

Abstract
This study was conducted to assess the ability of two-dimensional tissue tracking (2DTT) to evaluate changes in left ventricular (LV) myocardial function associated with sustained high electrical pacing. Pacemakers were implanted at the right ventricular (RV) apex of five female Beagles, and sustained high electrical pacing of 250 beats per minute (bpm) was performed for three consecutive weeks. Conventional echocardiography and 2DTT were performed at baseline, and at every week for three weeks with pacing. The baseline parameters were then compared to those of weeks 1, 2, and 3. Three weeks of pacing resulted in significant reduction of radial and circumferential global strains (p < 0.001). Regional analysis revealed reduction of segmental strains in both radial and circumferential directions, as well as increased dyssynchrony after three weeks of pacing in the radial direction (p = 0.0007). The results of this study revealed the ability of 2DTT to measure radial and circumferential strains in dogs with sustained high-electrical pacing, and allowed assessment of global and regional myocardial function and the degree of dyssynchrony.
Keywords: cardiology, dog, echocardiography, experimental animal model, myocardial failure
Introduction
Sustained high electrical pacing has been shown to produce dilated, congestive cardiomyopathy in dogs, and this canine tachycardia-induced myocardial dysfunction model has been widely used to investigate congestive heart failure [22,28,29,31]. Evaluation of the myocardial function of these models has been of great interest because they enable better understanding of myocardial disorders such as dilated cardiomyopathy.
Standard transthoracic echocardiography is a non-invasive method of assessing cardiac function that has become one of the most important diagnostic tools for cardiovascular disorders [5,6,13]. Commonly used conventional echocardiographic parameters for the assessment of left ventricular (LV) myocardial function are obtained from M-mode measurements, and these include LV chamber dimensions and fractional shortening (FS) [5,13]. However, FS may not reflect true global function since it is a measurement of two specific LV segments, the anteroseptal and posterior segments, and it only assesses radial deformation [3,18,20,23]. In addition, LV function is influenced by a number of factors, including regional myocardial functionand ventricular synchrony, which cannot be completely assessed based on conventional parameters alone [21].
Two-dimensional tissue tracking (2DTT) is a relatively new echocardiographic technique that provides a novel approach to the assessment of myocardial function [14,17,23]. 2DTT is based on the formation of 'speckles' caused by reflection, scattering, and interference between tissue and ultrasound beams in the standard gray scale, two-dimensional echocardiographic images [3,8,10,11,14,16,17,20,21]. Tracking these speckles from one frame to another enables analysis of myocardial movement throughout the entire cardiac cycle and calculation of strain, which is a measurement of deformation of the myocardium over time expressed as the percent change from the original [3,8,10,11,14,17,18,20,21]. Advantages of 2DTT include simultaneous evaluation of global and regional myocardial function independent of the angle of insonation and cardiac translational movement and analysis of myocardial deformation in three spatial directions [3,10,14,17].
The ability of 2DTT to evaluate the LV myocardial function associated with sustained high electrical pacing has not yet been assessed. Therefore, this study was conducted to investigate the ability of 2DTT to evaluate (1) global myocardial function, (2) regional myocardial function, and (3) the degree of dyssynchrony in the canine tachycardia induced myocardial dysfunction model.
Materials and Methods
Animals
This study was carried out in accordance with the standards established by the Tokyo University of Agriculture and Technology and its Guide for the Care and Use of Laboratory Animals. All experimental procedures were approved by the Animal Experimental Committee of Tokyo University of Agriculture and Technology (acceptance no. 21-30). Five female Beagles approximately one year of age were used. The dogs had body condition scores of 4 to 6 out of 9, and their body weights ranged from 8.75 to 10.00 kg. All dogs underwent complete physical examination, blood count and plasma biochemical analysis, electrocardiography, blood pressure monitoring, radiography, and echocardiography prior to initiating the study to rule out the presence of any abnormalities.
Study design
Thoracotomy was performed on each dog for the implantation of an epicardial pacemaker at the right ventricular (RV)apex, after which sustained high electrical pacing of 250 beats per minute (bpm) was applied for three consecutive weeks. For each dog, an oscillometric blood pressure (BP) exam (BP-100D, FUKUDA M.E KOGYO, Japan), standard 6-lead electrocardiogram (ECG) (α8000, FUKUDA M.E KOGYO), and conventional and 2DTT echocardiography were performed at the baseline and weeks 1, 2, and 3 of pacing. The entire examination was performed during a temporary cessation of pacing, at which time the pacemaker was turned off for at least an hour. All pacemakers were checked for accurate pacing at the end of the each examination.
Instrumentation
The dogs were pre-medicated with subcutaneous administration of atropine andintravenous buprenorphine and midazolam, after which anesthesia was induced with intravenous propofol and general anesthesia was maintained by the inhalation of isoflurane. Thoracotomy was performed under general anesthesia with the dogs positioned on the right lateral recumbency via an incision made at the fourth intercostal space. The heart was exposed through pericardectomy, after which the pacemaker electrode (TF204-062, KMY Medical, Japan) was implanted at the RV apex. The lead was then tunneled to the back and exited immediately ventral to the vertebral process, where it was connected to a pulse generator (EV4543, Pace Medical, USA). After recovery from general anesthesia, dogs were returned to a post-surgical care facility, where they received a standard diet and free access to water. Following surgery, all the dogs were given a week of recovery period before initiating the pacing.
Echocardiography
An ultrasonography unit (ALOKA prosoundα 10; Aloka, Japan) equipped with a 5 MHz phased array transducer probe (UST52108; Aloka) was used for all echocardiographic examinations, which were performed with concurrent ECG monitoring by the same trained examiner for all dogs. All examinations were performed on awake dogs, using only gentle restraint. A mean of three measurements of each parameter was obtained from three consecutive cardiac cycles.
Conventional echocardiography
LV measurements were taken from the right parasternal short axis view at the level of the papillary muscle using M-mode. Measurements included LV end-diastolic (LVIDd) and end-systolic (LVIDs) diameters, LV free wall thickness in diastole (LVPWd) and in systole (LVPWs), interventricular septal thickness in diastole (IVSd) and in systole (IVSs), and FS.
The percentage of wall thickening of the interventricular septum (IVS) and left ventricular free wall (LVFW), which is a parameter of regional contractility of the myocardium evaluated by the changes in wall thickening, were calculated as: (systolic thickness - diastolic thickness)/(diastolic thickness) × 100. Additionally, diastolic parameters including early (E) and late (A) ventricular filling velocity, E/A ratio, and deceleration time were obtained from the trans-mitral flow profile at the left parasternal apical four chamber view.
Two-dimensional tissue tracking
The right parasternal short axis view at the level of the papillary muscle with a rate of 70~110 frames/s was acquired and saved onto a hard disk and then analyzed off-line (DAS-RS1 software 1.1v; Aloka). The observer was unaware of the measurements of conventional parameters while analyzing the strain measurements. Strain analysis involved multiple steps. Initially, the endocardium and the epicardium were manually traced at the end-systole by placing a number of points at the borders of the myocardium. The software then automatically tracked these points on a frame-by-frame basis, after which it divided the LV into six segments (anterior, lateral, posterior, inferior, septal, and anterior septal). Regional peak systolic strains of the six segments and global peak systolic strains, which were the mean of the six segments, were calculated for both the radial and circumferential directions. LV synchrony was also assessed by calculating the synchrony time index (STI), which is the difference in timing of peak strains from the earliest to the latest segments.
Statistical analysis
Statistical analyses were performed using statistical software (Prism 5.0v; GraphPad Software, USA and JMP 10.0.2; SAS Institute, USA). Parameters including conventional and 2DTT data were tested for normality and sphericity. The normality of distribution was testedusing the Kolmogorov-Smirnov test and a visual inspection of histograms, and normally distributed variables were expressed as the mean ± standard deviation. The Mauchly test was used to investigate the assumption of sphericity. These parameters were then evaluated for any significant changes between baseline and weeks 1, 2, and 3 using one-way repeated-measures ANOVA. The effectiveness of matching for the repeated measure was tested using an F test. When a significant difference was detected, further testing was performed using Dunnett's multiple comparison tests to compare the baseline measurements with weeks 1, 2, and 3. Significant differences was defined as p < 0.05.
Results
Pacemaker implantation was successful and recovery was uneventful in all five dogs. Additionally, all dogs were able to maintain adequate physical condition and survived until the last day of pacing. The measured conventional echocardiographic and 2DTT parameters are shown in Table 1. The resting heart rate with cessation of pacing at each examination revealed no significant changes from the baseline (p = 0.35). BP measurements showed declining trends, but significant differences were only observed between the mean and diastolic BP (p = 0.0035 and 0.0067, respectively). No abnormalities on the ECG were observed during any examinations.
Table 1.
Characteristics of physiological data, blood pressure parameters, conventional echocardiographic parameters and two-dimensional tissue tracking parameters, expressed as the mean ± standard deviation
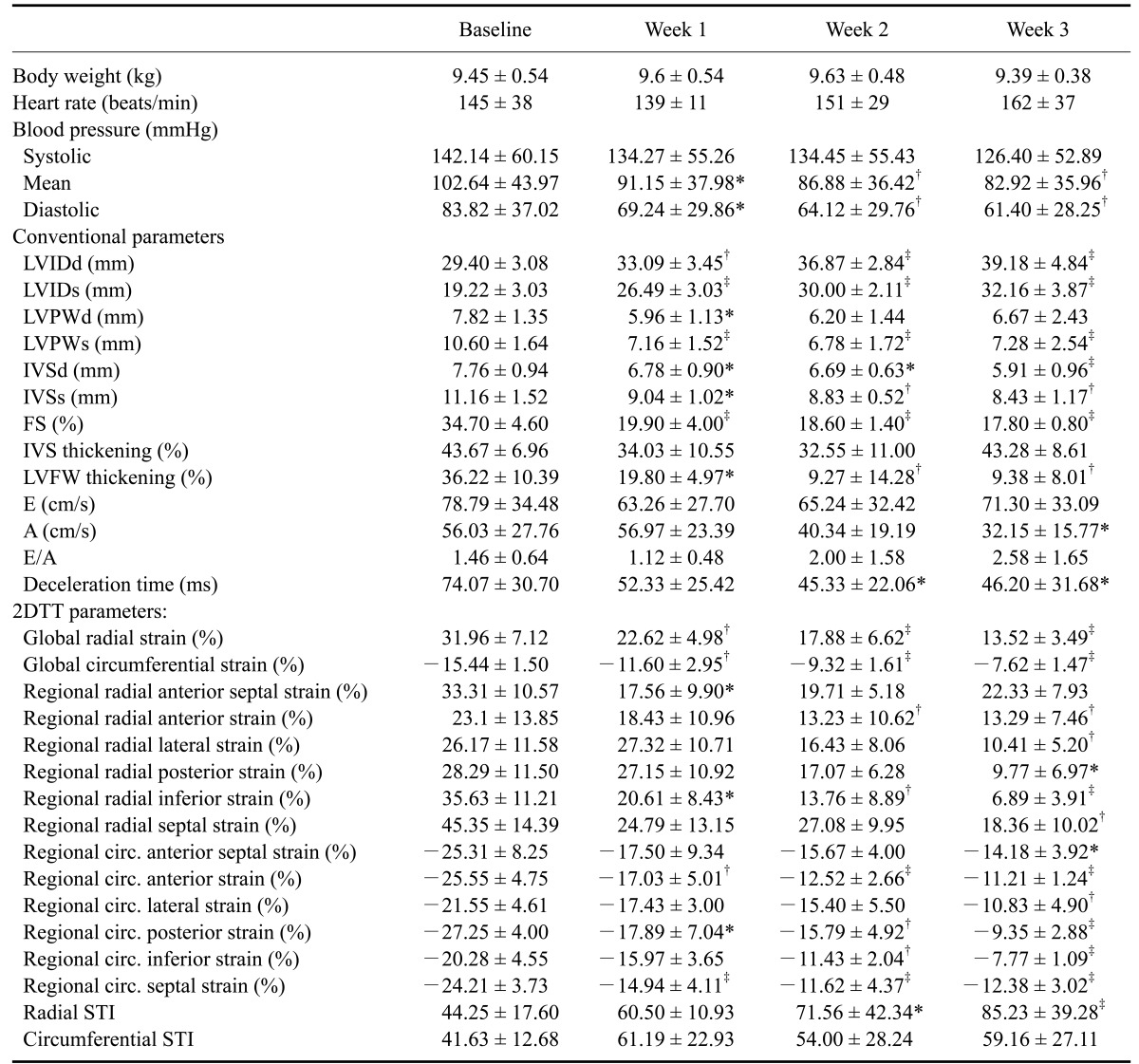
*p < 0.05, †p < 0.01, ‡p < 0.001 versus corresponding baseline values.
M-mode variables including diastolic and systolic IVS (p = 0.001 and 0.0028, respectively), LVID (p < 0.0001 for both), and LDPW (p = 0.0586 and 0.0001, respectively) revealed significant differences from week 1 of pacing. Pacing also resulted in significant differences in FS from week 1 (p < 0.001). Reduced percent wall thickening was observed at IVS and LVPW; however, significant differences were only observed with LVPW from week 1 of pacing (p = 0.0004). Among parameters describing diastolic function, only A (p = 0.0214) differed significantly at week 3, while deceleration time (p = 0.0198) showed a significant difference from week 2 of pacing.
Fig. 1 shows examples of radial and circumferential strains at baseline and week 3 of pacing. Compared to the baseline, pacing caused a significant reduction of both global radial and circumferential strains from week 1 (p < 0.0001 for both) (Fig. 2). Regionally, in the radial direction, the inferior segment showed significant changes of strain from week 1, the anterior segment showed significant changes from week 2, and the lateral, posterior, and septal segments showed significant changes at week 3. The anterior septal segment only showed significant changes of strain at week 1. Conversely, all of the segments in the circumferential direction revealed significant changes by the third week of pacing. The anterior, posterior and septal segments showed significant changes of strain from week 1, while the inferior segment showed significant changes from week 2, and the anterior septal and lateral segments showed significant changes at week 3. The STI values of the radial strains revealed significant increases from week 2, whereas no significant changes were observed in the circumferential strains (Fig. 3).
Fig. 1.

Examples of radial and circumferential strain profiles obtained from the right parasternal short axis view at the level of the papillary muscle using two-dimensional tissue tracking. Radial strain represents thickening and thinning motion of the myocardium in the radial direction, and circumferential strain represents myocardial motion along the circular perimeter. In the systole, the myocardial deformation increases in the radial direction, thus the radial strain becomes positive, and the myocardial deformation decreases in the circumferential direction, causing the circumferential direction to becomes negative. Radial (A) and circumferential (B) strains at baseline, and radial (C) and circumferential (D) strains at week 3 of sustained high electrical pacing.
Fig. 2.

Mean ± standard deviation values of global radial (A) and circumferential (B) strains plotted against time. Compared with baseline, †p < 0.01, ‡p <0.001 (ANOVA-Dunnet's post test).
Fig. 3.

Mean ± standard deviation values of radial (A) and circumferential (B) synchrony time index, which is the indicator used to assess the degree of dyssynchrony. Significant differences determined by Dunnett's multiple comparison tests are represented when relevant. Compared with baseline, *p < 0.05, †p < 0.001.
Discussion
2DTT was recently developed as an alternative technique to the tissue Doppler imaging (TDI) derived strain method, which was previously introduced as a method to quantify myocardial function [3,6,8,11,16,19,21]. 2DTT overcomes a number of problems encountered with TDI, including angle dependency, cardiac translation, noise interference, substantial intra-observer and inter-observer variability, and inability to measure strain in the azimuth or perpendicular planes [2,3,7,8,10,11,14,16,17,21]. In addition, 2DTT allows simultaneous assessment of global and regional myocardial movements, as well as quantitative evaluation of ventricular torsion and dyssynchrony [8,11,14,16,17,20,21]. The strain parameters derived from 2DTT have been validated in dogs, and shown to be well correlated with TDI derived strain, sonomicrometry, MRI, and measurement of the maximum rate of pressure rise during LV contraction (peak LV dP/dt) obtained from the pressure-volume loop [1,8,9,27]. However, most studies of 2DTT in veterinary medicine have been limited to clinically normal dogs, and there have not been many reports of strain analysis on cardiac disorders. Therefore, the present study was conducted as a pre-clinical evaluation to test the applicability of 2DTT on cardiac disorders. Specifically, experimentally induced canine myocardial dysfunction models were used to assess the ability of 2DTT to evaluate LV myocardial function in association with sustained high electrical pacing by analyzing; (1) global myocardial function, (2) regional myocardial function, and (3) the degree of dyssynchrony.
Human and animal studies have established that RV apical pacing results in dilated, congestive cardiomyopathy characterized by LV systolic and diastolic dysfunction and LV dyssynchrony [2,22,24,25,28-31]. The degree of myocardial dysfunction is dependent on the time and the rate of pacing [22,31]. In the present study, a three-week protocol with apacing rate of 250 bpm was chosen to ensure adequate LV structural changes and dysfunction during the three week period that could be detected by echocardiography.
Sustained high electrical pacing resulted in a successful tachycardia induced myocardial dysfunction model, with LV dilation and thinning of the myocardium. Systolic dysfunction, indicated by the reduction of FS, was observed immediately after the onset of pacing. Diastolic dysfunction, which was observed after the onset of systolic dysfunction, was characterized by reduction of A wave velocity and deceleration time, which was consistent with impaired compliance. These changes were also accompanied by reduced cardiac output, as indicated by the reduced blood pressure.
Pacing caused significant reduction of both global radial and circumferential strains. Radial strain indicates transmural dysfunction, whereas circumferential strains suggest subendocardial and subepicardial dysfunction [14]. Additionally, according to Wang et al. [26], systolic heart failure is characterized by the reduction of longitudinal, radial, and circumferential strains, whereas diastolic heart failure is characterized by the reduction of longitudinal and radial strains with preserved circumferential strains. In the present study, the significant myocardial changes observed in both radial and circumferential directions were most likely the result of both systolic and diastolic dysfunction, and indicative of transmural, subendocardial, and subepicardial dysfunction. Conventionally, FS has been used to evaluate the global function of the LV [5,13,23]. However, it may not reflect the true global function since it is only measured at the anteroseptal and posterior segments, and it only assesses radial deformation [3,18,20,23]. Conversely, global radial and circumferential strains can be assessed simultaneously. These parameters are the averages of measurements taken at multiple myocardial segments; therefore, they provide a better representation of the global myocardial function [3,14,17]. For example, dogs with uneven myocardial movements are sometimes encountered in clinical settings, such as when a dog has sustained myocardial movement only at the IVS, resulting in the values of FS remaining adequate. In such cases, 2DTT may be better suited for evaluation of LV myocardial function. However, further investigations using clinical cases are required to explore this possibility.
The results of regional strain parameters have shown pacing to have a detrimental effect on the regional myocardium in both the radial and circumferential directions. Interestingly, the six myocardial segments were not affected to the same degree, and the segments closest to the lead appeared to maintain function in both directions. Percent wall thickening is the difference in wall thickness at diastole and systole, a parameter similar to radial strain [28]. This parameter allows quantitative analysis of the regional myocardial movements at the IVS and LVFW, and can be used to evaluate the regional contractility of the myocardium [28]. In this study, consistent results of maintained myocardial movements at the IVS and reduced movements at the LVFW were observed in both % wall thickening and radial strains, confirming the results of the regional strain analysis. Wilson et al. [28] also looked at the changes in wall thickening in canine tachycardia induced myocardial dysfunction models and found impaired wall thickening at the segments closest to the pacing lead, which is contrary to the present finding. The results of this study do not allow elucidation of the mechanism underlying the maintenance of myocardial movement of the segments closest to the pacemaker lead. Regional strain analysis is an advantage of 2DTT because it provides an additional assessment of the myocardial function, which cannot be evaluated using conventional echocardiography alone.
The use of 2DTT in the field of human medicine is widely increasing as a method for assessment of cardiac resynchronization therapy and evaluation of ventricular dyssynchrony caused by permanent pacemaker devices [15,19,24,25,30]. A number of human studies have demonstrated an association between increased dyssynchrony and decreased LV function [12,15,25,30]. In the present study, LV dyssynchrony was measured in terms of STI, which is the difference in timing of peak strain from the earliest to the latest segments. Significant differences were observed in the radial direction, whereas no significant differences were observed in the circumferential direction. Similar results have been observed in humans, where a greater degree of myocardial deformation was observed in the radial direction [12,30]. These findings suggest that dyssynchrony is easier to detect in the radial direction. Additionally, the earliest and latest segments differed in each dog in the present study, indicating that the timing of the peak strain for each segment is not related to the degree of the strain, and that there was great individual variation. Overall, this study demonstrated the ability of the 2DTT to detect and measure dyssynchrony in canine myocardial dysfunction models. The ability to measure dyssynchrony would aid in the evaluation and monitoring of myocardial disorders.
There are several limitations to this study. Specifically, there was a small number of animals involved in the study. In addition, the high pacing rate employed may have been a limitation. Past studies of 2DTT have shown its ability for use in regional analysis, and strains are thought to be a more sensitive parameter of LV function that allow earlier detection of the myocardial dysfunction [23]. However, due to such a high pacing rate causing acute and severe myocardial changes, FS and 2DTT parameters both demonstrated immediate changes from the first week of pacing. 2DTT also has its own technical limitations. Specifically, the accuracy of the strain values depends on the quality of the image and the frame rates [14]. In addition, the inadequate small search area of the tracking points may cause the speckles to move in and out of the search area, decreasing the reliability and the ability to track these speckles. Therefore, in some studies, there have been reports of an inability to measure 2DTT parameters in as many as 5% of the myocardial segments [4].
In conclusion, this study has shown the ability of 2DTT to measure radial and circumferential strain parameters from the right parasternal short axis view, and to evaluate changes in global and regional myocardial movement and the degree of dyssynchrony in dogs with sustained high electrical pacing. The additional assessments of the regional myocardial function and the degree of dyssynchrony are great advantages of 2DTT, which facilitates our understanding of myocardial function.
References
- 1.Amundsen BH, Helle-Valle T, Edvardsen T, Torp H, Crosby J, Lyseggen E, Stoylen A, Ihlen H, Lima JA, Smiseth OA, Slordahl SA. Noninvasive myocardial strain measurement by speckle tracking echocardiography: validation against sonomicrometry and tagged magnetic resonance imaging. J Am Coll Cardiol. 2006;47:789–793. doi: 10.1016/j.jacc.2005.10.040. [DOI] [PubMed] [Google Scholar]
- 2.Arita T, Sorescu GP, Schuler BT, Schmarkey LS, Merlino JD, Vinten-Johansen J, Leon AR, Martin RP, Sorescu D. Speckle-tracking strain echocardiography for detecting cardiac dyssynchrony in a canine model of dyssynchrony and heart failure. Am J Physiol Heart Circ Physiol. 2007;293:H735–H742. doi: 10.1152/ajpheart.00168.2007. [DOI] [PubMed] [Google Scholar]
- 3.Artis NJ, Oxborough DL, Williams G, Pepper CB, Tan LB. Two-dimensional strain imaging: a new echocardiographic advance with research and clinical applications. Int J Cardiol. 2008;123:240–248. doi: 10.1016/j.ijcard.2007.02.046. [DOI] [PubMed] [Google Scholar]
- 4.Becker M, Lenzen A, Ocklenburg C, Stempel K, Kühl H, Neizel M, Katoh M, Kramann R, Wildberger J, Kelm M, Hoffmann R. Myocardial deformation imaging based on ultrasonic pixel tracking to identify reversible myocardial dysfunction. J Am Coll Cardiol. 2008;51:1473–1481. doi: 10.1016/j.jacc.2007.10.066. [DOI] [PubMed] [Google Scholar]
- 5.Boon JA. Veterinary Echocardiography. 2nd ed. Chichester: John Wiley & Sons; 2011. pp. 101–112. [Google Scholar]
- 6.Chetboul V. Advanced techniques in echocardiography in small animals. Vet Clin North Am Small Anim Pract. 2010;40:529–543. doi: 10.1016/j.cvsm.2010.03.007. [DOI] [PubMed] [Google Scholar]
- 7.Chetboul V, Sampedrano CC, Gouni V, Nicolle AP, Pouchelon JL, Tissier R. Ultrasonographic assessment of regional radial and longitudinal systolic function in healthy awake dogs. J Vet Intern Med. 2006;20:885–893. doi: 10.1892/0891-6640(2006)20[885:uaorra]2.0.co;2. [DOI] [PubMed] [Google Scholar]
- 8.Chetboul V, Serres F, Gouni V, Tissier R, Pouchelon JL. Radial strain and strain rate by two-dimensional speckle tracking echocardiography and the tissue velocity based technique in the dog. J Vet Cardiol. 2007;9:69–81. doi: 10.1016/j.jvc.2006.11.002. [DOI] [PubMed] [Google Scholar]
- 9.Culwell NM, Bonagura JD, Schober KE. Comparison of echocardiographic indices of myocardial strain with invasive measurements of left ventricular systolic function in anesthetized healthy dogs. Am J Vet Res. 2011;72:650–660. doi: 10.2460/ajvr.72.5.650. [DOI] [PubMed] [Google Scholar]
- 10.Dandel M, Hetzer R. Echocardiographic strain and strain rate imaging--clinical applications. Int J Cardiol. 2009;132:11–24. doi: 10.1016/j.ijcard.2008.06.091. [DOI] [PubMed] [Google Scholar]
- 11.Edvardsen T, Helle-Valle T, Smiseth OA. Systolic dysfunction in heart failure with normal ejection fraction: speckle-tracking echocardiography. Prog Cardiovasc Dis. 2006;49:207–214. doi: 10.1016/j.pcad.2006.08.008. [DOI] [PubMed] [Google Scholar]
- 12.Friedberg MK, Slorach C. Relation between left ventricular regional radial function and radial wall motion abnormalities using two-dimensional speckle tracking in children with idiopathic dilated cardiomyopathy. Am J Cardiol. 2008;102:335–339. doi: 10.1016/j.amjcard.2008.03.064. [DOI] [PubMed] [Google Scholar]
- 13.Fuentes VL. Echocardiography and Doppler ultrasound. In: Tilley L, Smith F, Oyama M, Sleeper M, editors. Manual of Canine and Feline Cardiology. 4th ed. Missouri: Saunders; 2008. pp. 78–98. [Google Scholar]
- 14.Geyer H, Caracciolo G, Abe H, Wilansky S, Carerj S, Gentile F, Nesser HJ, Khandheria B, Narula J, Sengupta PP. Assessment of myocardial mechanics using speckle tracking echocardiography: fundamentals and clinical applications. J Am Soc Echocardiogr. 2010;23:351–369. doi: 10.1016/j.echo.2010.02.015. [DOI] [PubMed] [Google Scholar]
- 15.Labombarda F, Blanc J, Pellissier A, Stos B, Gaillard C, Bajolle F, Maltret A, Sidi D, Bonnet D, Boudjemline Y. Health-e-Child project: mechanical dyssynchrony in children with dilated cardiomyopathy. J Am Soc Echocardiogr. 2009;22:1289–1295. doi: 10.1016/j.echo.2009.07.026. [DOI] [PubMed] [Google Scholar]
- 16.Lindqvist P, Borgström E, Gustafsson U, Mörner S, Henein MY. Asynchronous normal regional left ventricular function assessed by speckle tracking echocardiography: appearances can be deceptive. Int J Cardiol. 2009;134:195–200. doi: 10.1016/j.ijcard.2008.01.045. [DOI] [PubMed] [Google Scholar]
- 17.Mondillo S, Galderisi M, Mele D, Cameli M, Lomoriello VS, Zacà V, Ballo P, D’Andrea A, Muraru D, Losi M, Agricola E, D'Errico A, Buralli S, Sciomer S, Nistri S, Badano L. Speckle-tracking echocardiography: a new technique for assessing myocardial function. J Ultrasound Med. 2011;30:71–83. doi: 10.7863/jum.2011.30.1.71. [DOI] [PubMed] [Google Scholar]
- 18.Nesbitt GC, Mankad S, Oh JK. Strain imaging in echocardiography: methods and clinical applications. Int J Cardiovasc Imaging. 2009;25(Suppl 1):9–22. doi: 10.1007/s10554-008-9414-1. [DOI] [PubMed] [Google Scholar]
- 19.Nesser HJ, Winter S. Speckle tracking in the evaluation of left ventricular dyssynchrony. Echocardiography. 2009;26:324–336. doi: 10.1111/j.1540-8175.2008.00866.x. [DOI] [PubMed] [Google Scholar]
- 20.Perk G, Tunick PA, Kronzon I. Non-Doppler two-dimensional strain imaging by echocardiography - from technical considerations to clinical applications. J Am Soc Echocardiogr. 2007;20:234–243. doi: 10.1016/j.echo.2006.08.023. [DOI] [PubMed] [Google Scholar]
- 21.Schwarzwald CC, Schober KE, Berli ASJ, Bonagura JD. Left ventricular radial and circumferential wall motion analysis in horses using strain, strain rate, and displacement by 2D speckle tracking. J Vet Intern Med. 2009;23:890–900. doi: 10.1111/j.1939-1676.2009.0321.x. [DOI] [PubMed] [Google Scholar]
- 22.Shinbane JS, Wood MA, Jensen DN, Ellenbogen KA, Fitzpatrick AP, Scheinman MM. Tachycardia-induced cardiomyopathy: a review of animal models and clinical studies. J Am Coll Cardiol. 1997;29:709–715. doi: 10.1016/s0735-1097(96)00592-x. [DOI] [PubMed] [Google Scholar]
- 23.Takano H, Fujii Y, Ishikawa R, Aoki T, Wakao Y. Comparison of left ventricular contraction profiles among small, medium, and large dogs by use of two-dimensional speckle-tracking echocardiography. Am J Vet Res. 2010;71:421–427. doi: 10.2460/ajvr.71.4.421. [DOI] [PubMed] [Google Scholar]
- 24.Tomaske M, Breithardt OA, Balmer C, Bauersfeld U. Successful cardiac resynchronization with single-site left ventricular pacing in children. Int J Cardiol. 2009;136:136–143. doi: 10.1016/j.ijcard.2008.04.048. [DOI] [PubMed] [Google Scholar]
- 25.Tops LF, Suffoletto MS, Bleeker GB, Boersma E, van der Wall EE, Gorcsan J, 3rd, Schalij MJ, Bax JJ. Speckle-tracking radial strain reveals left ventricular dyssynchrony in patients with permanent right ventricular pacing. J Am Coll Cardiol. 2007;50:1180–1188. doi: 10.1016/j.jacc.2007.06.011. [DOI] [PubMed] [Google Scholar]
- 26.Wang J, Khoury DS, Yue Y, Torre-Amione G, Nagueh SF. Preserved left ventricular twist and circumferential deformation, but depressed longitudinal and radial deformation in patients with diastolic heart failure. Eur Heart J. 2008;29:1283–1289. doi: 10.1093/eurheartj/ehn141. [DOI] [PubMed] [Google Scholar]
- 27.Wess G, Keller LJM, Klausnitzer M, Killich M, Hartmann K. Comparison of longitudinal myocardial tissue velocity, strain, and strain rate measured by two-dimensional speckle tracking and by color tissue Doppler imaging in healthy dogs. J Vet Cardiol. 2011;13:31–43. doi: 10.1016/j.jvc.2010.08.001. [DOI] [PubMed] [Google Scholar]
- 28.Wilson JR, Douglas P, Hickey WF, Lanoce V, Ferraro N, Muhammad A, Reichek N. Experimental congestive heart failure produced by rapid ventricular pacing in the dog: cardiac effects. Circulation. 1987;75:857–867. doi: 10.1161/01.cir.75.4.857. [DOI] [PubMed] [Google Scholar]
- 29.Wu W, Wang H, Tang Y, Yuan W, Wang H, Jiang Y. Application of quantitative tissue velocity imaging to evaluate left ventricular early diastolic dysfunction in dogs with heart failure due to rapid ventricular pacing. J Am Soc Echocardiogr. 2008;21:1269–1276. doi: 10.1016/j.echo.2008.07.004. [DOI] [PubMed] [Google Scholar]
- 30.Yoshikawa H, Suzuki M, Tezuka N, Otsuka T, Sugi K. Differences in left ventricular dyssynchrony between high septal pacing and apical pacing in patients with normal left ventricular systolic function. J Cardiol. 2010;56:44–50. doi: 10.1016/j.jjcc.2010.02.002. [DOI] [PubMed] [Google Scholar]
- 31.Zupan I, Rakovec P, Budihna N, Brecelj A, Koželj M. Tachycardia induced cardiomyopathy in dogs; relation between chronic supraventricular and chronic ventricular tachycardia. Int J Cardiol. 1996;56:75–81. doi: 10.1016/0167-5273(96)02728-3. [DOI] [PubMed] [Google Scholar]