

Abstract
Aim:
Oral motor dysfunction is a common issue in children with cerebral palsy (CP). Drooling, difficulties with sucking, swallowing, and chewing are some of the problems often seen. In this study, we aimed to research the effect of oral motor therapy on pediatric CP patients with feeding problems.
Materials and Methods:
Included in this single centered, randomized, prospective study were 81 children aged 12-42 months who had been diagnosed with CP, had oral motor dysfunction and were observed at the Pediatric Neurology outpatient clinic of the Children's Health and Diseases Department, Istanbul Medical Faculty, Istanbul University. Patients were randomized into two groups: The training group and the control group. One patient from the training group dropped out of the study because of not participating regularly. Following initial evaluation of all patients by a blinded physiotherapist and pedagogue, patients in the training group participated in 1 h oral motor training sessions with a different physiotherapist once a week for 6 months. All patients kept on routine physiotherapy by their own physiotherapists. Oral motor assessment form, functional feeding assessment (FFA) subscale of the multidisciplinary feeding profile (MFP) and the Bayley scales of infant development (BSID-II) were used to evaluate oral motor function, swallowing, chewing, the gag reflex, the asymmetrical tonic neck reflex, tongue, jaw, and mouth function, severity of drooling, aspiration, choking, independent feeding and tolerated food texture during the initial examination and 6 months later.
Results:
When the initial and post-therapy FFA and BSID-II scores received by patients in the training and the study group were compared, the training group showed a statistically significant improvement (P < 0.05).
Conclusion:
Oral motor therapy has a beneficial effect on feeding problems in children with CP.
Keywords: Cerebral palsy, feeding, oral motor function
Introduction
Cerebral palsy (CP) is a movement and posture disorder caused by non-progressive lesions in the developing brain. CP may affect oral motor skills, leading to speech delay, drooling and difficulties with sucking, swallowing, and chewing.[1,2] The feeding problems caused by oral motor dysfunction lead, in turn, to growth and development retardation,[3] while drooling leads to physical problems and has a major effect on social development.[4] It has been suggested that combining physiotherapy and rehabilitation with oral motor therapy may have a beneficial effect on functional independence levels.[5] The aim of this study was to assess the effect of oral motor therapy on oral functions and neuromotor development in children with CP.
Materials and Methods
Included in this single centered, randomized, prospective study were consecutively chosen 81 patients aged 12-42 months that were diagnosed with CP, who answered positively to having at least one or more problems of oral motor functions such as sucking, chewing, swallowing, drooling and independent feeding during routine follow-up to the same pediatric neurologist at the Pediatric, Neurology out-patient clinic of the Children's Health and Diseases Department, Istanbul Medical Faculty, Istanbul University. Patients who had seizures frequent enough to prevent daily activity and physiotherapy and who were receiving drug treatment for drooling were not included in the study.
Patients were randomized by the sequence in which they enter the study. Forty one patients made up the training group, while the other 40 served as the control group. All patients continued to receive routine physiotherapy guided by Istanbul University Istanbul Medical Faculty Department of Physiotherapy and Rehabilitation. Exclusion criterias to the training group was non-participation for more than three sessions and one patient was excluded from the study. The patients’ families were informed, that our aim was to provide oral motor therapy in order to strengthen oral motor functions, reduce drooling and feeding problems, and increase daily life activities of the patient. During the first meeting prior to the start of training, informed written consent was obtained from a legal guardian by our research nurse. This study was approved by the Ethics Committee of the Istanbul Medical Faculty and was carried out in accordance with the Declaration of Helsinki.
Oral motor therapy
Training group
Patients participated in 1 h oral motor therapy sessions with a physiotherapist once in a week for 6 months (12 sessions in total).
To improve swallowing and chewing, the tactile and proprioceptive aspect of eating was intended to be increased. To improve mouth function and mouth control, the texture of food was gradually thickened, and families were taught proper positioning.
When mouth muscle control was insufficient, mouth control was performed to enable feeding. Methods of spoon feeding were shown to the families. Oral stimulation was performed manually.
For drinking training, moderately dense liquids were used and correct glass use technique was taught. Children were taught correct midline hand use to facilitate independent feeding.
Mouth control, positioning and posture control were taught in order to reduce drooling.
Control group
Forty children diagnosed with CP and oral motor dysfunction was randomized to make up the control group. After the first evaluation, patients were called in for an evaluation 6 months later. During this time routine physiotherapy went on as planned when the patients started follow-up for the first time from our out-patient clinic. For the control group not participating regularly to routine physiotherapy was defined as exclusion criteria. All patients attended routine physiotherapy according to the established program during these 6 months.
Evaluation
Prior to and after the training, all patients were evaluated by a blinded physiotherapist different from the training physiotherapist using a patient evaluation form which includes name, gender, date of birth, diagnosis, status of swallowing, gag and asymmetric tonic neck (ASTN) reflexes, an oral motor assessment form and the Functional Feeding Assessment (FFA) subscale of the Multidisciplinary Feeding Profile (MFP). A blinded pedagogue who was not involved in the training sessions performed the Bayley scales of infant development (BSID-II) before and after the training. In the first evaluation, the number of cases with a particular oralmotor dysfunction was specified according to the patient's evaluation and oral motor assessment forms and control and training groups were compared according to their baseline values. Six months later in the second evaluation, again number of cases with the specific disorder assessed according to the patient evaluation and oral motor assessment forms. Change in the number of cases was analyzed. FFA and BSID-II were analyzed and compared between groups using their own scoring systems. The physiotherapist who performed the trainings did not intervene in data input or analyses. Those involved in data analyses were blinded during the study and data analyses via de-identified data.
Oral motor assessment form
The patients’ oral motor function was evaluated using the oral motor assessment form. Difficulties with sucking, swallowing, chewing, drooling, independent feeding, and feeding problems were graded as “present” or “absent”. Food texture, tongue, jaw and mouth function, swallowing function,[3] swallowing assessment[6] and severity of drooling,[7] aspiration and choking were evaluated.
FFA subscale of the MFP
All patients were observed during feeding. The FFA subscale of the MFP was used to assess spoon feeding, biting, chewing, drinking and swallowing. Behaviors in each area were categorized as normal and abnormal. Normal behaviors were marked as “adequate”, “poor”, “absent” or “not found”. Abnormal behaviors were marked as “absent”, “undecided”, “present” or “not found”. Performance in each area was rated in numbers as normal (90-100%), mildly impaired (70-89%), moderately impaired (50-69%) and severely impaired (<50%).[6]
Statistical analysis
Statistical analysis of data was performed using the SPSS for Windows 15.0 software. For two-tailed comparison of groups in terms of initial characteristics, pre-and post-therapy results and observed changes, a P < 0.05 was accepted as statistically significant. The Chi-square test or Fisher's exact test were used for comparison of categorical variables. The Mann-Whitney U and Student's t-test were used when dependent variables were not normally distributed.
Results
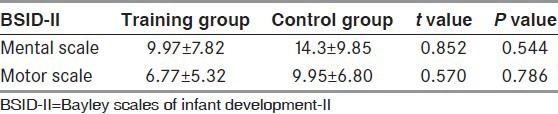
The average patient age was 24.32 months ± 10.86 months in the training group and 28.15 months ± 10.22 months in the control group. In the training group, 62.25% of patients were female (n = 25) and 37.5% were male (n = 15); in the control group, 50% were female (n = 20) and 50% were male (n = 20). There was no significant difference between groups in terms of sex, age, clinical types of CP [Table 1] and initial presence and types of oral motor difficulties (P > 0.05). Prior to therapy, no significant difference was found between groups in terms of tongue, jaw and mouth function, swallowing difficulties, severity of drooling, and tolerated food texture (P > 0.05). The average pre-therapy FFA [Table 2] and BSID-II scores [Table 3] did not vary significantly between groups (P > 0.05).
Table 1.
Clinical cerebral palsy types according to groups
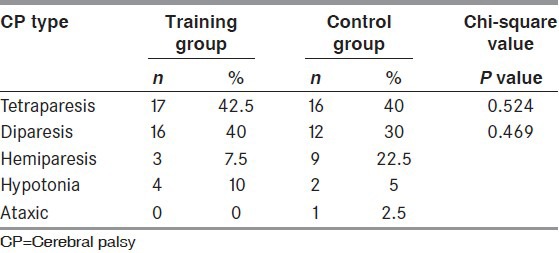
Table 2.
Baseline comparison between control and training group according to functional feeding assessment subscale of the multidisciplinary feeding profile
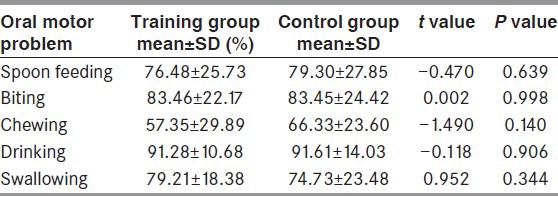
Table 3.
Baseline comparison of bayley scales of infant development-II scores between two group
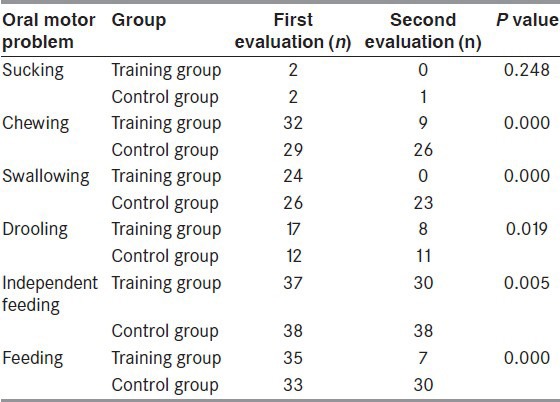
The pre- and post-therapy clinical features of patients in the two groups were compared. In terms of post-therapy changes in asymmetrical tonic neck reflex (ATNR) and swallowing reflex, no significant difference was seen between the two groups (P > 0.05). Regarding oral motor problems, there was no significant difference between groups in terms of sucking difficulty (P > 0.05). In terms of chewing, swallowing, drooling, independent feeding, and feeding problems, the changes in the training group were significantly more pronounced than in the control group (P < 0.05) [Table 4]. The training group also showed a marked improvement in swallow delay, aspiration, and choking as compared to the control group (P < 0.05), while no significant difference was seen between groups in coughing/suffocation improvement (P > 0.05).
Table 4.
The change in the oral motor problems of training and control groups 139
Changes in tongue extension, elevation and lateralization were significantly more prominent in the training group than in the control group (P < 0.05). Changes in jaw verticalization could not be evaluated due to the insufficient number of cases. There was no difference between groups in jaw lateralization improvement (P > 0.05), while the training group showed a significant improvement in jaw stabilization as compared to the control group (P < 0.05). Improvement in mouth functions like spoon feeding, lip wiping and holding the mouth/lips closed was significantly more pronounced in the training group as compared to the control group (P < 0.05), as was improvement in tolerated food texture (P < 0.05) and swallowing evaluation results (P < 0.05).
The training group showed a significant reduction in drooling as compared to the control group (P < 0.05).
In the training group, there was a significant improvement in average FFA scores as compared to the control group (P < 0.05) [Table 5]. The average BSID-II scores significantly improved in the training group as well (P < 0.05) [Table 6].
Table 5.
Comparison of the final functional feeding assessment scores of the groups
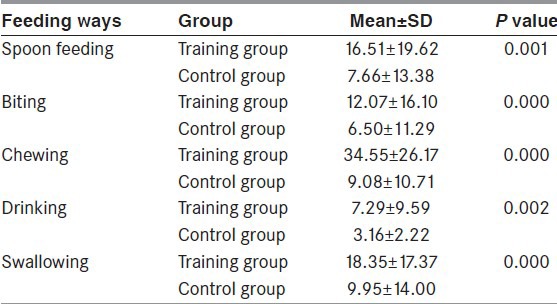
Table 6.
The change in the scores of bayley scales of infant development-II of training and control groups

Discussion
Voluntary oral movements play an important role in feeding development. Children with CP who have no gag reflex, a weak swallowing reflex and ATNR face serious feeding problems.[3,8]
In our study, no significant difference in ATNR or swallowing reflex improvement was seen between the therapy and the control group, which may be due to the limited number of cases with these problems. The lack of significant improvement in sucking difficulty may be explained by the fact that children under 1 year of age were not included in the study.
In a study of 28 tetraplegic CP patients aged 12-48 months, Borkowska reported that training had a significant effect on feeding, while correct positioning and feeding affected, in turn, the development of eye-hand coordination.[9] Similarly, the training group in our study showed a significant improvement in chewing, swallowing, drooling, independent feeding, and feeding problems.
A study of 27 children with CP by Gisel, evaluated the effect of 10-20 week oral sensorimotor training on aspiration frequency, feeding and growth. Oral motor training did not have a significant effect on feeding and growth but was found to reduce feeding problems caused by aspiration.[10] Using videofluoroscopy, Helfrich-Miller et al. diagnosed a delayed swallowing reflex and tongue dysfunction in 6 children with CP and severe mental retardation. Based on the pattern found in two patients who aspirated over 10% of every bite of food, they developed a program that included oral motor training, thermal stimulation, and changes in feeding routines. A marked improvement in swallowing function was seen after 4 months of therapy.[11] Similarly, the improvement in delayed swallowing, aspiration and choking seen in our training group points to the beneficial effect of oral motor training. It may not, however, have any effect on coughing/suffocation, as no improvement in this area was seen in either group.
Changes in jaw verticalization could not be evaluated due to the low number of cases, which may also be the reason why no difference was seen between groups in terms of jaw lateralization improvement. In a study of 12 children with CP aged 15-39 months, Reilly and Skuse observed their patients for 1 year without providing any training. The results of feeding evaluation showed that none of the children had mastered oral functions that involved tongue lateralization and jaw movement.[3] The improvement in jaw stabilization seen in our training group indicates the beneficial effect of mouth control training.
A study of 35 children with CP by Gisel, evaluated the effect of oral sensorimotor treatment on feeding. Eleven patients in the study group received treatment for 10 weeks, while the control group was only assigned chewing exercises. At the end of treatment, both groups showed a shorter duration of eating, but there was no significant change in food texture (solid, semi-solid, puree).[12] We saw an improvement in tolerated food texture in our training group, which we attribute to the 6 months of regular weekly therapy and family cooperation.
Domaracki and Sisson researched the effect of oral motor stimulation on drooling, which affects social life and health in children. Two patients received oral motor training for 1 h on school days, but no reduction in drooling was observed.[13] In a different study of eight CP patients six of whom had moderate-to-severe mental retardation, oral motor training helped reduce drooling.[14] These contradictory findings may be the result of small patient populations, lack of control groups and differences in training programs and their duration. In our study, a significant reduction in drooling was seen in the training group. We consider this progress to be the result of training that did not only focus on drooling but aimed to improve all oral motor functions.
At the end of therapy, changes in average FFA scores were compared between groups. In the training group, improvement in areas such as spoon feeding, biting, chewing, drinking and swallowing was significantly more pronounced than in the control group. We attribute this to the positive effect of feeding and oral motor training.
When the changes in average BSID-II scores were compared between groups, the therapy group showed a significant improvement in mental and motor scale scores. This can be attributed to the educational information on mental and motor development that was provided to the families in the training group during the 6 months of therapy.
Considering the fact that mothers can spend up long hours daily on feeding a child with CP, facilitating this process by improving oral motor functions can significantly reduce feeding times and stress levels for both the mother and the child, leaving time for other activities like physiotherapy and improving the family's quality of life.
To summarize, oral motor therapy involves the patient's family and a physiotherapist (9) has a beneficial effect on oral motor functions in children with CP.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.Reilly SM, Skuse DH, Wolke D, Stevenson J. Oral-motor dysfunction in children who fail to thrive: Organic or non-organic? Dev Med Child Neurol. 1999;41:115–22. doi: 10.1017/s0012162299000225. [DOI] [PubMed] [Google Scholar]
- 2.Senner JE, Logemann J, Zecker S, Gaebler-Spira D. Drooling, saliva production, and swallowing in cerebral palsy. Dev Med Child Neurol. 2004;46:801–6. doi: 10.1017/s0012162204001409. [DOI] [PubMed] [Google Scholar]
- 3.Reilly S, Skuse D. Characteristics and management of feeding problems of young children with cerebral palsy. Dev Med Child Neurol. 1992;34:379–88. doi: 10.1111/j.1469-8749.1992.tb11449.x. [DOI] [PubMed] [Google Scholar]
- 4.Blasco PA. Management of drooling: 10 years after the Consortium on Drooling, 1990. Dev Med Child Neurol. 2002;44:778–81. doi: 10.1017/s0012162201002924. [DOI] [PubMed] [Google Scholar]
- 5.Gisel EG. Oral-motor skills following sensorimotor intervention in the moderately eating-impaired child with cerebral palsy. Dysphagia. 1994;9:180–92. doi: 10.1007/BF00341263. [DOI] [PubMed] [Google Scholar]
- 6.Yilmaz S, Basar P, Gisel EG. Assessment of feeding performance in patients with cerebral palsy. Int J Rehabil Res. 2004;27:325–9. doi: 10.1097/00004356-200412000-00013. [DOI] [PubMed] [Google Scholar]
- 7.O’Dwyer TP, Conlon BJ. The surgical management of drooling: A 15 year follow-up. Clin Otolaryngol Allied Sci. 1997;22:284–7. doi: 10.1046/j.1365-2273.1997.00022.x. [DOI] [PubMed] [Google Scholar]
- 8.Engsberg JR, Olree KS, Ross SA, Park TS. Quantitative clinical measure of spasticity in children with cerebral palsy. Arch Phys Med Rehabil. 1996;77:594–9. doi: 10.1016/s0003-9993(96)90301-9. [DOI] [PubMed] [Google Scholar]
- 9.Borkowska M. Effect of rehabilitation of the feeding function on the development of visual-motor coordination and speech in children with infantile cerebral palsy. Probl Med Wieku Rozwoj. 1979;9:209–34. [PubMed] [Google Scholar]
- 10.Gisel EG, Applegate-Ferrante T, Benson JE, Bosma JF. Effect of oral sensorimotor treatment on measures of growth, eating efficiency and aspiration in the dysphagic child with cerebral palsy. Dev Med Child Neurol. 1995;37:528–43. doi: 10.1111/j.1469-8749.1995.tb12040.x. [DOI] [PubMed] [Google Scholar]
- 11.Helfrich-Miller KR, Rector KL, Straka JA. Dysphagia: Its treatment in the profoundly retarded patient with cerebral palsy. Arch Phys Med Rehabil. 1986;67:520–5. [PubMed] [Google Scholar]
- 12.Gisel EG. Effect of oral sensorimotor treatment on measures of growth and efficiency of eating in the moderately eating-impaired child with cerebral palsy. Dysphagia. 1996;11:48–58. doi: 10.1007/BF00385800. [DOI] [PubMed] [Google Scholar]
- 13.Domaracki LS, Sisson LA. Decreasing drooling with oral motor stimulation in children with multiple disabilities. Am J Occup Ther. 1990;44:680–4. doi: 10.5014/ajot.44.8.680. [DOI] [PubMed] [Google Scholar]
- 14.Yam WK, Yang HL, Abdullah V, Chan CY. Management of drooling for children with neurological problems in Hong Kong. Brain Dev. 2006;28:24–9. doi: 10.1016/j.braindev.2005.03.008. [DOI] [PubMed] [Google Scholar]