

Abstract
Translational science requires that scientists from multiple disciplines work together to improve the prevention, diagnosis, and treatment of human disease. Although a literature exists on the design and management of multidisciplinary teams, little has been written on multidisciplinary translational teams (MTTs). MTTs are distinct hybrid entities, with goals taken from both industry and academic models. We identified 30 design factors in 10 domains from a literature survey relevant to our MTT model: specific goals, structures, and processes. These dimensions were adapted to our own institutional environment in the selection and management of 11 MTTs that exploited resources of University of Texas Medical Branch (UTMB) Clinical and Translational Sciences Awards (CTSA). Case illustrations of two specific MTTs illustrate some of the challenges encountered and opportunities realized in terms of education and scientific advances. Network depiction of disciplinarity indicated that CTSA KRs and CTSA leadership contributed to discipline diversity especially in small (or nascent) MTTs. A separate depiction of MTT‐KR utilization indicated that data analysis, translational technologies, and novel methods were heavily utilized by MTTs, whereas other KRs contributed significant effort to infrastructure development. We conclude that the CTSA can provide a rich infrastructural framework and scientific environment for the development of successful MTTs. Clin Trans Sci 2013; Volume 6: 60–71
Keywords: team science, multidisciplinary teams, translational research
Introduction
The need for multidisciplinary teams in translational science
Team‐based models are increasingly used to pursue the technological challenges of “big science” in the postgenomic era.1 Trend analyses of peer‐reviewed scientific publications have concluded that biological science advancements are increasingly the product of multi‐investigator studies, team science is more often cited than the work of an individual researcher, and their work has higher scientific impact.2, 3, 4 The greater impact of multidisciplinary science is attributed to innovation engendered by discipline diversity,5 and, as a result, the formation of teams in science has become widespread.6 Although this analysis has been derived from basic biological and physical sciences, it follows that a team approach is also an appropriate organizational form in translational science due to the breadth and complexity of the T1–T4 spectrum.7, 8, 9, 10 As a result, there is considerable interest in exploiting the potential of the nascent field of the Science of Team Science to facilitate translational research. One framework within which this development can occur is the Clinical and Translational Sciences Awards (CTSA), although other academic structures may serve a similar function.11, 12, 13
Development of team science in translational research
The NIH has published a field guide for collaboration and team science to advance development of scientific teams,14 but this experience may be context‐dependent; the best strategies for academic health centers (AHCs) have yet to be determined, and may vary by the specific context of individual institutions. Applying lessons from multidisciplinary team‐based structures from basic science and industry to academic translational science is inherently complex for several reasons. First, little is known about the optimum way to define, structure, organize, and lead translational research teams.15, 16 Although team development processes for the product‐driven business community are established, how teams can be developed within an academic environment that still satisfy the academic needs for peer recognition and individual advancement is not intuitive. Moreover, the most effective ways to train and develop the membership of translational teams have yet to be determined, as are the necessary skill sets for team participation or leadership.7, 17, 18
In this CTS Special Report, we review considerations of design and support of multidisciplinary teams through integration of literature review and our experience with developing a series of multidisciplinary research teams at the University of Texas Medical Branch (UTMB). We have identified key dimensions for the design and support of MTTs and provide case illustrations developed within the CTSA environment. We discuss the opportunities and challenges in the design and support of MTTs and the value of CTSA structure to teams. This information will simultaneously drive the development of training curricula for CTSA‐affiliated faculty and inform educational competencies for CTSA KL2 programs.
Multidisciplinary Translational Teams (MTTs): A Novel Collaborative Approach to Translational Science
Unique requirements of an MTT
Academic missions include knowledge generation and education, yet MTTs in AHCs must embrace product‐like translational goals to develop or apply a device, diagnostic, therapeutic, or intervention to improve human health. Hence, MTTs represent a unique, hybrid form of team organization. We surveyed organizational team types from business and management literature to inform our implementation of MTT support strategies (an annotated bibliography is available as a Supporting Information online).
Attributes from business teams applicable to MTT development
In our consideration of team development for translational science, we reviewed three distinct academic team types5, 19, 20, 21, 22, 23, 24, 25 and five business team types.26, 27, 28, 29, 30, 31, 32, 33 Although there is a rich literature in business and industry which describes the value of many different types of teams,26, 29, 31, 32, 34 less is known about team science in AHCs.1, 6, 7, 11, 12, 13, 14 Table 1 illustrates the goals, structure, and processes unique to each type. None of the existing team types satisfy the unique combination of attributes of MTTs (highlighted in Table 1).
Table 1.
Comparison of academic and business teams. Academic and business teams differ in goals, structure, and process. Among academic teams, no existing team type satisfies the unique requirements of translational science
| Context | Team Types | Goals | Structure | Processes |
|---|---|---|---|---|
| BUSINESS | Traditional task/project group | Production: profitability, market share, operational efficiency of a product | Centralized and role specific by function | Functional control |
| Capacity development | ||||
| Career development | ||||
| New product design | New Products: Specialized market niche for design or product | Varying levels of centralization depending upon life cycle | Challenge and inquiry utilizing specialized fields of knowledge that are compatible | |
| Cross functional | Decision Making: Disparate and dispersed bases of knowledge/ expertise with constituency buy‐in | Varying levels of centralization depending upon tasks and needs | Broad range of individual expertise or knowledge networks | |
| Virtual | Strategy: Technologically facilitated ideas, designs or solutions without physical presence; low cost | Varying levels of centralization, use of virtual networks | Symmetrical and asymmetrical facilitation | |
| Meetings and decisions mediated by technology | ||||
| Self‐managed | Knowledge: products and processes associated with ownership and commitment | Decentralized and flat, variable and flexible authority | Emergent leadership and control | |
| ACADEMIC | Individual and Multidisciplinary | Research: Publications, papers, patents, grants, funding generating new knowledge | Centralized and role specific, variable by discipline | Mentored learning |
| Integrated care (ICU, transplant, cancer care teams, etc.) | Clinical: Efficiency and effectiveness of care | Centralization based on rank and experience | Implementation of best practices | |
| MTT | Translational (Multidisciplinary): Impact on human health by applications of new diagnostics or therapeutics | Network based with strategic core, flexible participation based on need | Trainees | |
| Capacity development | ||||
| Career development |
From this comparison, we identified attributes from five business team types that are most appropriate to incorporate into an MTT design. The formally designated roles and leadership and objective evaluation criteria characteristic of a Traditional Task/Project Team constitute a strategic core and provide metrics for assessing translational product development (Table 2 ). The focus on innovation characteristic of an industry‐based New Product Design Team is necessary for an MTT to develop new approaches to diagnostic or therapeutic development. Multidisciplinary scientific paradigms in Cross‐Functional Teams inform the structure of an MTT. Technological mediation to enable data visualization and team management in Virtual Teams are applicable to MTTs. Finally, egalitarian governance and transformational leadership characteristic of Self‐Managed Teams are attributes of MTTs that align with academic pursuits.
Table 2.
Business team types and characteristics that inform MTT development. Business team types can inform development of an MTT in an academic health center. Selecting attributes of business teams that foster the goals of a multidisciplinary translational research team results in incorporation of their advantages while avoiding most of the disadvantages in the business model
| Business Team Types | Attributes Desirable to Incorporate in MTTs |
|---|---|
| Traditional Task/Project | • Formally assigned roles and leadership |
| • Formal goals and scientific strategies, as well as objective evaluation criteria from scientific task/project | |
| New Product Design | • Focus on innovation |
| • Focus on speed of discovery and application | |
| Cross‐ Functional | • Focus on creativity possible through managing inherent disciplinary differences |
| • Use of multidisciplinary and divergent scientific paradigms to frame and execute scientific questions and study design | |
| Virtual | • Use of technological mediation to generate ideas, visualize data and phenomena, manage team processes |
| • Geographic, institutional, and disciplinary differences in time and space minimized through technology | |
| Self‐Managed | • Egalitarian governance and transformational leadership present |
| • Use of overarching goals (i.e., scientific/health need) and focal issues, organizing principles, and focus on commitment |
We postulate that MTTs have differentiating purpose, structure, and processes rooted in team organization principles taken from both business and academic environments (Table 3).
Table 3.
Design considerations for the establishment of MTT. The specific structure, processes, and functioning of an MTT will differ based on its goals, its membership, and the design features summarized here
| Design Domain | Design Factors for MTTS |
|---|---|
| Context | • Changing institutional support and federal funding |
| • Traditional academic structures promote silo based philosophies | |
| Tasks | • Scientific inquiry and production requiring high degree of autonomy, interdependence, multidisciplinary thinking, technology mediation, and knowledge management |
| • Acceleration of project to individual and population based health impact | |
| Individual Members | • Selection based on member personalities: openness, self‐efficacy, scientific/academic/social capital |
| • Selection based on potential for high scientific and team skills | |
| Skill Acquisition | • Core competencies in clinical and translational research |
| • eadership development | |
| Team Development | • Frequently nonlinear and based upon opportunities and needs |
| • Based upon collaboration, exchange, active engagement, and is subject to frequent reorientation | |
| Team Structure | • Strategic core of team members maintains scientific focus and continuity |
| • Loosely coupled networks of internal and external collaborators based on need | |
| Team Processes | • Agreed upon charter, vision, goals |
| • Agenda based meetings/team documentation | |
| • Internal and external collaboration/network creation | |
| • Clarity of roles and responsibilities | |
| • Acknowledgment and resolution of conflicts and barriers | |
| • Focus on results and translational goals | |
| • Empowerment‐based leadership and support | |
| • Effective decision making and problem solving | |
| • Acknowledgement/use of expertise | |
| • Focus on development | |
| • Challenge of process and scientific inquiry | |
| Team Reactions and Affective States | • High self‐awareness, consensus on team model, knowledge of individual and team‐based expertise and capacities |
| • Strong commitment to team satisfaction, justice, efficiency, potency, and trust | |
| Team Evolution | • Continuous changes promote learning and adaptation |
| • Episodic, radical, and unexpected changes creating disequilibrium based change and growth | |
| Team Performance | • Accelerated innovation and discovery to address human disease |
| • Translation to population based health outcomes |
MTT Goals/Purpose
The principal goal of an MTT is to develop and apply new knowledge to improvements in human health. The purposes of the MTT span accelerated product development, education and training, improvement of internal teamwork skills, leadership development, and team adaptation. A stated goal of the CTSA (and that of MTTs) is increasing the pace at which diagnostic procedures and new therapeutics are brought to bear on human health. In this respect, MTTs are similar to New Product Teams in industry.35, 36 Training and education imperatives include trainee development, leadership skills, and team‐based capabilities,17, 37 consistent with the CTSA Education and Training Key Function Committee recommended competencies which include leading multidisciplinary teams, facilitating innovation, and fostering creativity.37 Development of teamwork skills improves team effectiveness.38, 39, 40 Finally, teams that learn, adapt, and self‐correct become more effective and innovative over time.41, 42, 43 This capacity to adapt in both scientific and organizational domains is paramount given the dynamic nature of translational science.
MTT structure
Innovative translational research spans a range of expertise, knowledge and tasks in the clinical research continuum. Incorporation of multiple disciplines leads to increased effectiveness and innovation.44, 45, 46 Many types of disciplinary interactions (referred to as “interdisciplinarity,” “multidisciplinarity,” and “transdisciplinarity”) have roles in team‐based translational research,13 but an argument can be made that multidisciplinarity may be the most effective form. First, multidisciplinarity does not require a fully integrated or new discipline be developed to approach a translational project. In the translational continuum, the requirement for specific disciplines and expertise vary not only as a function of team goals, but also with time as the project develops. Second, multidisciplinarity is more time efficient than what a full interdisciplinarity approach would demand. This efficiency better facilitates the MTT goal of accelerated product development. For both of these reasons, we propose that an essential organizing structure of an MTT is that it be legitimately multidisciplinary.
MTTs, as in business Traditional Task/Project Teams, are based on a strategic core structure (Figure 1).47 The roles within the MTT strategic core would be academically defined, and could include a principal investigator, other collaborating scientists from multiple disciplines, a project manager, and trainees. The strategic core may change over time as projects are initiated and concluded; these dynamic changes influence collaboration and performance within the team.
Figure 1.
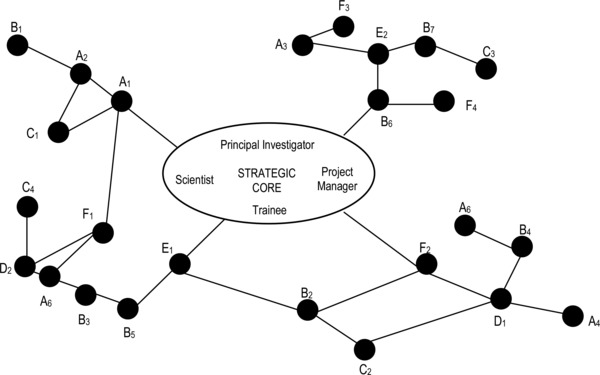
Dynamics of MTT‐network collaborations. Shown is an illustration of the dynamic relationship between MTT and network collaborators. (A) external universities; (B) external research centers; (C) independent research labs; (D) pharmaceutical companies; (E) governmental agencies, (F) CTSA clinical research support‐bio‐repositories, biostatistics, clinical research units, etc.
The strategic core of an MTT interacts with both internal and external networks of collaborators, which gives rise to increased team effectiveness and innovation. These external networks may include other universities and research centers, independent labs, pharmaceutical labs and companies, governmental labs and agencies, as well as key functions such as bio‐repositories, biostatistics, and/or clinical research centers provided by a CTSA or other institutional structure. As the team matures and projects progress, different individuals and networks may engage, disengage and reconfigure its structure as required for progressing along the T1–T3 translational continuum.
MTT processes
Team processes also differentiate an MTT from other types of teams. Collaboration, interdependence, autonomy and self‐selection, egalitarian governance, and technological facilitation are critical features for team performance.48, 49 Collaboration is an academic tradition characteristic of individual laboratories, associated with high performing science teams.50 Here, collaboration is both a process and a product. It is a process in that specific members are chosen and engaged for a given project, and is a product in that such collaboration renders commitment, trust, and team cohesion over time.
Interdependence also distinguishes MTTs from other team types. Considerable research indicates that interdependent, heterogeneous, and diverse teams are more innovative44, 51 and effective.52 Thus, incorporating processes that foster interdependence and diversity of expertise is a key feature of the MTT.
Egalitarian governance and technological facilitation are additional differentiating components of an MTT. Nondirect leadership structures that stress transformational principles such as overall goals, criticality of mission, and alignment of interest with broader institutional goals is critical in effective research‐based teams.53, 54 Given the potential geographic dispersion of many core team members and external collaborators, technologic facilitation may be another essential component of MTTs. Team success is dependent on effective transfer of knowledge and information typical of scientific groups. Recent evidence suggests such facilitation is predictive of knowledge production and team innovation.55, 56
MTT adaptive evolution
MTTs evolve and mature quite differently than traditional business teams. A considerable literature details specific stages and phases of business team maturation. While MTTs may progress through distinct phases, it is also likely that, because of the dynamism of translational goals, the requirements of scientific collaboration, and the time variance of MTT network collaborations, MTT team development will not be linear, and hence its development is not aligned with traditional business teams. Team development and evolution occurs as a result of time‐based adaptations as well as disruptive and revolutionary quantum changes. Here, science teams, such as MTTs, may experience long periods of inertia punctuated by disruptive change, such as radical changes in funding, or scientific breakthroughs. We postulate that MTTs exist in no less than four distinct phases or stages. Because of the degree of multidisciplinarity, changing membership, and contextual factors, we propose that MTTs are never at a state of full maturity, but rather are in a constant state of reconfiguration and redeployment (Figure 2). This model is quite distinct from that of an industry team, in which the product focus constrains the extent of reconfiguration. In an MTT, each stage may be completed, only to reenter a previously mastered stage due to changes in team project, structure, or goals.
Figure 2.
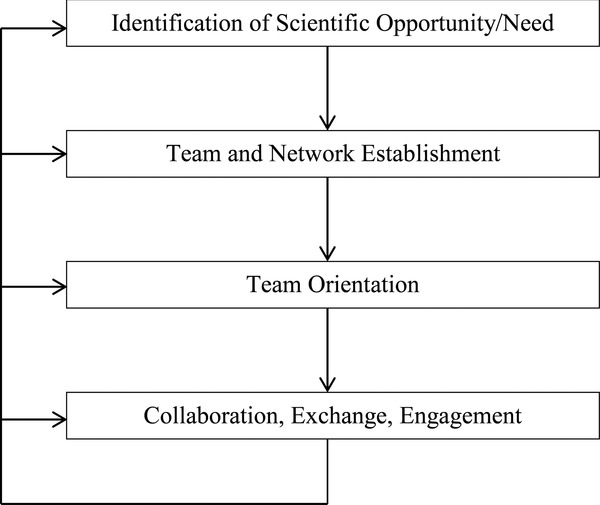
Developmental stages of MTTs. Shown are the major proposed stages of development for MTTs.
Hence, our model is a dynamic process beginning with identification of a translational science opportunity or need, followed by establishment of a strategic core and network collaborators, followed by team orientation (creation of identity, goals, roles, and structural agreements), and lastly by team collaboration, scientific exchange, and full engagement and productivity aligned with translational goals. Such dynamic stages have theoretical justification from the literature, as teams learn and evolve over time, and may require substantively different lengths of time to reach maturity.
Instantiation of MTTs at UTMB
Team design characteristics
Our literature analysis suggests that at least thirty team design characteristics are important to the function of MTTs. These features can be aggregated into the domains of context, tasks, membership, skill acquisition, team development, team structure, team processes, team reactions and affective states, team evolution and development, and team performance criteria (Table 3). An optimal MTT design will incorporate aspects of each of these domains (Table 4). To place the above discussion in practical terms, we will illustrate the UTMB environment for MTTs, how MTTs are operationalized and describe the development of two distinct MTTs as Case Illustrations.
Table 4.
Characteristics of an MTT. Implementation of MTTs requires elements of each of these attributes
| Characteristic | Attributes |
|---|---|
| Goals | Address issues related to human disease/ community health |
| Accomplish scientific tasks at an accelerated rate | |
| Expand scientific, educational and team‐based capabilities | |
| Develop team effectiveness through adaptation and learning | |
| Structure | Multidisciplinary membership |
| Formally designated roles | |
| Connection with internal and/or external research networks | |
| Process | Collaboration |
| Interdependence | |
| Autonomy and self‐selection | |
| Egalitarian governance | |
| Technological facilitation |
Contextual factors
Interdisciplinary research teams at UTMB predate the development of the NIH roadmap57 by over two decades. Accordingly, the academic context in which our MTTs were developed likely shares important features with other academic health centers. In the late 1980s, UTMB made the strategic decision to use institutional and foundation funds to develop and support thematically focused interdisciplinary research centers. Within each center, a core nucleus of scientists produce scientific discovery relevant to the center's focus. Research themes are identified by center faculty who develop consensus during research retreats and by identifying strategic opportunities. Resources are then used to recruit and develop additional faculty and for equipment for core laboratories within the center. Center members are jointly appointed in appropriate academic departments. Currently six active centers are supported by the university on topics such as Molecular Medicine (and Systems Biology), Environmental Health and Medicine, Structural Biology and Molecular Biophysics, Vaccine Development, Cancer and Cell Biology.
The Centers use the institutional funding to support successful new extramural funding in the form of multi‐investigator (P01 and Center) grants and to stimulate new innovative themes that can themselves become Centers. To support the Center model, the university has developed mechanisms for multiple (joint) center‐ and department affiliations that have resulted in a culture of multidisciplinary faculty collaborations. Because of the central role that Core Resource Laboratories played in Center operations, formal Academic Promotion and Tenure (APT) criteria were revised with specific wording for the evaluation of scholarly activities, which now includes specific criteria for independent scholarly and creative contributions, collaborative research accomplishments, and exceptional facilitation of the work of many others. This latter criterion is often accomplished by core resource support that is essential for translational research in biostatistics, genomics, proteomics, and bioinformatics.
Oversight and support for university‐wide core laboratories is by a broad‐based faculty committee (University Core Development Committee) that proactively assesses the needs for new technologies and encourages adoption of best practices. This process of multi‐investigator research initiated by Centers has created a fertile environment for developing MTTs.
Operationalizing MTTs in the UTMB CTSA
The UTMB center structure positioned the CTSA to apply the hybrid industry‐academic MTT model. The UTMB CTSA is organized into 12 Key Functions (Key Resources) linked by a central point of contact (Coordination Core). MTTs are competitively selected for CTSA support through peer review by our Scientific Review Committee. Review criteria include the theme, rigor of the proposed science, qualities of the principal investigator(s), projected impact of the translational project, and involvement of trainees (Table 5). MTTs are ultimately approved by our Executive Committee. Institutional structures that have broad based resources at other institutions could conceivably serve the infrastructural support needs that our CTSA provides.
Table 5.
Selection Criteria for MTTs
| Selection criteria | Characteristic |
|---|---|
| Research topic | University research strength or strategic priority |
| Leadership | Principal Investigator with national stature, including active NIH support |
| Translational project | Translational project that involves patient‐oriented research or a clinical intervention |
| Strategic core | Strategic core of multidisciplinary investigators that regularly interact/meet |
| Training/education | Assistant professors, fellows or predoctoral students embedded within the team |
Currently the CTSA portfolio includes 11 distinct MTTs with 119 members. A bipartite network was used to understand the range of disciplinarity and interconnection of the MTT membership (Figure 3). In this representation, the nodes represent 11 teams and 119 members, and edges between the nodes represent team membership. The colors of the nodes represented members’ departmental affiliations, and the diameter of each node was proportional to the number of connecting edges, so teams with many members were larger compared to those that had fewer members. Four teams in the center of the network shared four or more members, three teams shared at least two members, and two teams shared no members. The shared members were mostly researchers who specialized in methods (e.g., biostatistics, proteomics analysis), or CTSA leadership. Three teams were more homogenous in member affiliation compared to the rest. The overall observations led to the hypothesis that shared members could enhance interteam exchange of specialized technologies, or acquire new capabilities. Analysis of this network also suggested a correlation between team heterogeneity and the number of shared members. This depiction is a snapshot of a dynamic process, and ongoing assessment of our networks in relationship to objective metrics of team productivity will facilitate understanding the critical elements of team structure and function that predict research productivity.
Figure 3.
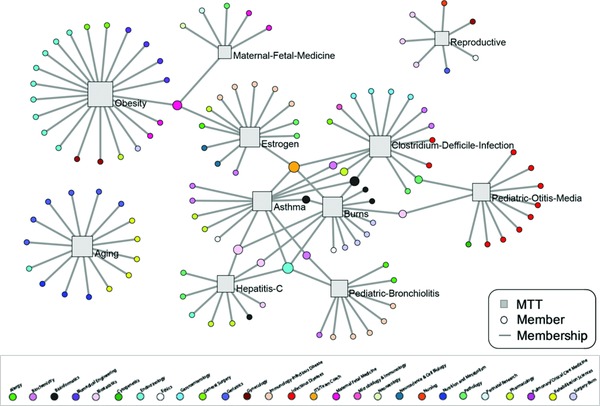
Disciplinarity in MTTs. Shown is a bipartite network of 11 translational teams and 119 members. The nodes were laid out using the Kamada Kawai algorithm suitable for mid‐sized networks in the range of 100 nodes. The algorithm pushes together nodes that share many connections, and pushes apart nodes that do not, resulting in a layout that approximates the relationship between nodes.
MTT–CTSA interactions: Utilization of key resources
After initiation, the MTT develops a shared vision, goal statement, and project description. Subsequently, the team meets with CTSA Operational leadership to determine which KRs are required to initiate the translational project. Although MTTs may have several active projects, typically only one active project is supported by the CTSA. The appropriate KR Directors are then assigned to interact with the MTT. The specific KRs engaged are dependent on the stage of the project development (schematically illustrated in Figure 4), and are expected to change over the life cycle of the MTT project. Evolving KR engagement is managed by the MTT leaders in conjunction with the CTSA Leadership (including the Coordination and Tracking and Evaluation KRs) based on analysis of milestones and outcomes.
Figure 4.
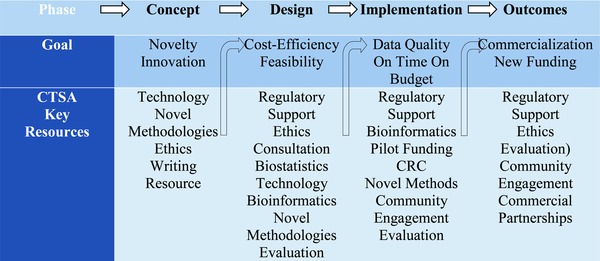
Development phases of a CTSA Translational Project. Shown are typical Key Resource needs for distinct stages of an MTT‐CTSA collaborative project.
We examined the utilization of 10 CTSA Key Resources by the 11 MTTs. In this analysis, the nodes represent 11 teams and 10 KRs, and the edges represent the KR utilization (Figure 5). The size of the KR nodes was proportional to the total time spent with each MTT (shown by the thickness of the edges connecting each MTT and KR), plus the total time spent for general activities such as infrastructure building that are useful across MTTs. The thickness of the edges connecting each KR‐MTT pair was proportional to the hours reported by each KR in support of the respective MTT. This analysis indicated that KR utilization varied along two dimensions: Frequency and Total Use. For example, the Coordination Core was utilized by all 11 MTTs, but the overall time spent across all MTTs was relatively small. In contrast, the Translational Technologies was used by 7 of the 11 MTTs, but its overall usage across those MTTs was high. Furthermore, there was a set of MTTs and KRs that formed an inner core representing high interaction characteristic of the needs of their translational project at their developmental stage. Projects early in development (Burns) required heavy use of biostatistics for clinical study design, whereas ongoing molecular‐based studies (Pediatric‐Bronchiolitis, Otitis Media, and Aging) required heavy use of the Translational Technologies KR.
Figure 5.
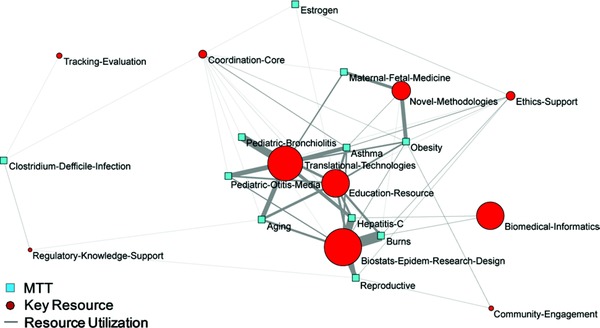
CTSA Key Resource Utilization by MTTs. Shown is a bipartite network of 11 MTTs and 10 Key Resources. The size of the KR nodes is proportional to the total time spent with each MTT (shown by the thickness of the edges connecting each MTT and KR), plus the total time spent for general activities such as infrastructure building that are useful across MTTs. The Clinical Research Center Key Resource, heavily used by one MTT, obscured the network analysis and was excluded from the visualization.
Case illustrations
Two MTTs are described, each entering at distinct developmental stages and requiring different CTSA Key Resources (Table 6, c.f. Figure 4).
Table 6.
Case Illustrations. Abbreviations of CTSA key resources used: BS = biostatistics; BioIT = bioinformatics; CC = coordination; ED = education; Edit = editorial support; Eth = ethics; NM = novel methodologies; Reg = regulatory; T&E = tracking and evaluation, TT = translational technologies
| Developmental Stage (Figure 2) | Severe Asthma – SAMTT | Clostridium difficile infection CDI‐MTT |
|---|---|---|
| Identification of Opportunity/Need | • Purpose: identify protein biomarker of severe asthma | • Purpose: develop novel therapeutic for CD infection/colitis |
| • Opportunity to leverage current UTMB assets by incorporating CTSA resources | • Basic science research in CD infection identified ‐mechanism of virulence | |
| • Molecular phenotyping is of considerable interest in academic asthma community | • Small molecule inhibitor of toxin defined | |
| • CTSA Help: Opportunity recognition | • CDI is important source of morbidity and mortality in USA and globally | |
| • CTSA KRs: CC, Pilot | • CTSA Help: guidance on MTT creation | |
| • CTSA KRs: CC | ||
| Team/Network Establishment | • Initiation: Working group in place; team development embryonic. | • Initiation: MTT goals established, and necessary expertise determined |
| • Team members with expertise in biostatistics, ethics, and informatics were added. | • Expertise in biostatistics, regulatory affairs, ethics, and clinical medicine, and trial design was embedded | |
| • Trainee positioned as project manager | • Team development had not begun | |
| • Team development coach necessary | • CTSA Help: Team development, logistics and scheduling; goal setting; leadership development | |
| • CTSA Help: Team development, trainees; goal setting; leadership development | • CTSA KRs: CC, Eth, BS, Reg, ED, NM, Pilot | |
| • CTSA KRs: CC, Eth, BS, ED | ||
| Team Orientation | • Barriers: Nonoverlapping expertise inhibited communication | • Barriers: New team required advice and support in many areas |
| • “Method Intuition” seminars to improve cross disciplinary communications | • TSA resources provided rapid start‐up of the MTT | |
| • Metrics, benchmarks, milestones | • Facilitated team development | |
| • CTSA Help: Logistics, scheduling, process | • Regulatory KR completed submission of a necessary IND | |
| • CTSA KRs: CC, BioIT, T&E, ED, Eth | • CTSA Help: Logistics, scheduling, | |
| • CTSA KRs: CC, Reg | ||
| Collaboration/ Exchange/Engagement | • Early outcomes: Two manuscripts published in field of molecular phenotyping | • Early Outcomes: Definition of S‐NO in toxin inactivation; Metabolomic analysis initiated as parallel project: identify metabolomic signature of CDI infection |
| • Incorporation of visual analytics added important mechanistic insights | • CTSA Help: Grant administration | |
| • CTSA Help: Edit | • CTSA KRs: CC, NM, TT | |
| • CTSA KRs: CC, BioIT, BS, |
The severe asthma MTT (SA‐MTT)
The SA‐MTT was formed upon CTSA funding by several existing, but independent research groups in airway inflammation. The translational goal of the SA‐MTT is to develop predictive protein biomarkers to advance personalized medicine in severe asthma.
The SA‐MTT strategic core began with a senior translational investigator as the team leader, a senior basic investigator, and a senior proteomics investigator as collaborating investigators, and a senior fellow in pulmonary medicine as a trainee. Biostatistics and ethics expertise from the CTSA key resources were included on initiation and other collaborators from each of the key areas were also invited to participate. Team meetings were scheduled on a recurring basis twice monthly. Initial work included developing a mutually agreeable team vision and goals, and establishing the framework for a new, multidisciplinary project. Once established, the vision and goals guided the discussion of the details of the project. Leadership development is an explicit goal of the MTT; consequently, we appointed a senior trainee (Clinical Fellow) as the Project Manager, whose responsibilities included confirming the logistics of meetings, maintaining agreed‐upon timelines for completion of work elements, leading team discussions, setting agenda and conducting specific aspects of the scientific program.
The involvement of the CTSA Bioinformatics KR enabled the SA‐MTT to identify proteomic signatures that correlate with important physiologic characteristics in asthma (eosinophilia, bronchodilator responsiveness to beta‐2 agonists, and methacholine responsiveness), and described four molecular phenotypes in our asthma subjects. Both of these papers were published in high profile peer‐reviewed journals.58, 59
With a new Bioinformatics resource developed by CTSA funding (the Discovery and Innovation through Visual Analytics Laboratory), the SA‐MTT used network analysis to reanalyze the proteomic signature data. Using these powerful approaches, 3 clusters of protein expression were identified, and associated with specific phenotypes of asthma, which provided important biological pathway information that was hitherto not evident. These observations have been also published in a high profile, peer‐reviewed journal.60 The impact of the CTSA was evident in that these insights would not otherwise have been generated.
The C. difficile infection MTT (CDI‐MTT)
The CDI‐MTT represented a new opportunity when a PhD‐trained investigator developed compelling new information regarding the molecular mechanisms by which Clostridium difficile infection causes colitis. Importantly, these mechanistic insights informed a strategy for developing novel therapeutic agents for this important disease. The purpose of the CDI MTT was to develop novel therapeutics strategies for clinical CDI, and test those strategies in appropriately designed clinical trials. However, efficiently moving the basic science concepts into a clinical realm was outside the current scope of expertise of the PI.
The team was initiated with a senior basic science investigator as the team leader, a clinical pathologist, and a gastrointestinal clinician as important members. Biostatistics and ethics expertise were included on initiation. Team meetings were scheduled on a recurring basis twice monthly, using the logistical support of the CTSA. Initial work included developing a mutually agreeable team vision and goals, and establishing the framework for a clinical trial. Once established, the vision and goals guided the discussion of the details of the project. As the planning for an intervention trial in CDI progressed, it became clear that the limited experience of the team with formal clinical trials had resulted in a trial design that failed to consider important complexities of diagnosis, treatment, and trial management.
As delays developed in initiating the trial, the team determined that another appropriate course of action was to expend resources towards developing a metabolomic profile that might predict recurrence of CDI. The development and analysis of a metabolomic dataset from patients with CDI has led to a provisional metabolomic panel which may have predictive capability for recurrence of CDI. In addition the CDI team incorporated a novel method for analysis of S‐nitrosylated proteins in host defense to the C. difficile enterotoxin that was developed and made available through the Translational Technologies Key Resource. This approach enabled the observation that host S‐nitrosylation is important in toxin inactivation, and resulted in a major publication61 that formed the basis for a newly funded RO1. From this experience, we learned that early incorporation of clinical trial expertise in an MTT project that might reasonably progress to a clinical trial within the time frame of the lifecycle of the proposed project would be useful. In addition, early incorporation of regulatory expertise to submit an investigational new drug application could accelerate the process.
Discussion and Lessons Learned
Increasing evidence confirms that the use of teams in science is productive.2, 3, 4, 6 As in other disciplines, much can be gained by employing best practices for effective team functioning. To achieve this goal, we have applied selected areas of team theory and practice to translational teams supported by an institutional framework, in our case, the CTSA.
Importance of defining team roles
Delineation of specific roles in teams is an important predictor of performance.47 Consequently, we have embedded in our MTT structures a strategic core of investigators which contains necessary multidisciplinary expertise. In our initial development of the SA‐MTT, we recognized that the PI is heavily time‐committed, and therefore may not be able to supervise multiple projects. Accordingly, we therefore developed the Project Manager role, to facilitate team progress and incorporate leadership training. This experience provides a framework to acquire team process core competencies established by the CTSA Education and Training Key Function Committee, but could be used to develop other important leadership skills.37 The project manager must have good interpersonal skills, be willing to develop team management skills, and be invested in the success of the team.
Knowledge communication and trust
Knowledge communication is an essential component of effective R&D, product, and virtual teams.62, 63 CTSAs can promote knowledge communication by providing informatics resources and infrastructure, such as Web‐accessible shared drives for data, and access to social networking tools, (formally adopted by the CTSA consortium). There is a strong positive relationship between trust and knowledge sharing for all types of teams.62 Trust amongst team members results in enhanced cooperation and acquisition of shared work values.64 Team trust coupled with emotional intelligence is promoted by regular interactions, appropriate recognition for team roles established through the formative stages of the MTT life cycle. As a result collaboration and team creativity is enhanced.65
To operationalize multidisciplinary communication within our SA‐MTT, we piloted a communications strategy called “methods intuition.” It had become apparent that team members were not familiar with the views, vocabulary, and common knowledge base of other disciplines within the team. For example, pulmonologist members performed invasive procedures, including bronchoscopy and bronchoalveolar lavage, but other members had such limited knowledge of the details that it inhibited substantive discussion. Analogously, many team members were not conversant in the technical specifics of proteomic analysis, or the intricacies of the ethical conduct of human research. The language, conceptual frameworks, and work flow were foreign. It became essential to develop effective cross‐disciplinary communication. Methods intuition focused on educating team members about the discipline‐specific terminologies used, the technical methodologies employed, and the kinds of inferences that can be drawn from that discipline.66 This activity significantly enhanced intra‐team communication and effectiveness.
MTT Disciplinarity
Because of the dynamic nature of discipline involvement in MTTs project evolution, we believe that multidisciplinarity is likely to be the most efficient structure for MTT organization. Our bipartite network depiction of disciplines represented in the UTMB MTTs was initially approached by an analysis of the primary departmental affiliations of the membership. From this analysis, several larger MTTs (aging, obesity) tended to have a more homogenous composition of 3–4 disciplines represented. By contrast, smaller or nascent MTTs (CDI‐MTT, SA‐MTT) were highly interconnected by several key disciplines. These highly connected components of the network tended to be represented by bioinformatics, and/or CTSA leadership (black circles, Figure 3). The cross‐MTT interactions may be opportunities for collaborations in new research domains. It will be of interest to follow the evolution of these highly connected MTTs to determine their productivity and trajectory.
CTSA impact on MTT innovation
The MTT construct provides its participants with unique opportunities for team science. First, dynamic team‐based systems can address the full range of expertise needed to span all phases of the translational domain. It is axiomatic that the full range of skills necessary for translational research spanning the T1‐T4 domains is rare in any single investigator.8 Appropriately composed, the strategic core of an MTT can contain the requisite skill sets for accomplishing T1 objectives, then can reform its skill sets as it transitions into a T2 domain by restructuring the MTT. Another facet of the MTT is enhanced influence in distinct disciplines. For example, the CTSA supported bioinformatics enabled the SA‐MTT to profiles of asthma phenotypes, contributing research papers in domains that would not have been possible otherwise. The formal MTT method intuition was an intervention to promote improved team communication and effectiveness. The method intuition approach was been shared throughout the CTSA MTT structure, to promote communication within other MTT strategic cores. Innovation in the CDI‐MTT was enhanced by access to novel proteomics technologies that enhanced discovery in mechanisms of host‐defense and potential mechanisms for translational therapy.
CTSA–MTT interactions
CTSA Key Resource utilization will depend on the developmental stage of the MTT Project (Figure 4). Hence, we recognize that the network representation of CTSA‐MTT interactions is a snapshot of a highly dynamic process. However, this shapshot informs optimal CTSA Key Resource configuration and size required to support MTT projects. The UTMB MTTs are primarily in T1 domain of the translational spectrum. Our analysis suggests that a cluster of Key Resources (biostatistics, translational technologies, and novel methodologies) are heavily involved at present in MTT projects, whereas other Key Resources (education, bioinformatics, CRC) are devoting significant time to the CTSA in terms of infrastructure development. In addition, the larger, independent MTTs from the discipline analysis (Figure 3) tended to consume a small subset of Key Resources. For example, the aging MTT primarily used the CRC and, to a lesser extent, translational technologies. Analysis of network depictions over time will inform dynamic right‐sizing of Key Resources as MTT projects evolve into T2 and T3 domain activities.
Education in the MTTs
Training in competencies required for translational research is one of the major goals of MTTs (Table 4). Within MTTs, early stage investigators, including junior faculty, research and clinical fellows, and graduate and medical students, are acquiring the scientific knowledge and skills of their individual disciplines, more specific skills needed by the MTT, and a broader set of competencies now expected of a translational researcher. Skills and competencies are acquired both from organized learning sessions and from ongoing experience. They are guided in these learning efforts by primary and secondary mentors who are members of their MTT, by team development coaches embedded in the CTSA, and by other faculty in their own disciplines. Their training includes undertaking a major role in a project within the MTT, which for students will relate course work to the scientific pursuits of the team. They also gain knowledge and experience in how teams function and learn the benefits of structured teamwork. They learn that functioning in a work silo is only one possible future scientific careers track, and that team‐based science may be more productive. They will incorporate advances in the field of team science and thereby understand that teams are subject to scientific study, and that individual activities within teams can be guided in a manner to achieve both scientific goals and career advancement. Conversely, they learn that a team project may fail due either to scientific issues or from problems with team relationships and functioning.
More generally, an MTT should provide a rich and unique educational environment for members at all levels. Effective team collaboration requires that each member learns to acknowledge the contributions of others, becomes conversant with other disciplines within the team, and contributes discipline‐specific knowledge. If this educational process is successful, all team members are more likely to work effectively toward clear and mutually agreed upon scientific goals. The process of educating each other in some aspects of their individual disciplines, using method intuition or other approaches, not only makes the team more productive, but also broadens scientific understanding and professional effectiveness of the individual team members. Thus, an MTT is an educational environment where junior and senior members from different disciplines can combine their skills and educate each other as they work on challenging and complex scientific problems. Members leaving a team are enriched by a more widely applicable fund of skills and knowledge and are better able to conduct team‐related work in the future.
Challenges and ongoing development
Both challenges and opportunities exist in the application of MTTs to translational science in AHCs. Formalized team training and team development increases team effectiveness,24, 67 and enhances innovation on team‐based projects.68 However, teams are somewhat contrary to traditional academic reward structures. Specific conceptual models of team maturity and adaptation are required, based on identifying team member skills, understanding development of new skills, metricating individual and team learning, and quantifying productivity.69, 70 A more prescriptive taxonomy of team based skills that is specific to team science would facilitate development of such models, but at present no consensus exists on this point. While general competencies have been developed,14 it will be necessary to define with more specificity the team‐related skills needed for success in both trainees and mature leaders.
Perhaps the greatest challenge involves the evaluation of team science in the context of a complex discipline, translational science. This issue is compounded by the fact that the evaluation of team science must occur at multiple levels, to include innovation, productivity, and pace of scientific discovery.1 Not only does team science present multiple evaluative difficulties, but its study is made more complex in that it must also address a long range clinical continuum representative of translational science, with outcomes that differ depending on the stage of translation.71 Thus, team structure, team processes, and team skills must be evaluated at multiple levels over long periods of time. While a sufficient number of general team effectiveness models exist,26, 27, 28, 29, 30, 31, 32, 34 team effectiveness models for translational science will need to be developed.
Strengths and Limitations of the MTT approach
Several strengths of our approach are notable. Clearly, conducting translational research, from T1 to T4, requires skills that are only rarely held by a single investigator, necessitating contributions by multiple investigators in distinct disciplines. In fact, even projects constrained within a single translational dimension are improved by multidisciplinarity. The MTT benefits both from complementarity of expertise of investigators from different disciplines, which promotes innovation and creativity, and also from overlap of expertise, which provides functional redundancy that reduces the likelihood that a complex project will halt due to the unavailability of a single team member. Goals that are developed and endorsed within the team have broader applicability, and increased significance and impact. Membership from several disciplines makes more likely that multiple publications from a single project, each focused on a particular discipline, will be produced, enhancing productivity. For example, the SA‐MTT has publications in clinical immunology, collaborative science, and information manangement journals, at least two of which would not have been written had the team not existed. The formal incorporation of trainees and leadership development processes promotes individual career skills development and facilitates the functioning of the team. Project management processes, adapted from the business community, bring temporal and task accountability to the team, avoiding unnecessary delays in the project. Periodic milestone assessment permits the team and its manager to identify bottlenecks and other obstacles, and inform the application of resources to mitigate or eliminate the hindrances. We postulate, but have not yet shown, that these advantages will result in increased innovation, accelerated scientific discovery, and faster reduction to practice.
The MTT structure does entail increased complexity, and a greater “process focus” than is common in AHC or traditional laboratory groups. This increased complexity translates to a greater initial investment of time and intellectual effort to instantiate a team and define its project. Conflict resolution skills, which in an hierarchical group are less frequently required, are not infrequently needed, as a wider variety of stakeholder views must be reconciled. There is a learning curve for senior investigators, accustomed to an autocratic reporting structure, to adapt to a distributed authority model. We anticipate that some investigators may not be able to make this transition effectively. Identifying these investigators and developing interventions that improve team skills may have great value to enhance the translational product pipeline.
Summary
Based within an academic healthcare environment with missions to generate knowledge, provide education and training, and care for patients, MTTs are tasked with developing translational products and accelerating the pace of scientific discovery that will positively impact human health. In this context, MTTs represent a unique, hybrid form of team organization. In this Special Report, we describe the adaptation of business and organizational principles to the development of MTTs and illustrated how the CTSA structure specifically can be used to further this purpose. More work will be required to identify the best mechanisms for fostering transformative leadership, evaluating team performance, and measuring the impact of translational science on human health.
Supporting information
Disclaimer: Supplementary materials have been peer‐reviewed but not copyedited.
Supporting Information
Acknowledgments
The authors would like to thank Drs. Robert M. Rose and Bill T Ameredes for helpful discussions, Lori Wiseman for programmatic coordination and the UTMB MTT leaders for their commitment to the CTSA MTT project. The authors are thankful to Karen Pierson and Lisa Velasquez for the tracking and evaluation data that made the network analysis possible. This research was supported by the National Institutes of Health, CTSA, and the Institute for Translational Sciences at the University of Texas Medical Branch at Galveston: 1UL1RR029876 UTMB CTSA (ARB).
References
- 1. Borner K, Contractor N, Falk‐Krzesinski HJ, Fiore SM, Hall, KL , Keyton, J , Spring B, Stokols D, Trochim W, Uzzi B. A multi‐level systems perspective for the science of team science. Sci Translat Med. 2010; 2(49): 49cm24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Jones BF, Wuchty S, Uzzi B. Multi‐university research teams: shifting impact, geography, and stratification in science. Science. 2008; 322(5905): 1259–1262. [DOI] [PubMed] [Google Scholar]
- 3. Wuchty S, Jones BF, Uzzi B. The increasing dominance of teams in production of knowledge. Science. 2007; 316(5827): 1036–1039. [DOI] [PubMed] [Google Scholar]
- 4. Adams JD, Black GC, Clemmons JR, Stephan PE. Scientific teams and institutional collaborations: evidence from U.S. universities, 1981–1999. Res Pol. 2005; 34(3): 259–285. [Google Scholar]
- 5. Choi BC, Pak AW. Multidisciplinarity, interdisciplinarity, and transdisciplinarity in health research, services, education and policy. Part 2. Promotors, barriers, and strategies of enhancement. Clin Invest Med. Medecine clinique et experimentale. 2007; 30(6): E224–232. [DOI] [PubMed] [Google Scholar]
- 6. Fiore SM. Interdisciplinarity as teamwork. Small Group Res. 2008; 39(3): 251–277. [Google Scholar]
- 7. Disis ML, Slattery JT. The road we must take: multidisciplinary team science. Sci. Translat. Med. 2010; 2(22): 22cm29. [DOI] [PubMed] [Google Scholar]
- 8. Woolf SH. The meaning of translational research and why it matters. JAMA. 2008; 299(2): 211–213. [DOI] [PubMed] [Google Scholar]
- 9. Sung NS, Crowley WF, Jr , Genel M, Salber P, Sandy L, Sherwood LM, Johnson, SB , Catanese V, Tilson, H , Getz K, Larson EL, et al. Central challenges facing the national clinical research enterprise. JAMA. 2003; 289(10): 1278–1287. [DOI] [PubMed] [Google Scholar]
- 10. Westfall JM, Mold J, Fagnan L. Practice‐based research–”Blue Highways” on the NIH roadmap. JAMA. 2007; 297(4): 403–406. [DOI] [PubMed] [Google Scholar]
- 11. Falk‐Krzesinski HJ, Borner K, Contractor N, Fiore SM, Hall KL, Keyton J, Spring B, Stokols D, Trochim W, Uzzi B. Advancing the science of team science. Clin Translat Sci. 2010; 3(5): 263–266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hall KL, Feng AX, Moser RP, Stokols D, Taylor BK. Moving the science of team science forward: collaboration and creativity. Am J Prevent Med. 2008; 35(2 Suppl): S243–249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Stokols D, Misra S, Moser RP, Hall KL, Taylor BK. The ecology of team science: understanding contextual influences on transdisciplinary collaboration. Am J Prevent Med. 2008; 35(2 Suppl): S96–115. [DOI] [PubMed] [Google Scholar]
- 14. Bennett LM, Gadlin H, Levine‐finley S. Collaboration and Team Science: A field guide. 2010. https://ccrod.cancer.gov/confluence/download/attachments/47284665/TeamScience_FieldGuide.pdf?version=1&modificationDate=1271730182423
- 15. Masse LC, Moser RP, Stokols D, Taylor BK, Marcus SE, Morgan GD, Hall KL, Croyle RT, Trochim WM. Measuring collaboration and transdisciplinary integration in team science. Am J Prevent Med. 2008; 35(2 Suppl): S151–160. [DOI] [PubMed] [Google Scholar]
- 16. Isohanni M, Isohanni I, Veijola J. How should a scientific team be effectively formed and managed. Nord J Psychiatry. 2002; 56(2): 157–162. [DOI] [PubMed] [Google Scholar]
- 17. Rubio DM, Schoenbaum EE, Lee LS, Schteingart DE, Marantz PR, Anderson KE, Platt LD, Baez A, Esposito K. Defining translational research: implications for training. Acad Med: J Assoc Am Med Colleges. 2010; 85(3): 470–475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. McGuire DB. Building and maintaining a multidisciplinary research team. Alzheimers Dis Assoc Disord. 1999; 13(1): S17–S21. [DOI] [PubMed] [Google Scholar]
- 19. Aboelela SW, Larson E, Bakken S, Carrasquillo O, Formicola A, Glied SA, Haas J, Gebbie KM. Defining interdisciplinary research: conclusions from a critical review of the literature. Health Serv Res. 2007; 42(1p1): 329–346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Fennell ML, Prabhu Das I, Clauser S, Petrelli N, Salner A. The organization of multidisciplinary care teams: modeling internal and external influences on cancer care quality. JNCI Monogr. 2010(40): 72–80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lemieux‐Charles L, McGuire WL. What do we know about health care team effectiveness? A review of the literature. Medical Care Research and Review : MCRR. 2006; 63(3): 263–300. [DOI] [PubMed] [Google Scholar]
- 22. Delva D, Jamieson M, Lemieux M. Team effectiveness in academic primary health care teams. J Interprof Care. 2008; 22(6): 598–611. [DOI] [PubMed] [Google Scholar]
- 23. Korner M. Interprofessional teamwork in medical rehabilitation: a comparison of multidisciplinary and interdisciplinary team approach. Clin Rehabil. 2010; 24(8): 745–755. [DOI] [PubMed] [Google Scholar]
- 24. Buljac‐Samardzic M, Dekker‐van Doorn CM, van Wijngaarden JD, van Wijk KP. Interventions to improve team effectiveness: a systematic review. Health Pol. 2010; 94(3): 183–195. [DOI] [PubMed] [Google Scholar]
- 25. Naylor MD, Feldman PH, Keating S, Koren MJ, Kurtzman ET, Maccoy MC, Krakauer R. Translating research into practice: transitional care for older adults. J Evaluat Clin Pract. 2009; 15(6): 1164–1170. [DOI] [PubMed] [Google Scholar]
- 26. Cohen SG, Bailey DE. What makes teams work: group effectiveness research from the shop floor to the executive level. J Manag. 1997; 23(3): 239–290. [Google Scholar]
- 27. Hackman JR. The design of work teams In: Lorsch JW, ed. Handbook of Organizational Behavior. Englewood Cliffs, NJ: Prentice‐Hall; 1987: 315–342. [Google Scholar]
- 28. Gladstein D. Groups in context: a model of task group effectiveness. Admin Sci Quart. 1984; 29(4): 499–517. [Google Scholar]
- 29. Sundstrom E, DeMuse KP, Futrall D. Work teams: applications and effectiveness. Am Psychol. 1990; 45(2): 120–133. [Google Scholar]
- 30. Guzzo RA, Dickson MW. Teams in organizations: recent research on performance and effectiveness. Ann Rev Psychol. 1996; 47: 307–338. [DOI] [PubMed] [Google Scholar]
- 31. Kozlowski SWJ, Ilgen DR. Enhacing the effectiveness of work groups and teams. Psychol Sci Pub Interest. 2006; 7(3): 77–124. [DOI] [PubMed] [Google Scholar]
- 32. Ilgen DR, Hollenbeck JR, Johnson M, Jundt D. Teams in organizations: from input‐process‐output models to IMOI models. Ann Rev Psychol. 2005; 56: 517–543. [DOI] [PubMed] [Google Scholar]
- 33. Marks MA, Mathieu JE, Zaccaro SJ. A temporally based framework and taxonomy of team processes. Acad Manag Rev. 2001; 26(3): 356–376. [Google Scholar]
- 34. Mathieu J, Maynard MT, Rapp T, Gilson L. Team effectiveness 1997–2007: a review of recent advancements and a glimpse into the future. J Manag. 2008; 34(3): 410–476. [Google Scholar]
- 35. Bullinger HJ, Warschat J, Fischer D. Rapid product development—an overview. Comput Ind. 2000; 42(2–3): 99–108. [Google Scholar]
- 36. Harmancioglu N, McNally RC, Calantone RJ, Durmusoglu SS. Your new product development (NPD) is only as good as your process: an exploratory analysis of new NPD process design and implementation. R&D Manag. 2007; 37(5): 399–424. [Google Scholar]
- 37. Committee CEKF. Core competencies in clinical and translational sciences. 2011. https://www.ctsacentral.org/core‐competencies‐clinical‐and‐translational‐research.
- 38. Hirschfeld RR, Jordan MH, Feild HS, Giles WF, Armenakis AA. Becoming team players: team members’ mastery of teamwork knowledge as a predictor of team task proficiency and observed teamwork effectiveness. J Appl Psychol 2006; 91(2): 467–474. [DOI] [PubMed] [Google Scholar]
- 39. Volpe CE, Cannon‐Bowers JA, Salas E, Spector PE. The impact of cross‐training on team functioning: an empirical investigation. Human Factors: J Human Factors Ergonom Soc. 1996; 38(1): 87–100. [DOI] [PubMed] [Google Scholar]
- 40. Salas E, Rozell D, Mullen B, Driskell JE. The effect of team building on performance. Small Group Res. 1999; 30(3): 309–329. [Google Scholar]
- 41. Burke CS, Stagl KC, Salas E, Pierce L, Kendall D. Understanding team adaptation: a conceptual analysis and model. J Appl Psychol. 2006; 91(6): 1189–1207. [DOI] [PubMed] [Google Scholar]
- 42. Savelsbergh CMJH, van der Heijden BIJM, Poell RF. The development and empirical validation of a multidimensional measurement instrument for team learning behaviors. Small Group Res. 2009; 40(5): 578–607. [Google Scholar]
- 43. Wong S‐S. Distal and local group learning: performance trade‐offs and tensions. Organ Sci. 2004; 15(6): 645–656. [Google Scholar]
- 44. Van der Vegt GS, Janssen O. Joint impact of interdependence and group diversity on innovation. J Manage. 2003; 29(5): 729–751. [Google Scholar]
- 45. Fay D, Borrill C, Amir Z, Haward R, West MA. Getting the most out of multidisciplinary teams: A multi‐sample study of team innovation in health care. J Occup Organ Psychol. 2006; 79(4): 553–567. [Google Scholar]
- 46. Jin L, Sun H. The effect of researchers’ interdisciplinary characteristics on team innovation performance: evidence from university R&D teams in China. Int. J. Human Res. Manag. 2010; 21(13): 2488–2502. [Google Scholar]
- 47. Humphrey SE, Morgeson FP, Mannor MJ. Developing a theory of the strategic core of teams: a role composition model of team performance. J Appl Psychol. 2009; 94(1): 48–61. [DOI] [PubMed] [Google Scholar]
- 48. LePine JA, Piccolo RF, Jackson CL, Mathieu JE, Saul JR. A meta‐analysis of teamwork processes: tests of a multidimensional model and relationships with team effectiveness criteria. Personnel Psychol. 2008; 61(2): 273–307. [Google Scholar]
- 49. Marks MA, Mathieu JE, Zaccaro SJ. A temporally based framework and taxonomy of team processes. Acad Manag. Rev. 2001; 26(3): 356–376. [Google Scholar]
- 50. Cummings JN, Kiesler S. Collaborative research across disciplinary and organizational boundaries. Soc. Stud. Sci. 2005; 35(5): 703–722. [Google Scholar]
- 51. Gully SM, Incalcaterra KA, Joshi A, Beaubien JM. A meta‐analysis of team‐efficacy, potency, and performance: interdependence and level of analysis as moderators of observed relationships. J Appl Psychol. 2002; 87(5): 819–832. [DOI] [PubMed] [Google Scholar]
- 52. Glynn MA, Kazanjian R, Drazin R. Fostering innovation in complex product development settings: The role of team member identity and interteam interdependence. J Product Innovat Manag. 2010; 27(7): 1082–1095. [Google Scholar]
- 53. Wageman R. How leaders foster self‐managing team effectiveness: design choices versus hands‐on coaching. Organ Sci. 2001; 12(5): 559–577. [Google Scholar]
- 54. Elkins T, Keller RT. Leadership in research and development organizations: a literature review and conceptual framework. Leadership Quart. 2003; 14(4–5): 587–606. [Google Scholar]
- 55. Wang S, Noe RA. Knowledge sharing: A review and directions for future research. Hum Resour Manage R. 2010; 20(2): 115–131. [Google Scholar]
- 56. Kerr DS, Murthy US. Divergent and convergent idea generation in teams: a comparison of computer‐mediated and face‐to‐face communication. Group Decis Negot. 2004; 13(4): 381–399. [Google Scholar]
- 57. Zerhouni EA. Clinical research at a crossroads: The NIH roadmap. J. Investigat. Med.: Official Publication of the American Federation for Clinical Research. 2006; 54(4): 171–173. [DOI] [PubMed] [Google Scholar]
- 58. Brasier AR, Victor S, Boetticher G, Ju H, Lee C, Bleecker ER, Castro M, Busse WW, Calhoun WJ. Molecular phenotyping of severe asthma using pattern recognition of bronchoalveolar lavage‐derived cytokines. J Allergy Clin Immunol. 2008; 121(1): 30–37 e36. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59. Brasier AR, Victor S, Ju H, Busse WW, Curran‐Everett D, Bleecker ER, Castro M, Chung KF, Gaston B, Israel E, et al. Predicting intermediate phenotypes in asthma using bronchoalveolar lavage‐derived cytokines. Clin Translat Sci. 2010; 3(4): 147–157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60. Bhavnani SK, Victor S, Calhoun WJ, Busse WW, Bleecker ER, Castro M, Ju H, Pillai R, Oezguean N, Bellala G, Brasier AR. How cytokines co‐occur across asthma patients: from bipartite network analysis to a molecular‐based classification. J Biomed Informat. 2011; 44(Suppl 1): S24–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Savidge TC, Urvil P, Oezguen N, Ali K, Choudhury A, Acharya V, Pinchuk I, Torres AG, English RD, Wiktorowicz JE, et al. Host S‐nitrosylation inhibits clostridial small molecule‐activated glucosylating toxins. Nature Med. 2011; 17(9): 1136–1141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62. Linlin J, Haifa S. The effect of researchers’ interdisciplinary characteristics on team innovation performance: evidence from university R&D teams in China. Int J Human Res Manag. 2011; 21(3): 2488–2502. [Google Scholar]
- 63. Staples DS, Webster J. Exploring the effects of trust, task interdependence and virtualness on knowledge sharing in teams. Informat Syst J. 2008; 18(6): 617–640. [Google Scholar]
- 64. Chou LF, Wang AC, Wang TYT, Huang MP, Cheng B. Shared work values and team member effectiveness: the mediation of trustfulness and trustworthiness. Hum Relat. 2008; 61(12): 1713–1742. [Google Scholar]
- 65. Barczak G, Lassk F, Mulki J. Antecedents of team creativity: An examination of team emotional intelligence, team trust, and collaboration culture. Creativ Innovat. 2010; 19(4): 332–345. [Google Scholar]
- 66. Bhavnani SK, Farroni J, Crowder J, McKinney EB, Pillai R, Calhoun WJ, Rose RM, Carter MA. The role of method intuition in translational ethics. Proceedings of AMIA Summit on Translational Bioinformatics. 2012: pg. 141 http://proceedings.amia.org/2351e5/2351e5/1
- 67. Tannenbaum SI, Beard RL, Salas E. Team building and its influence on team effectiveness: an examination of conceptual and empirical development In: Kelly K, ed. Issues, Theory, and Research in Industrial/Organizational Psychology. Amsterdam: Elsevier Science Publishers BV; 1992: 117–154. [Google Scholar]
- 68. Hoegl M, Gemeunden HG. Teamwork quality and the success of innovative projects: A theoretical concept and empirical evidence. Organizat Sci. 2001; 12(4): 435–449. [Google Scholar]
- 69. Morgan BB, Salas E, Glickman AS. An analysis of team evolution and maturation. J Gen Psychol. 1994; 120(3): 227–291. [Google Scholar]
- 70. Arrow H, Henry KB, Poole MS, Wheelan S, Moreland RL. Traces, trajectories and timing: the temporal perspective of groups In: Poole MS, Hollingshead AB, eds. Theories of Small Groups: Interdisciplinary Perspectives. Thousand Oaks, CA: Sage; 2005: 313–368. [Google Scholar]
- 71. Trochim W, Kane C, Graham MJ, Pincus HA. Evaluating translational research: a process marker model. Clin Translat Sci. 2011; 4(3): 153–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Disclaimer: Supplementary materials have been peer‐reviewed but not copyedited.
Supporting Information