

Sir,
We read with interest a report by Glenn et al.,[1] in which the authors assessed platelet function by platelet function analyzer (PFA) and standard thromboelastography (TEG) in a patient requiring epidural catheter removal as the patient had received an oral dose of clopidogrel and aspirin 72 hours earlier. As the results of both the tests were normal, removal of epidural catheter was allowed and authors concluded that ‘PFA and TEG offer potentially reliable guidance for epidural catheter removal in patient who had received double antiplatelet therapy’ (last paragraph pg 101).
However, we have some reservations if such conclusions can be drawn from their findings as antiplatelet response of aspirin and clopidogrel varies widely from one individual to another; with some having no response while some having bleeding.[2] Moreover, although PFA is a good screening tool for assessing platelet function, it is not recommended for monitoring of clopidogrel efficacy.[3] Also the ‘standard TEG’ used in the study is not sensitive to aspirin and clopidogrel drugs[4] and thus it can remain normal despite adequate platelet inhibition by aspirin and clopidogrel. While the modification of TEG, i.e., TEG-based platelet mapping (TEG®-PlateletMapping™; Haemoscope, Niles, IL, USA) can quantify the contribution of fibrin, adenosine diphosphate (ADP) receptor and thromboxane A2 (TxA2) receptor in clot strength.[5] Hence it can assess the effect of individual antiplatelet agents namely, aspirin and clopidogrel, via inhibition of TxA2 and ADP receptors, respectively. At our center we are using TEG-platelet mapping to quantify the effect of antiplatelet drugs in patients including those undergoing percutaneous cardiac intervention [Figure 1]. As illustrated in Figure 1 apart from MA-thrombin (maximum possible clot strength), it also measures MA-fibrin (clot strength by fibrin alone), MA-ADP (clot strength under ADP receptor inhibition by clopidogrel), MA-AA (clot strength under TxA2 receptor inhibition by aspirin) and thereafter the percentage (%) platelet inhibition is calculated. Thus platelet mapping measures platelet inhibition along with total platelet function as a reference point thereby assessing effect of antiplatelet agents more objectively.
Figure 1.
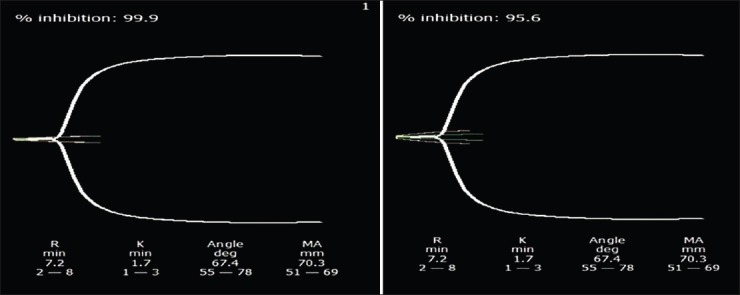
TEG-platelet mapping tracings in a patient posted for angioplasty who has received loading doses of aspirin and clopidogrel. Panel 1 shows % TxA2 receptor inhibition by aspirin. Panel 2 shows % ADP receptor inhibition by clopidogrel
Hence, use of TEG-platelet mapping would have been more appropriate to quantify the platelet inhibition by antiplatelet drugs more objectively and would have helped authors in taking evidence based decision to discontinue or continue antiplatelet therapy both before surgery and also postoperatively to ascertain the optimum timing for catheter removal. Also decision to stop antiplatelet agents in a case with recent stenting before surgery should be based on a quantitative assessment of platelet function by a method which can assess platelet inhibition with combined drug therapy. Though, authors used two different point of care tests namely, TEG and PFA to ascertain hemostatic function in their patient however, both of these tests have their own limitations[3,5] and TEG-platelet mapping alone would have been more appropriate in this setting. This is more so because TEG-platelet mapping assay could have been performed on the TEG analyzer using platelet-mapping kits.
References
- 1.Glenn E, Mehl J, Rosinia FA, Liu H. Safe removal of an epidural catheter 72 hours after clopidogrel and aspirin administrations guided by platelet function analysis and thromboelastography. J Anaesthesiol Clin Pharmacol. 2013;29:99–101. doi: 10.4103/0970-9185.105813. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Serebruany VL, Steinhubl SR, Berger PB, Malinin AI, Bhatt DL, Topol EJ. Variability in platelet responsiveness to clopidogrel among 544 individuals. J Am Coll Cardiol. 2005;45:246–51. doi: 10.1016/j.jacc.2004.09.067. [DOI] [PubMed] [Google Scholar]
- 3.Michelson AD, Frelinger AL, 3rd, Furman MI. Current options in platelet function testing. Am J Cardiol. 2006;98(10A):4–10N. doi: 10.1016/j.amjcard.2006.09.008. [DOI] [PubMed] [Google Scholar]
- 4.Hobson AR, Agarwala RA, Swallow RA, Dawkins KD, Curzen NP. Thrombelastography: Current clinical applications and its potential role in interventional cardiology. Platelets. 2006;17:509–18. doi: 10.1080/09537100600935259. [DOI] [PubMed] [Google Scholar]
- 5.Agarwal S, Coakley M, Reddy K, Riddell A, Mallett S. Quantifying the effect of antiplatelet therapy: A comparison of the platelet function analyzer (PFA-100) and modified thromboelastography (mTEG) with light transmission platelet aggregometry. Anesthesiology. 2006;105:676–83. doi: 10.1097/00000542-200610000-00011. [DOI] [PubMed] [Google Scholar]