.org .
2.Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of
recommendations. BMJ. 2004;328:1490. doi: 10.1136/bmj.328.7454.1490. [DOI] [PMC free article] [PubMed] [Google Scholar]
Among the several challenges faced by the growing elderly population with increasing longevity in India, post-menopausal osteoporosis (PMO) is emerging as one of the major public health issues. Osteoporosis is an asymptomatic or “silent” disease and generally presents as a fragility fracture. Typical osteoporotic fractures are those of the hip, spine and wrist. Global data indicates that 20% of women with hip fracture die within 1 year of the fracture and 50% of them never regain their functional independence.[1] Vertebral fractures can also have significant morbidity and are associated with increased long-term mortality.[2] World Health Organization (WHO) has identified osteoporosis as an important non-communicable disease. Osteoporotic fractures impose great financial, medical, and social burden on society. These guidelines are intended to be used as a resource document by the health-care providers involved in post-menopausal women’s health at all levels of health-care with specific reference to India. Though framed for India, it is hoped that these guidelines will be useful for menopause practitioners across the globe.
BASICS CONCEPTS
Definition
1. WHO defines osteoporosis as “a systemic skeletal disease characterized by low bone mass (measured as bone mineral density – [BMD]) and micro architectural deterioration of bone tissue with a consequent increase in bone fragility and susceptibility to fractures involving the wrist, spine, hip, pelvis, ribs or humerus.[3] The National Institute of Health definition is “a disease characterized by decreased bone strength and propensity to fall.”[4]
Diagnosis
2. The diagnosis of an osteoporotic fracture, the clinical end point of osteoporosis is by the presence of fragility fracture (clinical or radiological) and or by BMD.
3. The “gold standard” method of BMD testing is by dual X-ray absorptiometry (DXA). Its value is expressed in standard deviation (SD) units from the population mean in young adults (T-score) or from the mean in an age-matched population (Z score).
4. The reference range recommended by the International Osteoporosis Foundation (IOF), International Society of Clinical Densitometry WHO and National Osteoporosis Foundation (NOF) for calculating the T-score in post-menopausal women is the National Health and Nutrition Examination Survey (NHANES) III reference database in Caucasian women aged 20-29 years.[4,5,6]
5. BMD based criteria for diagnosis of osteoporosis by different organizations is based on a common principle:
In 1994, WHO definition was based on the T-score of the lumbar spine, total hip, or femoral neck.
Currently WHO/IOF define osteoporosis as a value for BMD 2.5 SD or more assessed at the femoral neck and is below the young female adult mean (T-score ≤ −2.5 SD).[4,5] Population based sampling and expressing fracture risk as a function of BMD with age adjustment have shown that the risk of hip/vertebral fracture is similar in men and women for a given absolute value of BMD and therefore the diagnostic criteria for defining osteoporosis in men is the same as in women.[7,8] Hence, the femoral neck BMD is used for diagnosis of osteoporosis. It needs to understand that the T-score cannot be used interchangeably with different techniques and at different sites since the prevalence of osteoporosis and proportion of individuals allocated to any diagnostic category would vary as does the risk of fracture. Due to the above reasons, the WHO uses the femoral neck as the reference site, but this does not mean that other techniques or other sites cannot be used in the clinical management. Further, it should be recognized that the information derived from the T-score may differ from that provided by BMD at the femoral neck.
The NOF diagnosis is based on T-score of femoral neck and spine.[5]
The International Society for Clinical Densitometry diagnostic criteria for osteoporosis in post-menopausal women and in men age 50 and older is if the T-score of the lumbar spine, total hip, or femoral neck is −2.5 or less. In certain circumstances, the 33% radius (also called 1/3 radius) may be utilized.[9]
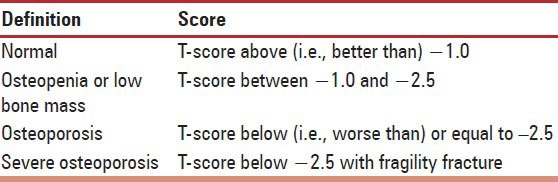
6. BMD (T-score)-based diagnosis of osteoporosis for post-menopausal women [Table 1].
7. The Z-score describes the number of SDs by which the BMD in an individual differs from the mean value expected for that age and sex. It is mostly used in children, adolescents, and premenopausal women. A Z-score below –2 is regarded as abnormal and should be referred to as “low for age.” A low Z score in a post-menopausal woman indicates the need to evaluate for secondary osteoporosis.
8. Limitations of present definitions of osteoporosis
The WHO criteria for diagnosis of osteoporosis are derived from Caucasian post-menopausal women population and are thus best applicable to that group. However, in the absence of normative data from other races, WHO criteria have been widely accepted and used in the clinical practice. Normative data for Indians is emerging.[10,11,12,13,14,15,16,17] Presently in India, the reference range of the DXA machines are based on the database of the NHANES III reference range. It is possible that by applying these criteria, substantial number of patients may be over diagnosed and over treated. Thus, it is imperative that population-based normative data and reference range for Indians is established and incorporated in the DXA machines. Though, the present diagnostic threshold is −2.5, it is advisable to set the intervention threshold at −3 to prevent overtreatment. (GRADE C).
BMD is a good surrogate marker of bone strength and fracture risk. But BMD measurement lacks the sensitivity (±50%) to identify those at risk of fracture; hence treatment strategies cannot be based only on T-scores (GRADE A).
BMD measurements are quite specific (85%). The mortality adjusted lifetime risk of fracture for women with a T-score less than and equal to −2.5 is 65% (95% confidence interval).
Although WHO classification has provided a practical basis for identifying the approximately 30% of post-menopausal Caucasian women at risk of sustaining a fracture, but we need to understand that it is one of the quantifiable risk factors for fracture among others. A single BMD measurement lacks sensitivity since less than 50% of patients with a known osteoporotic fracture have a BMD value that is within the osteoporosis range that is T-score below −2.5. However, a low BMD is perhaps the only quantitative risk factor, which characterizes osteoporosis predisposing to clinical fracture, similar to other diseases, e.g., diabetes and hypertension, which are characterized by quantitative risk factors (GRADE A).
The WHO diagnostic criteria have been validated using DXA of the axial skeleton, that is, the spine and hip, extrapolation of these criteria to other techniques (e.g., ultrasound, computed tomography) used to measure BMD, including the peripheral skeleton may yield incorrect information regarding fracture risk. T-scores cannot, therefore, be used interchangeably between the different techniques available to measure BMD.
The exclusively BMD-based diagnostic approach of the WHO classification does not include extra-skeletal risk factors like the propensity to fall.
The emergence of largely BMD-independent risk factors contributing to fragility fractures, the BMD-based criteria alone will not be sensitive enough to identify those at risk of a fracture. This has underscored the need for fracture risk assessment tools or algorithms to manage patients with osteopenia and osteoporosis. It is important that we understand that we should not be treating T-scores only (GRADE C).
Bone quality, an important component of bone strength is not considered in the WHO definition. A low bone mass is most commonly the result of osteoporosis, it may be reflected secondary to osteomalacia and primary hyperparathyroidism, which are simpler to treat than advanced osteoporosis.
Falsely high BMD may be due to flurosis, which is prevalent in some parts of the country.[18]
TYPES OF OSTEOPOROSIS
9. Osteoporosis was earlier classified as primary and secondary.(experts feel that this classification is no longer valid):
Primary osteoporosis is seen in post-menopausal women in whom there is no specific pathogenetic mechanism other than age.
There is an accelerated bone loss at the rate of 2-5%/year due to declining estrogens levels and is seen in the first 5-7 years after menopause.[19]
Secondary osteoporosis is due to specific causes.
10. Osteoporosis and osteomalacia
Bone is a dynamic tissue with a continuous remodeling leading to the formation of new bone and resorption of old bone. A mismatch of this process forms the basis for osteoporosis while defective mineralization of the newly formed osteoid is called osteomalacia.
11. Fragility fracture
A fragility fracture has been defined by the WHO as “a fracture caused by injury, which would be insufficient to fracture normal bone: The result of reduced compressive and/or torsional strength of bone”.
Clinically, a fragility fracture can be defined as one, which occurs as a result of minimal trauma, such as a fall from a standing height or less, or no identifiable trauma.
The most common sites of fragility fracture are the hip, spine, and forearm. The other sites are pelvis, proximal femur, proximal humerus, proximal tibia, and fractures involving three ribs simultaneously.
Fragility fractures account for 80% of fractures in post-menopausal women.[20]
Risk of recurrence of a hip fracture is 5-10%, and with vertebral fracture, it is 20% within a year following a primary fracture.[21,22]
Fragility fracture leads to significant impairment of physical, social, and mental health, with a drain on emotions and economics.
12. Fragility
Fried et al.,[23] have standardized the definition as three or more of the following five criteria: Unintentional weight loss, self-reported exhaustion, weakness (grip strength), slow motor performance (walking speed), and low physical activity.
EPIDEMIOLOGY
13. Preliminary data from India (published and unpublished) indicate a high prevalence rate of PMO making it a major public health problem. This also underscores the need for population-based studies for prevalence, and incidence of new hip fractures and related mortality.
14. Though the prevalence of PMO in population above the age of 50 years varies widely across the globe 5.8-50.1%,[24] the limited data from India reveal the prevalence to be ranging from 25.8 to 62. This reflects the need for using a standard site, method and reference standards for diagnosis of PMO based on BMD and is prudent to use the current WHO based criteria. Further, stratification of the risk based on age shows that the prevalence of low bone mass is more than 40% from the age of 40 years and increases to more than 62% by age 60 and 80% by the age of 65 years.[25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46]
15. Community-based epidemiological data on fractures are lacking. Hospital-based studies show that hip fractures are more common in women and with an average age between 60 years and 70 years.[42] The exact hip fracture incidence remains a challenge to investigators, but data from expatriate Indians, places their incidence somewhat lower than white Caucasians and Chinese, and higher than Malays.[42,44,45] A longitudinal follow-up study of urban women (n = 450) over a 3 year period revealed that 7 women who had sustained an atraumatic fracture had osteoporosis at either the hip or the spine (unpublished data, Shah and Savardekar).
16. X-rays revealed vertebral fractures in 17% (urban) 23.8% (rural) of women between 55 years and 59 years and 22% (urban)-38% (rural) in women above 65 years.[38] Recent data suggest that Indians have similar vertebral fracture risk as western and other Asian populations Delhi Vertebral Osteoporosis Study. (DeVOS).[46]
17. High prevalence of PMO in Indian women may be due to inadequate nutrition, i.e., protein, vitamin D3,[47,48,49,50] and calcium, sedentary life-style, and early menopause.[51]
18. There is wide prevalence of low dietary calcium intake in Indians of all age groups with the majority of post-menopausal women consuming < 400 mg/day.[10,28,48] This extends to all the other age groups (infancy, adult hood, post-menopausal women, pregnancy, and lactation).
19. Studies on bone mineral health from different parts of India indicate wide prevalence of vitamin D deficiency in all age groups, including neonates, infants, school children, pregnant/lactating women, adults, and post-menopausal women.[40,42,44,47,48,49,50,52,53,54,55,56,57,58,59,60]
20. The result of Indian multi-centric study in middle aged health-care professional found that 79% of subjects were vitamin D deficient, 15% had insufficient levels of 25-hydroxy vitamin D (25(OH) D), and just 6% of health professionals were adequate in vitamin D status. The mean concentration of 25(OH) D was 14.65 ± 10.32 ng/mL (median 11.93 ng/mL)[61] This study confirms the results from a single center smaller studies carried out earlier amongst the health professionals in India.[62,63] A review of the global vitamin D status by the IOF in 2009 underscores the fact that South Asia may be one of the worst affected regions in the world.[43]
21. Recent data indicate that Indians have lower bone density than their North American and European counterparts.[15,16,28,64,65,66,67,68,69]
22. It is reported that osteoporotic fractures occur 10-20 years earlier in Indians compared to Caucasians.[28,64] The probable reasons cited are genetic, environmental, and nutritional.
23. Nutritional factors probably play a major role as shown in the ICMR (Indian Council of Medical Research) studies on three socio-economic groups at the National Institute of Nutrition. They showed that after the age of 50 years, osteoporosis of the spine was only 16% in the high income group (with calcium intake of 1000 mg) compared to the low income group with 65% osteoporosis (calcium intake around 400 mg).[10] The major limitation of this study was it was confined only to four major cities in India and only up to Hyderabad (latitude 17°22’N) (latitudinal extent of India 8°4’N to 37°6’N). India has a vast cultural, ethnic, dietary, and dress code variations and it is imperative to include all sections of the population in length and breadth of the country.
24. Parallel to a decrease in the calcium intake, bone densities were also lower with a decreasing income. Those above 50 years suffered from much worse bone densities than those less than 50 years in the same group.[10] The fracture rate at the neck of the femur was shown to occur 12-15 years earlier in women from low income group as compared to that in high income group.[70] Dhanwal et al., have reported that hip fracture patients in India have vitamin D deficiency and secondary hyperparathyroidism.[71]
25. Marwaha et al., have evaluated the impact of life-style on BMD and osteoporosis in Indian Jawans and Indian sportswomen, and highlighted that good nutrition, better bone biochemical parameters, adequate sun exposure, and physical activity from younger age helped to attain better peak bone mass (PBM) when compared to their age matched sedentary controls.[14,72,73]
26. Early menopause in Indian women in comparison with their Caucasian counterparts may assume significance in causation of PMO in Indian context since there is an inverse correlation between and number of years since menopause and BMD.
27. This brings to attention the urgent need for the Government and Non-Government Organizations to promote community and school-based educational programs on nutrition, physical, and outdoor activities, to tackle these modifiable risk factors for osteoporosis.
PEAK BONE MASS
28. PBM is the highest level of bone mass achieved as a result of normal growth and is important as it determines resistance or susceptibility to osteoporosis and fractures. PBM is the result of the interaction of various factors: Genetic, hormonal, racial, nutritional, life-style, and physical exercise. Environmental factors modulate the expression of the genetic potential to achieve PBM.
29. Age, sex, and genetic predisposition are important non-modifiable risk factors for osteoporosis.
30. Acquisition of PBM and the rate of subsequent bone loss and formation are modulated by important modifiable environmental risk factors. Poor nutritional intake of protein, calcium and vitamin D from infancy to late adult life leads to low PBM and risk of osteoporosis and early post-menopausal fractures.[74]
31. Maternal nutrition and in utero influences have the potential to influence skeletal development through in utero programming of several hormones. Recent data on vitamin D status in pregnant and lactating Indian women from Delhi, Lucknow, and Mumbai reveal a very high prevalence of hypovitaminosis D (84-93%). One study suggested that supplementation with vitamin D during the pregnancy could result in better anthropometric indices in the newborns up to 9 months of follow-up.[75]
Hence, optimization of maternal nutrition and intrauterine growth should ideally be included in the preventive strategies for osteoporotic fracture.[76,77,78] There is an evidence to support the role of poor maternal nutrition (calcium and vitamin D) on the neonatal bone mineral content and its consequences on adult bone mass, skeletal size, and fracture risk. It is suggested to initiate the management of PMO from in utero.[75,79,80,81]
32. Although PBM is achieved by 25-30 years, 40-50% of bone mass is accumulated during pubertal years and 80% is achieved by the age of 18 years. At skeletal maturity women have 10-15% lower bone mass than men. Asian Indians have a significantly lower PBM than Caucasians.
33. Calcium intake seems to be a main nutritional determinant in bone mass acquisition. In children and adolescents in whom calcium intake is deficient, calcium supplementation according to adequate intake for age is recommended (GRADE B).
34. Vitamin D has a major role in stimulating intestinal calcium absorption. In children and adolescents having an insufficient vitamin D status, vitamin D supplementation according to adequate intake for age is recommended (GRADE B).
35. Physical exercise (mainly regular weight bearing activity) is a key factor for the acquisition and maintenance of bone mass. Children and adolescents need good nutrition and encouragement to undertake outdoor physical activities (GRADE B).
SCREENING AND DIAGNOSIS
36. Osteoporosis is asymptomatic unless a fracture occurs. Early diagnosis in the asymptomatic period is essential, and timely management of osteoporosis will prevent the associated morbidity and mortality. Screening is the early diagnosis of a pre-symptomatic disease among well individuals in the general population. Osteoporosis screening of large scale whole population groups is not likely to be cost-effective, so more selective approaches, i.e., targeted screening for disease detection is advocated. In the absence of a validated population screening tool for PMO in India, a case finding strategy utilizing clinical risk factors with the addition of DXA as needed is suggested (GRADE C).
37. Asymptomatic women: Opportunistic screening for women above 40 years is suggested:
Risk assessment factors for fractures are derived by history and clinical examination. It is important to distinguish between those risk factors, which lead to reduced bone mass from those which predispose to osteoporotic fractures with a BMD not in the osteoporotic range.
Major risk factors defined by WHO are (GRADE A):
Age: Advancing age is a single most significant risk factor.
Low body mass index (BMI). Although low BMI is a significant risk factor for hip fracture, but the value of BMI in predicting other fractures is much reduced when adjusted for BMD.
Prior history of a fracture: Doubles the risk of for further fracture. This is observed more markedly for a vertebral fracture following a previous spine fracture. The risks are in part independent of BMD.
Parental history of hip fracture: Is a significant risk factor that is largely independent of BMD.
Smoking: Is a risk factor that is in part dependent on BMD.
Glucocorticoid: The fracture risk by the use of glucocorticoid is not only dependent upon bone loss, but other BMD independent risks have been identified.
Alcohol: Alcohol intake and fracture risk is dose-dependent. Consumption of 3 or more Units daily are associated with a dose-dependent increase in fracture risk.
Rheumatoid arthritis. There are many secondary causes of osteoporosis (e.g., inflammatory bowel disease, endocrine disorders), but in most instances it is uncertain to what extent this is dependent on low BMD or other risk factors such as the use of glucocorticoids. Rheumatoid arthritis increases fracture risk independently of BMD.
Environmental factors: include nutrition (calcium intake using the quick dietary calculator, protein), physical activity, and sunlight exposure, which are important modifiable risk factors in India. Relevance of risk of falling increases with ageing (GRADE B).
38. Secondary osteoporosis: Case finding for secondary osteoporosis is practiced in high-risk disease subgroups, such as chronic glucocorticoid users and patients with rheumatoid arthritis, collagen vascular disease, or inflammatory bowel disease, hypogonadism, thyroid dysfunction, type 2 diabetes (GRADE A).
39. Symptomatic woman
Women presenting with fracture complain of severe pain, which is sudden in onset with minimal trauma, or chronic pain localized to the mid back, may radiate to the abdomen.
Generalized bone pain indicates osteomalacia or metastasis.
If needed a multifactorial fall assessment is recommended.
In vitamin D deficiency, proximal muscle is affected more than the distal so activity, such as using a squatting toilet, climbing stairs, and getting out of low chair can be particularly difficult. Tenderness on the pretibial and sternum can be elicited.
40. Physical examination
Should include recording the height and weight annually, checking for balance and gait, get up, and go test by asking the women to get up from the chair without using their arms.
The occiput to wall distance in a standing position is ideally zero: Inability to touch the occiput to wall while standing implies a thoracic fracture.
Inability to insinuate the four fingers of the hand between the lower rib cage and anterior superior iliac crest implies a lumbar fracture.
Kyphosis and Dowager’s hump are seen in the late stage of osteoporosis (GRADE A).
PTH (based on clinical judgment). Parathyroid Hormone.
42. The FRAX (WHO fracture risk assessment tool): (this is the expanded one).
For online use is available for India (http: www.shef.ac.uk/FRAX). FRAX is a validated and widely accepted tool used worldwide to identify patients in the osteopenia group most likely to benefit from treatment. It predicts the 10-year absolute risk for a fracture in an individual and the cost-effective analysis determines the interventional threshold above which treatment is cost-effective. All this is possible and valid when adequate data on the prevalence of osteoporotic fractures, mortality rates, and health economics data are available for the country. FRAX is country specific, and until more Indian data is available on the prevalence of osteoporotic fractures and mortality rates, the usage of FRAX in the Indian context for uniform guidance on intervention threshold is to be applied cautiously. Having said that an enormous advantage of FRAX is that it can be used without BMD also to identify cases at risk for fractures. In view of the limited availability of DXA dual X-ray absorptiometry machines in India, it will be helpful to use FRAX without BMD in Indian context. Given the heterogenecity of Indian scenario, intervention thresholds, and management may need to be individualized (GRADE C).
43. Heterogeneity in different regions of the country and the prevalence of nutritional and other risk factors unique to the Indian population has not been considered in the calculation of FRAX. Moreover, the diversity of the Indian population, make it difficult to develop a universally acceptable FRAX model for India (GRADE B).
44. It is suggested to conduct central DXA of the spine and hip in all women 5 years beyond the natural age of menopause and in women less than 5 years since menopause with one high clinical risk or more than two clinical risk factors. This suggestion is based on the following (GRADE C):
Early age of natural menopause that is 46.7 years in Indian women.[51]
Average life expectancy of a woman in India is 68 years (WHO statistics 2011).
Accelerated bone loss in the immediate 5 years of menopause and the trabecular bone is affected more.[4,42,40,68]
Stratification by age shows that the prevalence of low bone mass is more than 40% from the age of 40 years and increases to more than 80% by the age of 65 years.[25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46]
DXA
45. Indications for DXA (GRADE B)
All post-menopausal women more than 5 years of menopause.
Post-menopausal women less than 5 years of menopause with risk factors.
Women in menopause transition with secondary causes.
Radiological evidence of osteopenia and presence of vertebral compression fracture.
Women with fragility fractures.
Ideally before initiating pharmacotherapy for osteoporosis.
Emerging indications are to measure total body fat and lean tissue mass.
46. To monitor therapy the interval to the next DXA should depend on the calculated individual risk and would mostly be scheduled between 1 years and 5 years later.
47. The diagnosis is based on central DXA of the spine, total hip, and neck of femur. If this is not feasible lower one-third of the radius (33%) is measured. The Caucasian female normative database is used as a reference for T-scores (GRADE A).
48. The lowest BMD score obtained from all sites is used for diagnosis (GRADE A).
49. Screen post-menopausal women for secondary osteoporosis if history or examination shows systemic disease or low Z scores on DXA (GRADE A).
50. Peripheral DXA (X-ray based) may be used as a mass screening tool because of its high negative predictive value (GRADE C).
RADIOGRAPHY
51. X-ray abnormality is a feature of advanced bone disease. We recommend X-rays in all the diagnostic protocols for osteoporosis (GRADE A).
52. Vertebral Fractures are mostly clinically silent, but their presence pre-disposes a person to further fragility fractures of vertebra or even hip. Diagnosis of a vertebral fracture; therefore, on lateral X-ray of the spine is clinically important, ideally using a standard semi-quantitative method. Radiographic techniques are easily available and we recommended their usefulness in epidemiological screening (GRADE B).
53. Radiographic techniques cannot be used in monitoring drug therapy (GRADE A).
54. Adequate care should be taken while utilizing radiographic techniques since numerous physical factors, such as inconsistencies in beam quality, instability of the X-ray source, film response, processing conditions, radiation scattering conditions, and beam hardening effects may influence the radiographic image and have an adverse effect on precision and accuracy of the method (GRADE A).
QUANTITATIVE ULTRASOUND
55. WHO’s diagnostic criteria of − 2.5 SD below PBM does not apply for non-DXA techniques (GRADE A).
56. In the absence of calibrated ultrasound machines, it is not recommended for population screening (GRADE A). In areas of endemic fluorosis, (rampant in several parts of India) it is not advisable to follow ultrasound based bone densitometry for diagnosis of osteoporosis.[18]
(QCT) Quantitative Computed Tomography AND MAGNETIC RESONANCE IMAGING (MRI)
57. QCT and magnetic resonance imaging (MRI) give an additional advantage of 3D structural assessment of bone tissue (GRADE A).
BONE MARKERS
58. Normal values are reference values established in healthy pre-menopausal women aged 30-45 years.
59. Bone turnover markers are not a part of the routine tests to be used for clinical diagnosis (GRADE B).
60. However, if it is used to assess compliance and efficacy of therapy and preferably follow the broad guidelines given below (GRADE B):
Type of marker
Bone resorption: Serum CTX Carboxy-terminal cross linked telopeptide of type i collagen or urine CTX.
Bone formation: PINP N-terminal propeptide of type 1 procollagen, venous thromboembolism (VTE) and CVD Cardiovascular events.
Use one marker of bone resorption and one marker of bone formation. More specifically, markers for bone resorption when on anti-resorptives and bone formation markers when on anabolic agents.
Timing of sample
Serum: Morning (before 9 am) after an over-night fast.
Urine: Either first or second morning void, with creatinine correction after an overnight fast.
Try to use the same laboratory services and same assay or method for monitoring.
Intervals of measurement
Resorption markers: Before starting treatment and 3 or 6 months after treatment has been initiated.
Formation markers: Before starting treatment and 6 months after treatment has been initiated.
Further monitoring is not required if the drug is found efficacious.
61. Bone markers may in future emerge as one of the risk factors that can be utilized for prediction of osteoporosis fracture. While BMD provides a static picture of bone, the bone markers provides a dynamic measure of bone turnover and distinguish between fast and slow bone losers at menopause transition and may aid in decision making (GRADE B).
MANAGEMENT
62. A population based and a personalized approach is to be implemented to prevent and treat post-menopausal osteoporosis. This target is achieved by primary prevention (population based), intervention, and rehabilitation (individualized).
63. Fracture risk is defined by BMD (both primary and secondary causes) and clinical risk factors for osteoporotic fracture. For treatment purpose, combining BMD with clinical risk factors provides a better estimate of fracture risk. Hence, it will be easier to use a risk assessment tool like FRAX with or without BMD for risk assessment. We simply should not treat T-scores, but must take a patient’s full clinical status into account when we make therapeutic decisions.
64. It is good to understand the term prevention and treatment in the context of osteoporosis. The term prevention is used to denote the prevention of bone loss in post-menopausal women with osteopenia (T-score between −1 and −2.5) and increased fracture risk. Treatment is defined as a reduction in fracture risk in post-menopausal women with osteoporosis.
UNIVERSAL RECOMMENDATIONS
65. Life-style management
Balanced diet, adequate physical activity, and exposure to sunlight avoidance of bone depleting agents such as tobacco and alcohol.
66. Nutrition
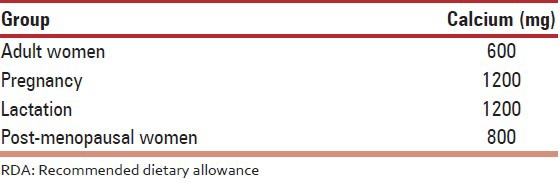
The recommended dietary allowance (RDA) of calcium intake for adult Indian women is given in Table 2.[82]
67. Assess the total calcium intake from dietary sources and if needed, supplements are used to correct the deficient balance. The intake should exceed > 800 mg/day (GRADE B). The risk of cardiovascular events, calculi are not observed with the recommended doses of calcium.
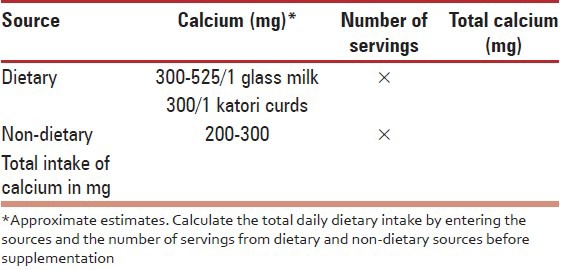
68. The following tool depicted in Table 3 can be used for a quick calculation of daily calcium intake.
Table 3.
Quick dietary calcium assessment chart: A tool for a quick assessment of total dietary calcium intake
69. Low sodium intake: Daily salt intake should not exceed 5 g (1 teaspoon). Protein should be 1 g/kg body weight.[82]
70. Decrease caffeine intake (< 3 cups/day), limit alcohol and avoid the use of tobacco (GRADE B). A cup (150 mL) of brewed coffee contains 80-120 mg of caffeine and instant coffee 50-65 mg while tea contains 30-65 mg of caffeine. Caffeine stimulates the central nervous system and induces physiological dependency. In general, low doses (20-200 mg) of caffeine produce mild positive effects such as a feeling of well-being, alertness, and energy. Higher doses (>200 mg) can produce negative effects such as nervousness and anxiety, especially in people who do not usually consume caffeine-containing beverages.[82]
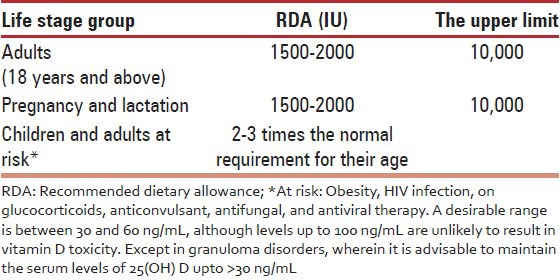
71. Vitamin D deficiency can be considered as a national nutritional deficiency pandemic. In the background of widespread vitamin D deficiency in all age groups, it is prudent to adopt the US Endocrine Society 2011 RDA [Table 5].[83] There is an urgent need for an Indian update on RDA for different age groups.
72. Vitamin D: Dietary sources are limited, adequate sunlight exposure has limitations and presently, food fortified with adequate vitamin D is unavailable in India. Urgent and cost-effective measures need to be implemented. Hence, it is recommended to use vitamin D as supplements, unless it is obtained in adequate daily requirement from natural sources (GRADE A).
73. Recommendations for management of vitamin D deficiency and maintenance are (GRADE B):
Cholecalciferol (vitamin D3) is available in the form of oral tablets and oral spray of 1000 IU and 2000 IU.
It is also available in the form of granules and tablet of 60,000 IU.
Intramuscular (IM) injections of vitamin D3 are available in doses of 300,000 IU and 600,000 IU per ampoule. Injections of cholecalciferol are cost-effective, may be recommended in cases of malabsorption and also to increase compliance. The disadvantage is being an oily injection, it is painful, and since it is administered intramuscularly can produce an erratic blood levels.
Cholecalciferol is the preferred therapy for correction of deficiency and maintenance.
A. Management of deficiency
Cholecalciferol (vitamin D3) tablet or powder 60,000 IU/once a week for 8 weeks preferably with milk or.
One IM injection of 6,00,000 IU is given to correct the deficiency.(not to be repeated before 3 months and may be given after confirmation of persisting low levels of vitamin D).
Maintenance therapy (from natural sources or supplements) is advised after correction of the deficiency.
B. Maintenance therapy
Cholecalciferol tablet or powder 60,000 IU once a month in summer or twice a month in winter.
Vitamin D supplements by oral spray or oral tablets of 1000 IU/day, or.
Injection of cholecalciferol 300,000 IU IM, twice a year or 600,000 IU IM once a year.
Cholecalciferol, 1000 IU daily, will raise blood levels, on average, by approximately 10 ng/mL.
C. Upper acceptable limit
The dose for treatment should not exceed 4000 IU/day and hypercalcemia has been reported when the dose exceeds 10,000 IU/day.
74. Vitamin D derivatives: Calcitriol, the active form of vitamin D is reserved only for patients with chronic renal and hepatic disease. Alfacalcidol is a synthetic analog of the active vitamin D metabolite calcitriol (1,25-dihydroxyvitamin D3), and it is metabolized to calcitriol by its 25-hydroxylation in the liver. It is less potent than calcitriol. The use of vitamin D derivatives necessitates monitoring of serum and possibly urine calcium. There is the risk of hypercalcemia and hypercalciuria. Adverse effects of prolonged hypercalcemia include impairment of renal function and nephrocalcinosis.
75. It is preferable to get vitamin D through sunlight by exposing 20% of body surface area (face, neck, and both arms and forearms) without sunscreen for at least 30 min between 10 am and 3 pm, depending on the season, latitude, altitude, pollution, and skin pigmentation. The sunlight between 11 am and 2 pm is preferably the best.
76. In post-menopausal women, the intake of vitamin D should be in addition to sunlight exposure. Vitamin D supplementation (≥500-2000 IU/day) was favorable in the reduction of hip fracture and any non-vertebral fracture in persons 65 years of age or older.
77. Vitamin K: For women of post-menopausal age, 180-350 μg/day of vitamin K2-7 may need to be supplemented along with the recommended intake of calcium, magnesium, vitamin D, and a balanced diet. The current RDA of vitamin K2-7 WHO of 65-80 μg/day is too low and needs to be raised up to at least 100 μg/day throughout life, with larger doses when needed.[84,85] Both bone and cardiovascular health of women with osteoporosis would benefit from vitamin K2-7 intake.[86,87,88,89,90,91,92,93,94,95,96,97] (GRADE C).
78. Interestingly, exposure to complex nutrients and food constituents interact to affect bone mass, it is however, left to individual clinician to decide on supplementing vitamin A, vitamin B12, and phytoestrogens (GRADE B).
PHYSICAL ACTIVITY
79. Adequate physical activity is needed to maintain bone health. Brisk walking 4-5 times a week for 30 min for hip, back strengthening exercises for spine, and resistances exercises for the upper arm is specific to maintain bone health (GRADE B).
80. Patients with severe osteoporosis should avoid engaging in motions, such as forward flexion exercises, using heavy weights or even performing side-bending exercises, because pushing, pulling, lifting, and bending exert compressive forces on the spine that may lead to fracture (GRADE A).
PREVENTION OF FALLS
81. Patients should receive a multifactorial risk assessment and intervention because; it is the most consistently effective strategy to prevent falls (GRADE A).
82. A fall evaluation includes an assessment of the following: History of fall, circumstances, medications, acute or chronic medical problems, and mobility levels; an examination of vision, gait and balance, and lower extremity joint function; an examination of basic neurological function, including mental status, muscle strength, lower extremity peripheral nerves, proprioception, reflexes, tests of cortical, extrapyramidal, and cerebellar function; assessment of basic cardiovascular status, including heart rhythm, and postural blood pressure.
83. Home hazard assessment and modification, exercise and physical therapy are recommended to prevent falls and injuries from falls. Biomechanics of posture and safe movements are a vital component of counseling (GRADE A).
84. Evaluation of medications (sedatives, antidepressants, antihypertensive, and hypoglycemic) and withdrawal of medications that increase the risk of falling is recommended (GRADE B).
85. Frailty related falls and fractures have been reported with OR of 1.38-2.4 for falls and recurrent falls, 1.40 and 1.7 for hip fracture in old women. Planning of individualized exercise program, for preventing vertebral fractures and strengthening for fall prevention, takes into consideration patients cardiovascular condition, muscular strength, flexibility, core stability, bone’s biochemical competence, etc., The program addresses balance and strengthening for fall and fracture prevention. Women’s health-care programs targeting post-menopausal women’s comprehensive care can contribute a lot by educating women as to take care of their musculoskeletal health through lifelong commitment to proper nutrition, exercise, and understanding about issues related to prevention of falls.[98,99,100]
EMOTIONAL AND PSYCHOLOGICAL FACTORS
86. Education and psychosocial support for various emotional and psychological aspects during treatment for PMO is needed.
87. Recommend smoking cessation and reduced alcohol consumption (GRADE B).
88. Psychiatric evaluation of patients with post-menopausal osteoporosis, structured unstructured, should be carried out whenever indicated, especially in patients with depression, psychosis, suicidal or cognitive impairment. Use brief screening instruments like Whooley’s 2-question screening test for depression (GRADE B).
89. Treatment for osteoporosis has been associated with improved psychological functioning in patients with post-menopausal osteoporosis. This has been seen with pharmacotherapeutic agents such as raloxifene, ibandronate, hormone replacement therapy, exercise-based interventions, etc., Strontium ranelate has been associated with memory impairment. Avoid/minimize the bone depleting action of medications.
90. For all patients having risk factors for secondary osteoporosis, universal recommendations need to be followed.
91. Glucocorticoid-induced osteoporosis (GIOP)
It is the most common secondary cause of osteoporosis.
For all patients receiving any dose of chronic oral glucocorticoid therapy or initiating glucocorticoids (> 7.5 mg prednisolone or equivalent) with an anticipated duration of ≥ 3 months.
Low bone mass is seen with the use of high potency or prolonged low dose inhaled glucocorticoid.
Inhaled glucocorticoid below 400 mcg/day and usage of budesonide or fluticasone seemed to have minimal systemic effects compared to beclomethasone. Use of spacer device significantly reduces the effect of inhaled glucocorticoid on bone formation.
Calcitriol is used for preventing glucocorticoid-induced bone loss and post-transplant-related bone loss (GRADE A).
A baseline BMD is necessary and treatment initiated in cases of osteopenia associated with clinical factors.
Duration of anti-resorptive therapy is as long as the steroids are prescribed. Bisphosphonates are the first-line option for GIOP (GRADE A).
Teriparatide counteracts many aspects of the pathophysiology of GIOP, hence better than anti-resorptive therapy (Ref: Indian Rheumatology Association Guidelines).
92. Women need to be supplemented with calcium and vitamin D while on anticonvulsant therapy,[101] retroviral therapy, and drugs for thyroid dysfunction.
93. We suggest that depot medroxy progesterone (DMP) may be us as a method of contraception (GRADE C). There is no need to limit DMP use to 2 years in most patients; women should be instructed to follow universal recommendations for bone health: Age-appropriate calcium and vitamin D intake, regular weight-bearing exercise, and smoking cessation. DMP should be used with caution in women with major risk factors for low bone density, such as a BMI < 17.5, previous amenorrhea, rheumatoid arthritis, and chronic oral glucocorticoid therapy[101,102,103,104]
94. Low dose (OCPs) oral contraceptive pills is a good choice of hormonal contraception in amenoheric women, women on (GnRH) Gonadotrophin Releasing Hormone analogs and women in the reproductive period (GRADE B).
PHARMACOTHERAPY
95. Treatment should be considered in women
Presenting with fragility fractures.
Radiographic diagnosis of incidental vertebral fracture and osteopenia.
Diagnosis of osteoporosis based on DXA, i.e., T-score of less than −2.5 at hip or spine.
With secondary causes and high-risk of fractures.
In the absence of BMD measurements by DXA, intervention is individualized, understanding and considering the cost benefit and risk benefit outcome of the intervention.
96. Health-care professionals managing PMO should be aware of the concepts of compliance, adherence, concordance, and persistence, and work to improve adherence in patients of PMO, in order to optimize therapeutic outcomes.
97. In choosing therapy, drug-related (risk-benefit), patient profile (age, years since menopause, symptoms, comorbidities) and environment-related factors (economics and social) should be identified. Patients should be educated in PMO and its treatment and empowered to take part in shared decision making to improve adherence.
98. Patients should be monitored initially, every 3-6 months for 2-3 contacts, then annually for clinical assessment. We suggest that markers of bone resorption and formation may be tested at baseline and after 3-6 months of therapy in certain situations and research settings (GRADE C).
99. We suggest that DXA should be performed every 2 years on the same machine in order to monitor osteoporosis therapy (GRADE B).
Measurement error must be considered when interpreting serial BMD assessments in order to determine whether the change is real and not simply random fluctuation or artefact.
Each center should determine its precision error in order to estimate the least significant change (i.e. the change in BMD required to have 95% confidence that the change is real).
However, most osteoporosis therapies do not cause large increases in BMD, and the anti-fracture effect of treatment is only partly explained by the relatively small changes in BMD.
Stable BMD is consistent with successful treatment.
100. Non-responders to PMO therapy may be due to poor adherence, poor calcium/vitamin D health, and untreated secondary osteoporosis, concomitant therapy with skeletotropic drugs, inappropriate choice of drugs or wrong choice of monitoring strategies (GRADE C).
101. Duration of therapy has to be individualized depending on the patient’s profile, drug used, and response to therapy.
102. There is no recommendation on combination therapies, sequential therapies and drug holidays; these should be planned as per individual patient’s need.
BISPHOSPHONATES
103. Bisphosphonates are recommended as first-line drugs for treating post-menopausal women, with proven efficacy in the prevention of vertebral and non-vertebral fractures, including hip fractures (GRADE A).
104. Fracture reduction is seen after 1 year of treatment.
105. Alendronate 70 mg weekly has similar efficacy to alendronate 10 mg daily in the treatment of post-menopausal osteoporosis. Continuous use of alendronate, for up to 10 years, if clinically indicated, produces a sustained increase in BMD and 55% significant reduction in spine fracture with a good safety profile (GRADE A).
106. Risedronate: This is associated with up to 49% reduction in new vertebral fracture in women with prior vertebral fractures and 39% reduction in non-vertebral fractures. Vertebral fracture risk reduction is seen after 6 months of therapy. Reduction of hip fracture risk after 3 years was 40% in women with confirmed osteoporosis and 60% in women with at least one coexisting vertebral fracture. Currently, the use of risedronate for up to 7 years is safe and efficacious. Risedronate 35 mg once weekly has similar efficacy to the 5 mg daily dosing (GRADE A).
107. Ibandronate: Oral ibandronate 2.5 mg daily for 3 years reduces vertebral fracture by 62% in post-menopausal women with prevalent vertebral fracture.
108. Zoledronic acid: Treatment with zoledronic acid (5 mg by intravenous infusion over at least 15 min once yearly) in osteoporotic post-menopausal women reduces the incidence of vertebral fracture by 70% over 3 years with significant reduction seen by 1 year. Hip fracture is reduced by 41% and non-vertebral fracture by 25% over 3 years (GRADE A). Zoledronic acid yearly infusion is also indicated for the prevention of new clinical fractures in patients who recently (within 90 days) have had a low trauma hip fracture. It has also been shown to be associated with a reduction in mortality.
109. Adverse effects of bisphosphonates: An association has been suggested between atypical femur shaft fractures and over suppression of bone turnover in patients exposed to bisphosphonates for longer than 3-5 years, particularly in younger Asian women.[105]
110. Bisphosphonate-related osteonecrosis of the jaw is a rare complication. Routine dental care is recommended for all patients and postponing the therapy until the dental treatment has been carried out. Patients who are vitamin D insufficient may be at higher risk for this complication. Calcium and vitamin D deficiency should be corrected before initiating the therapy (GRADE A).
HORMONE THERAPY
111. Estrogen progesterone therapy/estrogen therapy (EPT/ET) may be used for prevention and treatment of osteoporosis in the early post-menopause in symptomatic women unless there is a contra-indication. ET/EPT prevents all osteoporotic fractures even in low risk population, it increases lumbar spine BMD up to 7.6% and femoral neck BMD up to 4.5% over 3 years. It reduces the risk of spine, hip, and other osteoporotic fractures by 33-40% (GRADE A).
112. Pre-hormone therapy (HT) work-up and an annual follow-up are essential when prescribing HT. The dose and duration of HT should be individualized, and a risk-benefit assessment carried out annually. A full gynecological assessment is mandatory prior to starting HT and at regular intervals thereafter. Self-breast examination is advised monthly and clinical breast examination at least annually. Mammogram where available, should be carried out 1-3 yearly if the initial mammogram is normal (GRADE C).
113. All preparations, including low dose, non-oral routes of estrogen are effective in preserving bone mass. In women with hypertriglyceridemia, obesity, glucose intolerance, history of deep vein thrombosis, and tobacco users, non-oral route should be preferred (GRADE B).
114. HT should not be started solely for bone protection after 10 years of menopause. Extended use of HT in women with reduced bone mass is an option after considering the risk-benefit analysis compared to the other available therapies for osteoporosis. The bone protective effect is lost after stopping HT (GRADE B).
115. HT is indicated as primary therapy to prevent bone loss in women with premature menopause and secondary amenorrhea (GRADE C).
116. Progestogens should be added to ET in women with uterus (GRADE A).
117. If menopausal hormone therapy is given to women below the age of 60 or within 10 years of menopause, the risks are rare. Tables 6 and 7 elaborate the risks and benefits in terms that can be used during counseling for easy and understandable communication.
Table 6.
Based on WHI: Number of excess events on HT versus placebo per 10,000 women/year of HT use between the age group of 50-59 years
118. Classification of Frequency of Drug Reactions (according to WHO and Council for International Organizations of Medical Sciences)
Very common > 1/10.
Common (frequent) >1/100 and < 1/10.
Uncommon (infrequent) >1/1000 and < 1/100,
Rare > 1/10,000 and < 1/1000.
Very rare<1/10,000.
119. Harms: Based on WHI, number of excess events on HT versus placebo per 10,000 women/year of HT. Use between the age group of 50 years and 59 years (GRADE A) [Table 6].
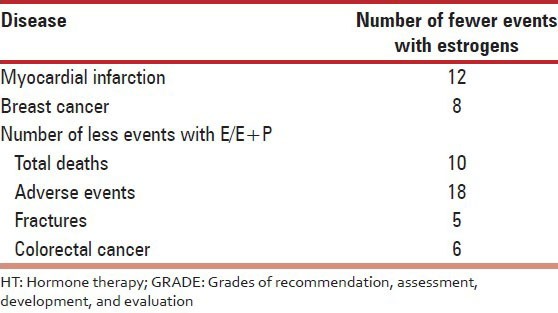
120. Benefits: Benefit of hormone therapy are shown in Table 7.
TIBOLONE
121. Tibolone is a selective tissue estrogenic activity regulator. It is a synthetic steroid compound, which has estrogenic, progestogenic and androgenic properties. It has an estrogenic effect on bone, inhibiting bone resorption by reducing osteoclastic activity. Tibolone is approved in 90 countries to treat menopausal symptoms and in 45 countries to prevent osteoporosis. It should be prescribed 1 year after amenorrhea.
122. Tibolone is effective in treating vasomotor symptoms and improves urogenital atrophy (GRADE A). It improves libido (GRADE B).
123. We recommend that tibolone is prescribed in a single daily dose of 2.5 mg orally. A lower dose of 1.25 mg has been found to be equally effective for most indications, including osteoporosis (GRADE A).
124. Tibolone reduces the risk of vertebral and non-vertebral fracture in older osteoporotic women. Tibolone prevents bone loss and is as effective as standard doses of conventional post-menopausal hormone therapy. Tibolone increases lumbar spine and total hip BMD to a statistically significantly greater extent than raloxifene (GRADE A).
125. It does not increase the risk of venous thromboembolism (VTE) and CVD Cardiovascular events (GRADE B).
126. It does not induce endometrial hyperplasia or carcinoma in post-menopausal women (GRADE A).
127. We suggest that tibolone may be preferable to HRT in symptomatic menopausal women with mammographically dense breast tissue (GRADE B).
128. We suggest that tibolone may be used as add-back therapy with GnRH analogs for vasomotor symptoms and to maintain BMD (GRADE B).
129. We recommend that tibolone should not be used in breast cancer survivors as it increases the recurrence risk (GRADE A).
130. We recommend that tibolone should be used with caution in women over 60 years and should not be used in those who have strong risk factors for stroke (GRADE A).
Selective estrogen receptor modulators
131. Selective estrogen receptor modulators (e.g. raloxifene at 60 mg daily) improve and preserve bone density at the spine (2.6%) and hip (2.1%) after 4 years with a simultaneous reduction by 76% in the risk of invasive breast cancer. Anti-fracture efficacy on hip is lacking (GRADE A).
132. Raloxifene has been shown to be beneficial in reducing new vertebral fracture risk by 69% in post-menopausal women with osteoporosis and 47% in post-menopausal women with osteopenia over 3 years (GRADE A).
133. Raloxifene can be used as therapy for the prevention and treatment of osteoporosis especially for women with an increased risk of breast cancer (GRADE A).
134. Raloxifene and estrogen are associated with a similar increased risk of VTE (GRADE A). However, no cases of VTE were reported among healthy post-menopausal Asian women whilst on raloxifene Other side-effects include hot flushes, which are more likely in the peri-menopausal period, and leg cramps.
Teripartide
135. Teriparatide is reserved for treating women at high-risk for fracture, including those with very low BMD and with a previous vertebral fracture. 20 mcg/day SC is given for 18 months. S. calcium and S. uric acid are monitored at 1, 6, and 12 months. A recommendation can be made for treatment with anti-resorptive therapy (bisphosphanates) following discontinuation of PTH (GRADE A).
Calcitonin
136. Calcitonin is approved for PMO treatment, but not for prevention.
Strontium ranelate
137. Strontium ranelate is an effective treatment to prevent fractures in PMO with a novel dual mechanism of action (GRADE B). However, only more experience will decide the future of this drug.
138. Anabolic steroids may be used in very old frail women with sarcopenia for a period of 6 months.
SURGICAL MANAGEMENT
139. Fractures: Vertebral compression fractures are common, but are often silent consequences of osteoporosis
140. MRI of the spine is probably the single most useful test for evaluating a fracture (R: GRADE C).
Hip fracture
141. Occult hip fractures are not uncommo.
142. In intra-capsular fractures, internal fixation could be considered, if the fracture can be reduced anatomically (GRADE B).
143. Hemi-arthroplasty should be cemented to eliminate thigh pain secondary to loosening and is ideal for elderly patients with limited life expectancy (GRADE A).
144. Total hip replacement should be considered when internal fixation is inappropriate or contraindicated in physiologically younger patients for improved quality of life (GRADE B).
145. All patients who suffer from a hip fracture should be subjected to BMD after surgery where possible and appropriate treatment for osteoporosis initiated (GRADE A).
146. Long bone fractures – preferred fixation – close reduction and intramedullary nailing (GRADE A).
147. Juxtra-articular fractures – preferred fixation – close reduction and anatomical locking plates with variable angle screws (GRADE A).
149. Articular fractures – unstable/comminuted replacement may be an option in elderly patients (GRADE B).
150. Post-fracture fixation – patient specific osteoporosis related medical management to avoid subsequent fractures (GRADE A).
151. Post-operatively start patients on:
Calcium and vitamin D as needed and start appropriate treatment for osteoporosis.
When indicated drugs like teriparatide, which facilitate osteoblastic bone formation can be started (GRADE A).
Anti-resorptive drugs like bisphosphonates are started 4-6 weeks later (GRADE B).
Spine fracture
152. All vertebral compression fractures without neurological deficit are treated conservatively for 3 weeks as majority get better during this period.
153. Percutaneous vertebroplasty and kyphoplasty have a definite role in the management of those vertebral compression fractures that do not respond to non-operative treatment (GRADE A).
REHABILITATION
154. Use of phase wise physiotherapy based on severity of osteoporosis, hip/spine affection.
155. Use of strengthening, resistance, weight-bearing exercise depending on age and severity of osteoporosis.
156. Combined approach using occupational and diet therapy along.
ECONOMICS OF OSTEOPOROSIS
157. Advising life-style measures to all post-menopausal women, improving calcium intake in diet, and increasing physical activity improves bone health and is cost-effective (GRADE B).
158. Prescription of calcium and vitamin D to all post-menopausal women with a view to improve bone health and prevent osteoporosis and its consequent fractures is the cost-effective strategy (GRADE A).
159. Screening post-menopausal women for osteoporosis/osteopenia by DXA at hip/spine and biochemical test is a cost-effective strategy (GRADE A).
160. Treatment of post-menopausal women with diagnosed osteoporosis is the cost-effective treatment strategy (GRADE A).
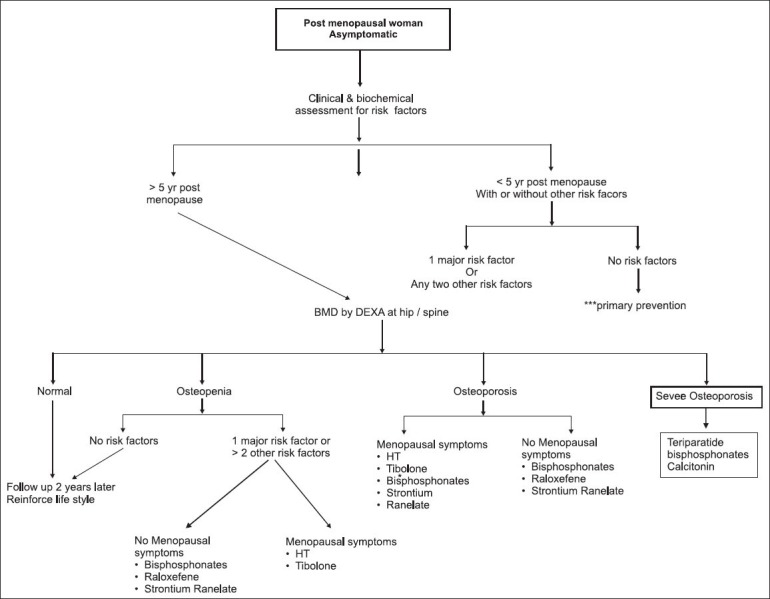
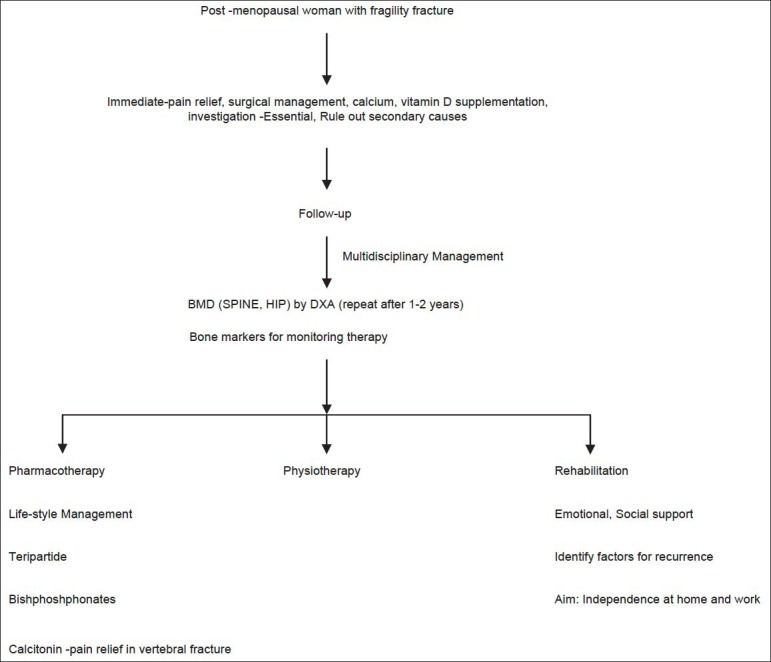
Flowcharts 1 and 2 show an approach to management of asymptomatic post-menopausal woman and post-menopausal woman with fragility fracture, respectively.
Decision making in the management of PMO is depicted in Flowcharts 1 and 2.
REFERENCES
1.Cooper C, Campion G, Melton LJ., 3rd Hip fractures in the elderly: A world-wide projection. Osteoporos Int. 1992;2:285–9. doi: 10.1007/BF01623184. [DOI] [PubMed] [Google Scholar]
2.Kado DM, Browner WS, Palermo L, Nevitt MC, Genant HK, Cummings SR. Vertebral fractures and mortality in older women: A prospective study. Study of Osteoporotic Fractures Research Group. Arch Intern Med. 1999;159:1215–20. doi: 10.1001/archinte.159.11.1215. [DOI] [PubMed] [Google Scholar]
3.Consensus development conference: Prophylaxis and treatment of osteoporosis. Am J Med. 1991;90:107–10. doi: 10.1016/0002-9343(91)90512-v. [DOI] [PubMed] [Google Scholar]
4.NIH consensus development panel on osteoporosis prevention, diagnosis, and therapy, March 7-29, 2000: Highlights of the conference. South Med J. 2001;94:569–73. [PubMed] [Google Scholar]
5.Kanis JA Assessment of Osteoporosis at the Primary Health Care Level 2008 World Health Organisation Scientific Group. UK: University of Shiffield; 2007. WHO Collaboration Centre for Metabolic Bone Diseases. [Google Scholar]
6.Dawson-Hughes B National Osteoporosis Foundation Guide Committee. A revised clinician's guide to the prevention and treatment of osteoporosis. J Clin Endocrinol Metab. 2008;93:2463–5. doi: 10.1210/jc.2008-0926. [DOI] [PubMed] [Google Scholar]
7.Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P, et al. Predictive value of BMD for hip and other fractures. J Bone Miner Res. 2005;20:1185–94. doi: 10.1359/JBMR.050304. [DOI] [PubMed] [Google Scholar]
8.Kanis JA, Johnell O, Oden A, De Laet C, Mellstrom D. Diagnosis of osteoporosis and fracture threshold in men. Calcif Tissue Int. 2001;69:218–21. doi: 10.1007/s00223-001-1046-6. [DOI] [PubMed] [Google Scholar]
9.Lewiecki EM, Gordon GB, Baim S, Leonard MB, Nicholas J. Vol. 43. BishopBone: Elseiver; 2008. International Society for Clinical Densitometry 2007 Adult and Pediatric; pp. 1115–21. [DOI] [PubMed] [Google Scholar]
10.New Delhi: Indian Council of Medical Research; 2010. ICMR Taskforce Study. Population based reference standards of peak bone mineral density of Indian males and female. An ICMR multicentre task force study. [Google Scholar]
11.Marwaha RK, Tandon N, Kaur P, Sastry A, Bhadra K, Narang A, et al. Establishment of age-specified bone mineral density reference range for Indian females using dual-energy X-ray absorptiometry. J Clin Densitom. 2012;15:241–9. doi: 10.1016/j.jocd.2011.09.006. [DOI] [PubMed] [Google Scholar]
12.Makker A, Mishra G, Singh BP, Tripathy A, Singh MM. Normative bone mineral density data at multiple skeletal sites in Indian subjects. Arch Osteoporos. 2008;3:25–37. [Google Scholar]
13.Patni R. Normal BMD values for Indian females aged 20-80 years. J Midlife Health. 2010;1:70–3. doi: 10.4103/0976-7800.76215. [DOI] [PMC free article] [PubMed] [Google Scholar]
14.Marwaha RK, Tandon N, Shivaprasad C, Kanwar R, Mani K, Aggarwal R, et al. Peak bone mineral density of physically active healthy Indian men with adequate nutrition and no known current constraints to bone mineralization. J Clin Densitom. 2009;12:314–21. doi: 10.1016/j.jocd.2009.05.004. [DOI] [PubMed] [Google Scholar]
15.Nangia S, Arya V, Gujral Ratni B, Mithal A. Lucknow: Presented at 27th Annual Meeting of The Endocrine Society of India; 1997. Spinal bone mineral density in normal Indian females. [Google Scholar]
16.Arya V, Nangia S, Gujral RB, Mithal A. Lucknow: Presented at 27th Annual Meeting of The Endocrine Society of India; Femoral bone mineral density in normal Indian females. [Google Scholar]
17.Pande KC, Johansen KB, Helboe AB. Digital X-ray radiogrammetry: Establishment and comparison of Indian female and male normative reference data. J Bone Miner Res. 2001;16(Suppl 1) M0871997. [Google Scholar]
18.Harinarayan CV, Ramalakshmi T, Prasad UV, Kumar EG, Srinivasa Rao PV. Ultrasound bone mineral density of os calcis-its relationship with bone mineral markers and 25(OH) vitamin D in endemic fluorotic and non-fluorotic villages. J Clin Sci Res. 2012;1:157–62. [Google Scholar]
19.Parfitt AM. The coupling of bone formation to bone resorption: A critical analysis of the concept and of its relevance to the pathogenesis of osteoporosis. Metab Bone Dis Relat Res. 1982;4:1–6. doi: 10.1016/0221-8747(82)90002-9. [DOI] [PubMed] [Google Scholar]
20.Bessette L, Ste-Marie LG, Jean S, Davison KS, Beaulieu M, Baranci M, et al. The care gap in diagnosis and treatment of women with a fragility fracture. Osteoporos Int. 2008;19:79–86. doi: 10.1007/s00198-007-0426-9. [DOI] [PubMed] [Google Scholar]
21.Papaioannou A, Wiktorowicz ME, Adachi JD, Goeree R, Papadimitropoulos E, Bedard M, et al. Mortality, independence in living and re-fracture, one year following hip fracture in Canadians. J Soc Obstet Gynaecol Can. 2000;22:591–7. [Google Scholar]
22.Colón-Emeric C, Kuchibhatla M, Pieper C, Hawkes W, Fredman L, Magaziner J, et al. The contribution of hip fracture to risk of subsequent fractures: Data from two longitudinal studies. Osteoporos Int. 2003;14:879–83. doi: 10.1007/s00198-003-1460-x. [DOI] [PubMed] [Google Scholar]
23.Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: Evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146–56. doi: 10.1093/gerona/56.3.m146. [DOI] [PubMed] [Google Scholar]
24.Cole ZA, Dennison EM, Cooper C. Osteoporosis epidemiology update. Curr Rheumatol Rep. 2008;10:92–6. doi: 10.1007/s11926-008-0017-6. [DOI] [PubMed] [Google Scholar]
25.Joshi VR, Mangat G, Balakrishnan C, Mittal G. Osteoporosis – Approach in Indian scenario. J Assoc Physicians India. 1998;46:965–7. [PubMed] [Google Scholar]
26.Makkar A, Mishra G, Singh BP. Peak bone density at multiple skeletal sites in Indian subjects. Arch Osteoporos. 2008;3:25–3. [Google Scholar]
27.Chibber G, Roy R, Eunice M, Srivastava M, Ammini AC. Prevalence of osteoporosis among elderly women living in Delhi and rural Haryana. IJEM. 2007;1:11–4. [Google Scholar]
28.Shatrugna V, Kulkarni B, Kumar PA, Rani KU, Balakrishna N. Bone status of Indian women from a low-income group and its relationship to the nutritional status. Osteoporos Int. 2005;16:1827–35. doi: 10.1007/s00198-005-1933-1. [DOI] [PubMed] [Google Scholar]
29.Gandhi A, Shukla AR. Evaluation of BMD of women above 40 years of age. J Obstet Gynecol India. 2005;55:265. [Google Scholar]
30.Meeta . Spain: Poster Presented at International Menopause Meeting; 2008. Evaluation of Risk Factors for Dexa Referral in Indian Women. Abstract book. [Google Scholar]
31.Krishna U, Mehta RU. Osteoporosis–Incidence and implications. J Obstet Gynecol India. 2000;50:150–6. [Google Scholar]
32.Babu AS, Ikbal FM, Noone MS, Joseph AN, Samuel P. Osteoporosis and osteopenia in India: A few more observations. Indian J Med Sci. 2009;63:76–7. [PubMed] [Google Scholar]
33.Sharma S, Tandon VR, Mahajan A, Kour A, Kumar D. Preliminary screening of osteoporosis and osteopenia in urban women from Jammu using calcaneal QUS. Indian J Med Sci. 2006;60:183–9. [PubMed] [Google Scholar]
34.Pande KC. Prevalence of low bone mass in healthy Indian population. J Indian Med Assoc. 2002;100:598–600. 602. [PubMed] [Google Scholar]
36.Paul TV, Thomas N, Seshadri MS, Oommen R, Jose A, Mahendri NV. Prevalence of osteoporosis in ambulatory postmenopausal women from a semiurban region in Southern India: Relationship to calcium nutrition and vitamin D status. Endocr Pract. 2008;14:665–71. doi: 10.4158/EP.14.6.665. [DOI] [PubMed] [Google Scholar]
37.Aggrawal N, Bathla S, Juneja S. Measurement of bone mineral density by dexa scan in postmenopausal women. Obs Gynae Today. 2004;9:768–71. [Google Scholar]
38.Meeta . Chandigarh: Poster at the Annual Indian Menopause Society meeting; 2006. Feb 4-5, Two hundred and six reasons to be informed about osteoporosis. [Google Scholar]
39.Unni J, Garg R, Pawar R. Bone mineral density in women above 40 years. J Midlife Health. 2010;1:19–22. doi: 10.4103/0976-7800.66989. [DOI] [PMC free article] [PubMed] [Google Scholar]
40.Savardekar LS, Shah RS, Iddya U, Balaiah D, Parihar A, Jaknkaria B. Bone density in normal Indian women: Assessment by USG and DEXA. Obs Abd Gynae Today. 2004;9:772–6. [Google Scholar]
41.Meeta, Shaantanu, Tanvir Assessment of risk factors for osteoporosis in Indian women submitted for publication -yet to be and published, -details from drmeeta919@gmail.com
42.Dhanwal DK, Siwach R, Dixit V, Mithal A, Jameson K, Cooper C. Incidence of hip fracture in Rohtak district, North India. Arch Osteoporos. 2013;8:135. doi: 10.1007/s11657-013-0135-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
43.International Osteoporosis Foundation. The Asian Audit: Epidemiology, costs and burden of osteoporosis in Asia 2009. 2009. [Last accessed on 2013 Jan 2]. Available from: http://www.iofbonehealth.org .
44.Sankaran B. Clinical studies: Incidence of fracture neck of femur and intertrochanteric fractures in three Delhi hospitals. In: Sankaran B, editor. Osteoporosis. New Delhi: South East Asia Regional Office, World Health Organisation; 2000. pp. 9–18. [Google Scholar]
45.Jha RM, Mithal A, Malhotra N, Brown EM. Pilot case-control investigation of risk factors for hip fractures in the urban Indian population. BMC Musculoskelet Disord. 2010;11:49. doi: 10.1186/1471-2474-11-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
46.Marwaha RK, Tandon N, Gupta Y, Bhadra K, Narang A, Mani K, et al. The prevalence of and risk factors for radiographic vertebral fractures in older Indian women and men: Delhi Vertebral Osteoporosis Study (DeVOS) Arch Osteoporos. 2012;7:201–7. doi: 10.1007/s11657-012-0098-8. [DOI] [PubMed] [Google Scholar]
47.Balasubramanian K, Rajeswari J, Gulab, Govil YC, Agarwal AK, Kumar A, et al. Varying role of vitamin D deficiency in the etiology of rickets in young children vs. adolescents in northern India. J Trop Pediatr. 2003;49:201–6. doi: 10.1093/tropej/49.4.201. [DOI] [PubMed] [Google Scholar]
48.Harinarayan CV, Ramalakshmi T, Venkataprasad U. High prevalence of low dietary calcium and low vitamin D status in healthy south Indians. Asia Pac J Clin Nutr. 2004;13:359–64. [PubMed] [Google Scholar]
49.Kalra S, Kalra B, Khandelwal SK. Vitamin D deficiency in healthy postmenopausal women in Haryana. World J Life Sci Med Res. 2011;1:11. [Google Scholar]
50.Harinarayan CV. Prevalence of vitamin D insufficiency in postmenopausal south Indian women. Osteoporos Int. 2005;16:397–402. doi: 10.1007/s00198-004-1703-5. [DOI] [PubMed] [Google Scholar]
51.Singh M. Early age of natural menopause in India, a biological marker for early preventive health programs. Climacteric. 2012;15:581–6. doi: 10.3109/13697137.2011.643514. [DOI] [PubMed] [Google Scholar]
52.Harinarayan CV, Joshi SR. Vitamin D status in India – Its implications and remedial measures. J Assoc Physicians India. 2009;57:40–8. [PubMed] [Google Scholar]
53.Sachan A, Gupta R, Das V, Agarwal A, Awasthi PK, Bhatia V. High prevalence of vitamin D deficiency among pregnant women and their newborns in northern India. Am J Clin Nutr. 2005;81:1060–4. doi: 10.1093/ajcn/81.5.1060. [DOI] [PubMed] [Google Scholar]
54.Marwaha RK, Tandon N, Reddy DR, Aggarwal R, Singh R, Sawhney RC, et al. Vitamin D and bone mineral density status of healthy schoolchildren in northern India. Am J Clin Nutr. 2005;82:477–82. doi: 10.1093/ajcn.82.2.477. [DOI] [PubMed] [Google Scholar]
55.Harinarayan CV, Appicatlaa L, Nalini BA, Joshi S. Efficacy and safety of cholecalciferol supplementation in Vitamin D deficient subjects based on endocrine society clinical practice guidelines. Endocrinol Metab Syndr. 2012;S4:004. [Google Scholar]
56.Goswami R, Gupta N, Ray D, Singh N, Tomar N. Pattern of 25-hydroxy vitamin D response at short (2 month) and long (1 year) interval after 8 weeks of oral supplementation with cholecalciferol in Asian Indians with chronic hypovitaminosis D. Br J Nutr. 2008;100:526–9. doi: 10.1017/S0007114508921711. [DOI] [PubMed] [Google Scholar]
57.Agarwal N, Faridi MM, Aggarwal A, Singh O. Vitamin D Status of term exclusively breastfed infants and their mothers from India. Acta Paediatr. 2010;99:1671–4. doi: 10.1111/j.1651-2227.2010.01912.x. [DOI] [PubMed] [Google Scholar]
58.Harinarayan CV, Sachan A, Reddy PA, Satish KM, Prasad UV, Srivani P. Vitamin D status and bone mineral density in women of reproductive and postmenopausal age groups: A cross-sectional study from south India. J Assoc Physicians India. 2011;59:698–704. [PubMed] [Google Scholar]
59.Marwaha RK, Tandon N, Garg MK, Kanwar R, Narang A, Sastry A, et al. Vitamin D status in healthy Indians aged 50 years and above. J Assoc Physicians India. 2011;59:706–9. [PubMed] [Google Scholar]
60.Mithal A, Arya V. Vitamin D status in urban North India adults. J Bone Miner Res. 1999;14(suppl) Abstract. [Google Scholar]
61.Beloyartseva M, Mithal A, Kaur P, Kalra S, Baruah MP, Mukhopadhyay S, et al. Widespread vitamin D deficiency among Indian health care professionals. Arch Osteoporos. 2012;7:187–92. doi: 10.1007/s11657-012-0096-x. [DOI] [PubMed] [Google Scholar]
62.Goswami R, Gupta N, Goswami D, Marwaha RK, Tandon N, Kochupillai N. Prevalence and significance of low 25-hydroxyvitamin D concentrations in healthy subjects in Delhi. Am J Clin Nutr. 2000;72:472–5. doi: 10.1093/ajcn/72.2.472. [DOI] [PubMed] [Google Scholar]
63.Zargar AH, Ahmad S, Masoodi SR, Wani AI, Bashir MI, Laway BA, et al. Vitamin D status in apparently healthy adults in Kashmir Valley of Indian subcontinent. Postgrad Med J. 2007;83:713–6. doi: 10.1136/pgmj.2007.059113. [DOI] [PMC free article] [PubMed] [Google Scholar]
64.Gupta A. Osteoporosis in India— The nutritional hypothesis. In: Mithal A, Rao DS, Zaidi M, editors. Metabolic Bone Disorders. Lucknow: Hindustani Book Depot; 1998. p. 115. [Google Scholar]
65.Teotia SP, Teotia M. Nutritional bone disease: The continuing challenge to neonatal bone health. Postgrad Med. 2009;23:30–8. [Google Scholar]
66.Nangia S, Arya V, Gujral RB, Mithal A. Spinal bone mineral density in normal Indian females. In: Mithal A, Rao DS, Zaidi M, editors. Metabolic Bone Disorders. Lucknow: Hindustani Book Depot; 1998. p. 213. [Google Scholar]
67.Nangia S, Arya V, Gujral RB, Mithal A. Mittal A, Rao DS, Zaidi M, editors. Femoral bone mineral density in normal Indian females. Metabolic bone disorders Indian Society for Bone and Mineral Research. 1998:215. [Google Scholar]
68.Singh M, Magon N, Singh T. Major and minor discordance in the diagnosis of postmenopausal osteoporosis among Indian women using hip and spine dual-energy X-ray absorptiometry. J Midlife Health. 2012;3:76–80. doi: 10.4103/0976-7800.104457. [DOI] [PMC free article] [PubMed] [Google Scholar]
69.Reddy PG, Mithal A, Rao DS. Bone mineral density in healthy Asian Indian women: Development of a reference database and implications for diagnosis of osteoporosis in Indian women living in the United States [abstract] J Bone Miner Res. 2002;17(Suppl 1):SA270. [Google Scholar]
70.Shatrugna V. Osteoporosis in Asian region: Newer questions. In: Shetty P, Gopalan C, editors. Diet, Nutrition and Chronic diseases: An Asian Perspective. London: Smith Gordon Co; 1998. pp. 81–3. [Google Scholar]
71.Dhanwal DK, Sahoo S, Gautam VK, Saha R. Hip fracture patients in India have vitamin D deficiency and secondary hyperparathyroidism. Osteoporos Int. 2013;24:553–7. doi: 10.1007/s00198-012-1993-y. [DOI] [PubMed] [Google Scholar]
72.Alekel DL. Mortillaro E, Hussain EA,1999 Lifestyle and biologic contributors to proximal femur bone mineral density and hip axis length in two distinct etnic groups of premenopausal women. Osteoporos Int 9. :327–338. doi: 10.1007/s001980050155. [DOI] [PubMed] [Google Scholar]
73.Marwaha RK, Puri S, Tandon N, Dhir S, Agarwal N, Bhadra K, et al. Effects of sports training and nutrition on bone mineral density in young Indian healthy females. Indian J Med Res. 2011;134:307–13. [PMC free article] [PubMed] [Google Scholar]
74.Davies JH, Evans BA, Gregory JW. Bone mass acquisition in healthy children. Arch Dis Child. 2005;90:373–8. doi: 10.1136/adc.2004.053553. [DOI] [PMC free article] [PubMed] [Google Scholar]
75.Ganpule A, Yajnik CS, Fall CH, Rao S, Fisher DJ, Kanade A, et al. Bone mass in Indian children – Relationships to maternal nutritional status and diet during pregnancy: The Pune maternal nutrition study. J Clin Endocrinol Metab. 2006;91:2994–3001. doi: 10.1210/jc.2005-2431. [DOI] [PubMed] [Google Scholar]
76.Langley-Evans SC. Developmental programming of health and disease. Proc Nutr Soc. 2006;65:97–105. doi: 10.1079/pns2005478. [DOI] [PMC free article] [PubMed] [Google Scholar]
77.Cooper C, Cawley M, Bhalla A, Egger P, Ring F, Morton L, et al. Childhood growth, physical activity, and peak bone mass in women. J Bone Miner Res. 1995;10:940–7. doi: 10.1002/jbmr.5650100615. [DOI] [PubMed] [Google Scholar]
78.Cooper C, Fall C, Egger P, Hobbs R, Eastell R, Barker D. Growth in infancy and bone mass in later life. Ann Rheum Dis. 1997;56:17–21. doi: 10.1136/ard.56.1.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
79.Sayer AA, Cooper C. Fetal programming of body composition and musculoskeletal development. Early Hum Dev. 2005;81:735–44. doi: 10.1016/j.earlhumdev.2005.07.003. [DOI] [PubMed] [Google Scholar]
80.Cooper C, Eriksson JG, Forsén T, Osmond C, Tuomilehto J, Barker DJ. Maternal height, childhood growth and risk of hip fracture in later life: A longitudinal study. Osteoporos Int. 2001;12:623–9. doi: 10.1007/s001980170061. [DOI] [PubMed] [Google Scholar]
81.Dennison EM, Syddall HE, Sayer AA, Gilbody HJ, Cooper C. Birth weight and weight at 1 year are independent determinants of bone mass in the seventh decade: The Hertfordshire cohort study. Pediatr Res. 2005;57:582–6. doi: 10.1203/01.PDR.0000155754.67821.CA. [DOI] [PubMed] [Google Scholar]
82.National Institute of Nutrition, ICMR. Dietary Guidelines for Indians: A Manual. Annexure 3. 2011:89–90. [Google Scholar]
83.Holick MF, Binkley NC, Bischoff-Ferrari HA, Gordon CM, Hanley DA, Heaney RP, et al. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–30. doi: 10.1210/jc.2011-0385. [DOI] [PubMed] [Google Scholar]
84.Recommended Dietary Allowances. 10th ed. Washington, DC: National Academy Press; 1989. Subcommittee on the Tenth Edition of the Recommended Dietary Allowances, Food and Nutrition Board. [Google Scholar]
85.Kaneki M, Hodges SJ, Hosoi T, Fujiwara S, Lyons A, Crean SJ, et al. Japanese fermented soybean food as the major determinant of the large geographic difference in circulating levels of vitamin K2: Possible implications for hip-fracture risk. Nutrition. 2001;17:315–21. doi: 10.1016/s0899-9007(00)00554-2. [DOI] [PubMed] [Google Scholar]
86.Geleijnse JM, Vermeer C, Grobbee DE, Schurgers LJ, Knapen MH, van der Meer IM, et al. Dietary intake of menaquinone is associated with a reduced risk of coronary heart disease: The Rotterdam Study. J Nutr. 2004;134:3100–5. doi: 10.1093/jn/134.11.3100. [DOI] [PubMed] [Google Scholar]
87.Gast GC, de Roos NM, Sluijs I, Bots ML, Beulens JW, Geleijnse JM, et al. A high menaquinone intake reduces the incidence of coronary heart disease. Nutr Metab Cardiovasc Dis. 2009;19:504–10. doi: 10.1016/j.numecd.2008.10.004. [DOI] [PubMed] [Google Scholar]
88.Ikeda Y, Iki M, Morita A, Kajita E, Kagamimori S, Kagawa Y, et al. Intake of fermented soybeans, natto, is associated with reduced bone loss in postmenopausal women: Japanese Population-Based Osteoporosis (JPOS) Study. J Nutr. 2006;136:1323–8. doi: 10.1093/jn/136.5.1323. [DOI] [PubMed] [Google Scholar]
89.Kawana K, Takahashi M, Hoshino H, Kushida K. Circulating levels of vitamin K1, menaquinone-4, and menaquinone-7 in healthy elderly Japanese women and patients with vertebral fractures and patients with hip fractures. Endocr Res. 2001;27:337–43. doi: 10.1081/erc-100106011. [DOI] [PubMed] [Google Scholar]
90.Amizuka N, Li M, Guo Y, Liu Z, Suzuki R, Yamamoto T. Biological effects of vitamin K2 on bone quality. Clin Calcium. 2009;19:1788–96. [PubMed] [Google Scholar]
91.Sokoll LJ, Booth SL, O’Brien ME, Davidson KW, Tsaioun KI, Sadowski JA. Changes in serum osteocalcin, plasma phylloquinone, and urinary gamma-carboxyglutamic acid in response to altered intakes of dietary phylloquinone in human subjects. Am J Clin Nutr. 1997;65:779–84. doi: 10.1093/ajcn/65.3.779. [DOI] [PubMed] [Google Scholar]
92.Yasui T, Uemura H, Umino Y, Yamada M, Kuwahara A, Matsuzaki T, et al. Undercarboxylated osteocalcin concentration in postmenopausal women receiving hormone therapy daily and on alternate days. Menopause. 2006;13:314–22. doi: 10.1097/01.gme.0000177908.40257.cf. [DOI] [PubMed] [Google Scholar]
93.Kanellakis S, Moschonis G, Tenta R, Schaafsma A, van den Heuvel EG, Papaioannou N, et al. Changes in parameters of bone metabolism in postmenopausal women following a 12-month intervention period using dairy products enriched with calcium, vitamin D, and phylloquinone (vitamin K(1)) or menaquinone-7 (vitamin K(2)): The Postmenopausal Health Study II. Calcif Tissue Int. 2012;90:251–62. doi: 10.1007/s00223-012-9571-z. [DOI] [PubMed] [Google Scholar]
94.Emaus N, Gjesdal CG, Almås B, Christensen M, Grimsgaard AS, Berntsen GK, et al. Vitamin K2 supplementation does not influence bone loss in early menopausal women: A randomised double-blind placebo-controlled trial. Osteoporos Int. 2010;21:1731–40. doi: 10.1007/s00198-009-1126-4. [DOI] [PubMed] [Google Scholar]
95.Knapen MH, Drummen NE, Smit E, Vermeer C, Theuwissen E. Three-year low-dose menaquinone-7 supplementation helps decrease bone loss in healthy postmenopausal women. Osteoporos Int. 2013 doi: 10.1007/s00198-013-2325-6. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
96.Mehta DS, Vaidya RA, Dound YA, Nabar NS, Pandey SN, Vaidya AD. Therapeutic Activity and Safety of Vitamin K2-7 in Muscle Cramps. Indian Pract. 2010;63:287–91. [Google Scholar]
97.Ensrud KE, Ewing SK, Taylor BC, Fink HA, Stone KL, Cauley JA, et al. Frailty and risk of falls, fracture, and mortality in older women: The study of osteoporotic fractures. J Gerontol A Biol Sci Med Sci. 2007;62:744–51. doi: 10.1093/gerona/62.7.744. [DOI] [PubMed] [Google Scholar]
98.Sinaki M. Exercise for patients with osteoporosis: Management of vertebral compression fractures and trunk strengthening for fall prevention. PM R. 2012;4:882–8. doi: 10.1016/j.pmrj.2012.10.008. [DOI] [PubMed] [Google Scholar]
99.Sakuma K, Yamaguchi A. Sarcopenia and age-related endocrine function. Int J Endocrinol 2012. 2012 doi: 10.1155/2012/127362. 127362. [DOI] [PMC free article] [PubMed] [Google Scholar]
100.Menon B, Harinarayan CV. The effect of anti epileptic drug therapy on serum 25-hydroxyvitamin D and parameters of calcium and bone metabolism – A longitudinal study. Seizure. 2010;19:153–8. doi: 10.1016/j.seizure.2010.01.006. [DOI] [PubMed] [Google Scholar]
101.American College of Obstetricians and Gynecologists Committee on Gynecologic Practice. ACOG Committee Opinion No. 415: Depot medroxyprogesterone acetate and bone effects. Obstet Gynecol. 2008;112:727–30. doi: 10.1097/AOG.0b013e318188d1ec. [DOI] [PubMed] [Google Scholar]
102.Cromer BA, Scholes D, Berenson A, Cundy T, Clark MK, Kaunitz AM, et al. Depot medroxyprogesterone acetate and bone mineral density in adolescents – The black box warning: A position paper of the society for adolescent medicine. J Adolesc Health. 2006;39:296–301. doi: 10.1016/j.jadohealth.2006.03.011. [DOI] [PubMed] [Google Scholar]
103.Cundy T, Ames R, Horne A, Clearwater J, Roberts H, Gamble G, et al. A randomized controlled trial of estrogen replacement therapy in long term users of depot medroxyprogesterone acetate. J Clin Endocrinol Metab. 2003;88:78–81. doi: 10.1210/jc.2002-020874. [DOI] [PubMed] [Google Scholar]
104.Khandelwal S, Chandra M, Lo JC. Clinical characteristics, bone mineral density and non-vertebral osteoporotic fracture outcomes among post-menopausal U.S. South Asian Women. Bone. 2012;51:1025–8. doi: 10.1016/j.bone.2012.08.118. [DOI] [PubMed] [Google Scholar]