

Abstract
Objectives:
To study the prevalence of language delay and to examine its socio-economic correlates in children less than 3 years.
Materials and Methods:
Participants were 130 children (males = 56%) aged 12-35 months (mean age = 1.81 years, SD = 0.58), from an urban center in north India. The language quotient (LQ) of the child was measured by the Clinical Linguistic Auditory Milestone Scale (CLAMS). Children with an LQ score of less than 70 were considered language delayed.
Results:
Overall, 6.2% of the children were language delayed with a higher prevalence found for girls (7%) than for boys (5.5%), although the difference was not statistically significant. Several significant correlations between socio-economic and demographic variables and the LQ of the child were found. Stepwise multiple regression analysis revealed that 31.4% of the variance in the LQ scores of girls was accounted for by income (F = 23.80, P = 0.000) and 18.1% of the variance in the LQ scores of boys was accounted for by education of the mother and income (F = 15.67, P = 0.000).
Conclusions:
Developmental problems in early years are often precursors of problems in later life and early intervention can facilitate favorable outcomes among children with multiple risks. The high prevalence of language difficulties in young children underscores the need to target language delay in early years, to reduce the likelihood of adverse outcomes and thus optimize chances of improvement.
Keywords: Children, language delay, socio-economic correlates
Introduction
Speech and language development is one of the most useful pointers of a child's overall development and intellectual functioning.[1] Parents are most likely to raise speech and language delay concerns in their encounters with primary care clinicians.[2,3] Prevalence rates for language delay have been reported across wide age ranges and samples. For children aged less than 5 years, studies have reported prevalence rates ranging from 2.3% to 19%.[4,5,6] Evidence indicates that untreated speech and language delay in preschool children can persist in 40-60% of the children and these children are at a high risk for social, behavioral, emotional, and cognitive problems in their later years.[7] Early identification of children at risk for language and other developmental problems can lead to enrollment in intervention programs, which can ameliorate the impact of early risk considerably.[3,8] Several population-based studies have recommended that screening toddlers for language delays reduces the number of children who require special education, which leads to improved language performance.[4,6,9]
Most of the studies on language development have been conducted in the developed countries and only a handful of studies from India have examined the prevalence and correlates of language delay in young children. In a recently conducted study of neurologic associations and factors related to speech and language delay, Parakh et al.[10] examined the medical records of 670 patients, with a mean age of 6.1 years (SD = 4.72), attending the pediatric neurology clinic of a tertiary care hospital over a period of 1 year. Prevalence of speech and language delay was found to be 16.27% and the male to female ratio was 2.76:1. Language delay was found to be associated with medical disorders such as seizure disorder, ADHD, autism, neonatal resuscitation, and epileptiform EEG with or without clinical seizure activity. In another study, Malhi and Singhi[11] evaluated 79 parent–child dyads who were seeking well-child pediatric services in the outpatient department of a tertiary care teaching hospital. Children in the age range of 2-5 years with no history of motor or sensory impairment, chronic illness, or perinatal problems were recruited to study the relationship between parents’ concerns and the child's developmental status. Parental concerns were elicited using a standardized questionnaire, Parents Evaluation of Developmental Status.[12] Expressive language concerns were significantly more likely to be raised by parents of children with delayed development (23%) compared to parents of children with normal development (14%). The authors concluded that parents’ concerns about expressive and receptive language and gross and fine motor development were moderately sensitive predictors of developmental delay in children between 2 and 5 years.
However, the findings of studies based on clinic-based samples cannot shed light on the language development of children in the general population. In a community-level study, Sidhu et al.[13] assessed 123 pre-school children aged two and a half to five years for developmental status using the Battelle Developmental Inventory-II.[14] Twenty-one (17%) children showed delayed expressive language functioning, defined as standard scores one standard deviation below the mean. Children with delayed language showed significantly lower scores on tasks that tested attention, memory, reasoning, academics, perception, and concepts. The authors concluded that language impairment in young children is associated with a broad spectrum of developmental impairments and there is need for multi-disciplinary developmental surveillance.
Several risk factors such as poverty, male sex, family history of speech and language delay, perinatal risk factors, family discord, family size, social stress, maternal depression, and poor parental education have been found to be associated with greater risk for language delay in children.[15,16,17] For example, Sidhu et al.[17] examined the relationship between cumulative biological and environmental risk factors and the language development of children less than 3 years using the Clinical Linguistic Auditory Milestone Scale (CLAMS).[18] Twelve possible risk factors, 4 biological and 8 environmental, were studied including preterm birth, low birth weight, history of birth asphyxia, history of neonatal jaundice, low income, large family size, minimal father's and mother's education, disadvantaged caste, low level of occupation of head of the household, absence of father, and higher birth order. A significant general downward linear trend in the language quotient (LQ) was found as the number of risk factors increased. Each risk factor reduced the LQ of the children by 2.63 points. The authors argued that the adverse effects of early exposure to risk factors for children living in disadvantaged and impoverished homes render children less likely to succeed in school, compromises their academic achievement, and impacts their potential to succeed in adult life.
Given the significance of early language skills for cognitive development, schooling, and academic achievement of children, it is important to study both the prevalence of language delay and the socio-economic risk factors associated with it. Moreover, early screening and detection of children with language delays is important as it can identify children who require intensive stimulation services, which in turn leads to improved language performance. Prevalence of language delay and its correlates in the community is virtually unknown in India. Most of the studies have been conducted on clinical samples of children, and these cannot be used to shed light on the correlates of early language delay in young children. The present study was therefore designed to provide preliminary data on the prevalence of language delay in young children from the community and to study its socio-economic and demographic correlates.
Materials and Methods
Participants
A total of 130 children (males = 56.15%) aged 12-35 months (mean age = 1.81 years, SD = 0.58) attending government and private crèches and play schools and hospitals for routine well child visits were recruited from an urban center in north India. The mean age of the children was 16.89 months (SD = 3.01) in the age group of 12-23 months and 29.76 months (SD = 3.21) in the age group of 24-35 months.
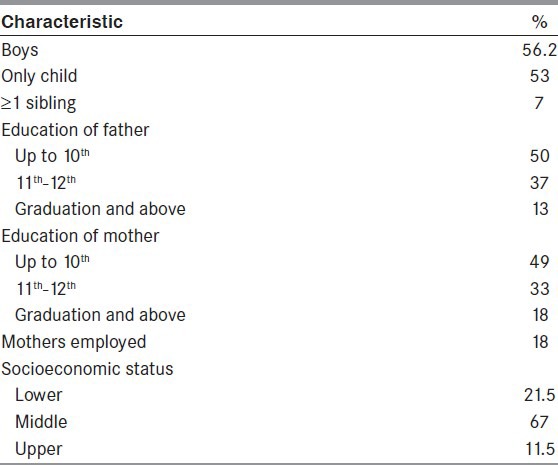
The data considered here are part of a larger study focusing on the assessment of children in multiple developmental domains. All children with a history of parent-reported sensory impairments or chronic illnesses were excluded from the study. A description of the sample is provided in Table 1.
Table 1.
Background characteristics of children and parents (N=130)
Measures
A semi-structured interview schedule was used to elicit information from the primary caretaker on the socio-economic, demographic, and birth-related variables of the child. The language development of the child was measured by the CLAMS.[18]
Clinical linguistic auditory milestone scale
The main outcome measure was the LQ of the child as measured by the CLAMS,[18] which is a 43-item language assessment instrument that assesses the receptive and expressive language development skills and milestones in children aged 1-36 months of age. For example, orients towards bell – upward directly (9 months); whether the child understands no (10 months); understand one step command with gesture (12 months); 3-word vocabulary (14 months); mature jargoning (18 months); 2-word phrases (21 months). The test uses standardized methods for obtaining information from parent report and from direct interaction between the examiner and the child. The CLAMS focuses on expressive and receptive language skills of children up to 3 years of age. The scale yields a language developmental age in months, which is then used to derive an LQ by dividing the language age by the chronological age and multiplying by 100. An LQ score less than 70 indicates a significant delay in language development. LQ scores between 70 and 90 indicate low average language developmental status, 91-110 represent average language skills, and LQ scores more than 111 depict above-average language development. The CLAMS has been used with Indian children and been found to be a useful test to measure language development.[3,17] The interview with the parent/caregiver and the language and developmental assessment of the child was conducted by a trained psychologist.
Socioeconomic status
The revised Kuppuswamy socio-economic status scale was used to assess the socio-economic status (SES) of the family.[19] The scale is based on 3 parameters: Education, occupation, and income of the family members. The scale assigns a score to each of these three categories, with higher scores indicating higher socio-economic status. The scale classifies the monthly income of the family into seven categories and assigns scores ranging from 1 to 12, with higher scores indicating higher income. Education is classified into 7 categories; the lowest score of 1 is assigned to a person who is illiterate and 7 to a professional degree holder. Occupation is also classified into 7 categories, with the lowest score of 1 being assigned to an unemployed person and the highest score of 10 being assigned to a person who is a professional. The scores on the 3 parameters are added to yield a total score that ranges from 3 to 29. Based on the total score of each family, 5 categories of socio-economic groups are identified: Upper (scores 25-29), Upper Middle (16-25), Lower Middle (11-15), Upper Lower (5-10), and Lower (<5). Higher scores indicate higher SES.
Results
Prevalence of language delay by age and sex
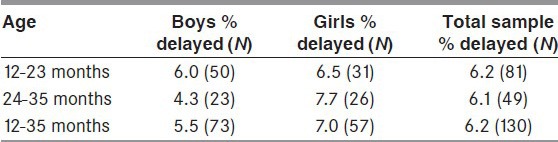
Table 2 presents the prevalence of language delay by age and sex. Overall 6.2% of the children had scores less than 70 on CLAMS and were language delayed. Although more girls (7%) compared to boys (5.5%) were language delayed, the difference was not statistically significant. There was no difference in the prevalence of language delay by age. Prevalence of language delay was found in 6.2% of the children less than 24 months of age and in 6.1% of children 24-35 months of age. The table also shows that the percentage of language delay tends to decline with age for boys and increase for girls, although no significant sex differences emerged in the prevalence of language delay at any age.
Table 2.
Prevalence of language delay by age and sex of child
Socio-economic and demographic correlates of language development in children
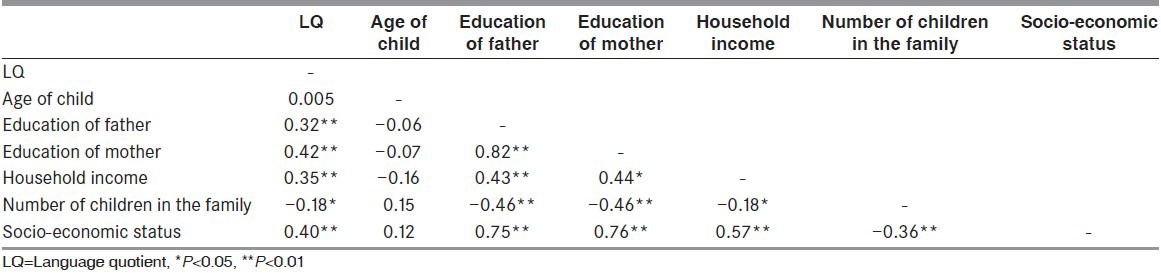
Table 3 presents the inter-correlations between the LQ on the CLAMS and the socio-economic and demographic variables. Several significant correlations between socio-economic, demographic variables, and LQ of the child were found. The LQ of the child was positively correlated with education of the mother (r = 0.42, P < 0.01), education of the father (r = 0.32, P < 0.01), SES index (r = 0.40, P < 0.01), and household income (r = 0.35, P < 0.01), and negatively correlated with number of children in the family (r = 0.18, P < 0.05). The results indicate that children from relatively poorer homes, with parents with low levels of education, and belonging to lower socio-economic status families with more children were more likely to have lower LQs.
Table 3.
Inter correlations of the socio-economic and demographic characteristics with language quotient
Stepwise multiple regression was performed to examine the crucial socio-economic and demographic predictors of the LQ of children. The analysis revealed that 31.4% of the variance in the LQ scores of girls was accounted for by income (F = 23.80, P = 0.000) and 18.1% of the variance in the LQ scores of boys was accounted for by education of the mother and income (F = 15.67, P = 0.000).
Discussion
This paper provides a rare examination of the prevalence of language delay in Indian children less than 3 years of age from the community setting and highlights that a sizeable minority have language delay. Language delay was found in 6.2% of the children less than 3 years of age. Our results are in line with results from studies conducted in the West, which also report prevalence rates for speech and language delay in the range of 2-8%.[4,20,21] There is considerable evidence to show that untreated speech language delay in young children is associated with diminished reading skills, behavioral problems, social skills deficits, and psychosocial adjustment problems. In turn, these difficulties may lead to overall poor academic achievement and lower IQs.[22,23] Furthermore, longitudinal data on early language delay suggests that these children continue to show poor academic skills even as adolescents.[24] Since language delay has long-term cognitive and behavioral sequelae, the high prevalence of language difficulties in young children found in the present community sample underscores the need to target language delay in early years, to reduce the likelihood of adverse outcomes and optimize chances of improvement. Most language problems in children can be identified at an early stage in the preschool period when interventions are most effective.[25,26]
No sex differences in language delay at any age were found and the female advantage in language development observed in the developed countries[27,28] was not replicated in the present study. Interestingly, more boys than girls were language delayed at less than 24 months of age, and more girls were delayed after the age of 24 months, although these sex differences were not statistically significant. Perhaps the strong son preference along with a general neglect of the girl child prevalent in the north Indian states negates the language advantage accruing to girls all over the world.[29,30] It is noteworthy that the percentage of girls with delayed language increases with age wherein for boys it decreases with age.
Income and maternal education emerged as significant contributing factors to the LQ of the child. Evidence indicates that socio-economic disadvantage is associated with inadequate food, poor nutrition and hygiene, poor maternal education, inadequate stimulation at home, inadequate schooling, and suboptimal physical environment at home.[31,32,33,34,35,36,37] Children from socio-economically disadvantaged families begin their lives with a poorer platform of health and a reduced capacity to benefit from the economic and social advances experienced by the rest of the society. Better educated mothers not only talk more to their children but also use more complex words and hence provide a cognitively enriched environment, which in turn enhances the child's language skills.[38,39,40,41,42] Maternal education is therefore a proxy measure of the quality of home environment that parents provide to their developing children.
There are some limitations of the study that should be taken into account while generalizing the results of the study. First, the small sample size does not represent the population and more controlled studies are required to elaborate and confirm the findings. However, the study provides preliminary data and this can be used to generate hypotheses for future investigations. Secondly, cross-sectional data are used to study the prevalence of language delay in the various ages; longitudinal data would have provided more accurate and precise measures of prevalence. Finally, only one measure of language development was used to measure the language skills of the child. Multiple measures may have provided a more accurate measure of the child's language development skills than a single assessment measure.
Nevertheless, the results of this study have implications for professionals involved in providing services to children. The study highlights the potential value of assessing and incorporating instructions for language development into treatment programs for preschool children. Research shows that developmental problems in early years are often precursors of problems in later life and early intervention programs are a promising way to facilitate favorable outcomes among children with multiple risks.[43,44] Moreover, recent studies indicate that the “wait and watch policy” used by professionals for children showing even uncomplicated expressive language delay can no longer be the norm, given the newer findings that majority of these delayed toddlers do not outgrow this delay.[44,45]
Several developmental programs have been launched by the Indian government to counter the deleterious impact of poverty and disadvantage in early childhood, the most comprehensive being the Integrated Child Development Services (ICDS). It provides counseling to pregnant and lactating mothers, growth monitoring for children less than 5 years of age, immunization, feeding, and preschool centers for children 3-6 years of age. Evidence indicates that the ICDS has improved the nutritional status and school attendance rates of preschool children, which are covered by this program.[46,47] To what extent these programs provide an impetus to the language development of young children, however, needs to be investigated.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil
References
- 1.Prathanee B, Thinkhamrop B, Dechongkit S. Factors associated with specific language impairment and later language development during early life: A literature review. Clin Pediatr (Phila) 2007;46:22–9. doi: 10.1177/0009922806297153. [DOI] [PubMed] [Google Scholar]
- 2.Glascoe FP, Dworkin PH. The role of parents in the detection of developmental and behavioral problems. Pediatrics. 1995;95:829–36. [PubMed] [Google Scholar]
- 3.Mallhi P, Singhi P. Screening young children for delayed development. Indian Pediatr. 1999;36:569–77. [PubMed] [Google Scholar]
- 4.Horwitz SM, Irwin JR, Briggs-Gowan MJ, Bosson Heenan JM, Mendoza J, Carter AS. Language delay in a community cohort of young children. J Am Acad Child Adolesc Psychiatry. 2003;42:932–40. doi: 10.1097/01.CHI.0000046889.27264.5E. [DOI] [PubMed] [Google Scholar]
- 5.King TM, Rosenberg LA, Fuddy L, McFarlane E, Sia C, Duggan AK. Prevalence and early identification of language delays among at-risk three year olds. J Dev Behav Pediatr. 2005;26:293–303. doi: 10.1097/00004703-200508000-00006. [DOI] [PubMed] [Google Scholar]
- 6.Tomblin JB, Records NL, Buckwalter P, Zhang X, Smith E, O’Brien M. Prevalence of specific language impairment in kindergarten children. J Speech Lang Hear Res. 1997;40:1245–60. doi: 10.1044/jslhr.4006.1245. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Law J, Rush R, Schoon I, Parsons S. Modeling developmental language difficulties from school entry into adulthood: Literacy, mental health, and employment outcomes. J Speech Lang Hear Res. 2009;52:1401–16. doi: 10.1044/1092-4388(2009/08-0142). [DOI] [PubMed] [Google Scholar]
- 8.Shetty P. Speech and language delay in children: A review and the role of a pediatric dentist. J Indian Soc Pedod Prev Dent. 2012;30:103–8. doi: 10.4103/0970-4388.99979. [DOI] [PubMed] [Google Scholar]
- 9.van Agt HM, van der Stege HA, de Ridder-Sluiter H, Verhoeven LT, de Koning HJ. A cluster-randomized trial of screening for language delay in toddlers: Effects on school performance and language development at age 8. Pediatrics. 2007;120:1317–25. doi: 10.1542/peds.2006-3145. [DOI] [PubMed] [Google Scholar]
- 10.Parakh M, Parakh P, Bhansali S, Singh GA, Parakh P, Mathur G. A clinico-epidemiologic study of neurologic associations and factors related to speech and language delay. Natl J Community Med. 2012;3:518–22. [Google Scholar]
- 11.Malhi P, Singhi P. Role of parents evaluation of developmental status in detecting developmental delay in young children. Indian Pediatr. 2002;39:271–5. [PubMed] [Google Scholar]
- 12.Glascoe FP. Nashville TN: Ellsworth and Vandermeer Press; 1998. Collaborating with Parents: Using Parents’ Evaluation of Developmental Status to Detect and Address Developmental and Behavioral Problems. [Google Scholar]
- 13.Sidhu M, Kaur J, Malhi P. Kolkata, India: Academy of Applied Psychology (IAAP); 2008. Feb, Developmental Profile of Young Children with Speech/Language Impairments. Paper presented at the 12th International and 43rd National Conference of Indian. [Google Scholar]
- 14.Newborg J. 2nd ed. Itasca IL: Riverside Publishing; 2005. Batelle Developmental Inventory. [Google Scholar]
- 15.Rescorla L, Alley A. Validation of the language development survey (LDS): A parent report tool for identifying language delay in toddlers. J Speech Lang Hear Res. 2001;44:434–45. doi: 10.1044/1092-4388(2001/035). [DOI] [PubMed] [Google Scholar]
- 16.Campbell TF, Dollaghan CA, Rockette HE, Paradise JL, Feldman HM, Shriberg LD, et al. Risk factors for speech delay of unknown origin in 3-year-old children. Child Dev. 2003;74:346–57. doi: 10.1111/1467-8624.7402002. [DOI] [PubMed] [Google Scholar]
- 17.Sidhu M, Malhi P, Jerath J. Multiple risks and early language development. Indian J Pediatr. 2010;77:391–5. doi: 10.1007/s12098-010-0044-y. [DOI] [PubMed] [Google Scholar]
- 18.Capute AJ. Baltimore MD: Kennedy Fellows Association; 1996. The Capute Scales (CAT/CLAMS) [Google Scholar]
- 19.Kumar N, Shekhar C, Kumar P, Kundu AS. Kuppuswamy's socioeconomic status scale-updating for 2007. Indian J Pediatr. 2007;74:1131–2. [PubMed] [Google Scholar]
- 20.de Koning HJ, de Ridder-Sluiter JG, van Agt HM, Reep-van den Bergh CM, van der Stege HA, Korfage IJ, et al. A cluster-randomised trial of screening for language disorders in toddlers. J Med Screen. 2004;11:109–16. doi: 10.1258/0969141041732229. [DOI] [PubMed] [Google Scholar]
- 21.US Preventive Services Task Force. Screening for speech and language delay in preschool children: Recommendation statement. Pediatrics. 2006;117:497–501. doi: 10.1542/peds.2005-2766. [DOI] [PubMed] [Google Scholar]
- 22.Carson D, Klee T, Perry C, Muskina G, Donaghy T. Comparison of children with delayed and normal language at normal language at 24 months of age on measures of behavioral difficulties, social, and cognitive development. Infant Ment Health J. 1998;1:59–75. [Google Scholar]
- 23.Toppelberg CO, Shapiro T. Language disorders: A 10-year research update review. J Am Acad Child Adolesc Psychiatry. 2000;39:143–52. doi: 10.1097/00004583-200002000-00011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Rescorla L. Do late-talking toddlers turn out to have reading difficulties a decade later? Ann Dyslexia. 2000;50:85–102. doi: 10.1007/s11881-000-0018-2. [DOI] [PubMed] [Google Scholar]
- 25.Stott CM, Merricks MJ, Bolton PF, Goodyer IM. Screening for speech and language disorders: The reliability, validity and accuracy of the General Language Screen. Int J Lang Commun Disord. 2002;37:133–51. doi: 10.1080/13682820110116785. [DOI] [PubMed] [Google Scholar]
- 26.Westerlund M, Sundelin C. Can severe language disability be identified in three-year-olds? Evaluation of a routine screening procedure. Acta Paediatr. 2000;89:94–100. doi: 10.1080/080352500750029149. [DOI] [PubMed] [Google Scholar]
- 27.Berglund E, Eriksson M, Westerlund M. Communicative skills in relation to gender, birth order, childcare and socioeconomic status in 18-month-old children. Scand J Psychol. 2005;46:485–91. doi: 10.1111/j.1467-9450.2005.00480.x. [DOI] [PubMed] [Google Scholar]
- 28.Galsworthy M, Dionne G, Dale P, Plomin R. Sex differences in early verbal and non-verbal cognitive development. Dev Sci. 2000;3:206–15. [Google Scholar]
- 29.Malhi P. Do women's literacy and work participation differentially affect male and female childhood mortality in North and South India? Guru Nanak J Socio. 1996;17:103–22. [Google Scholar]
- 30.Malhi P, Jerath JM. Women's status and gender bias: A case of North India. Guru Nanak J Socio. 1997;18:61–79. [Google Scholar]
- 31.Barnett MA. Economic disadvantage in complex family systems: Expansion of family stress models. Clin Child Fam Psychol Rev. 2008;11:145–61. doi: 10.1007/s10567-008-0034-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Burchinal MR, Roberts JE, Hooper S, Zeisel SA. Cumulative risk and early cognitive development: A comparison of statistical risk models. Dev Psychol. 2000;36:793–807. doi: 10.1037//0012-1649.36.6.793. [DOI] [PubMed] [Google Scholar]
- 33.Klebanov PK, Brooks-Gunn J, McCarton C, McCormick MC. The contribution of neighborhood and family income to developmental test scores over the first three years of life. Child Dev. 1998;69:1420–36. [PubMed] [Google Scholar]
- 34.Pike A, Lervolino AC, Eley TC, Price TS, Plomin R. Environmental risk and young children's cognitive and behavioral development. Int J Beh Dev. 2006;30:55–66. [Google Scholar]
- 35.Sameroff AJ, Seifer R, Barocas R, Zax M, Greenspan S. Intelligence quotient scores of 4-year-old children: Social-environmental risk factors. Pediatrics. 1987;79:343–50. [PubMed] [Google Scholar]
- 36.Stanton Chapman TL, Chapman DA, Kaiser AP, Hancock TB. Cumulative risk and low-income children's language development. Topics Early Child Spec Educ. 2004;24:227–37. [Google Scholar]
- 37.Walker SP, Wachs TD, Gardner JM, Lozoff B, Wasserman GA, Pollitt E, et al. Child development: Risk factors for adverse outcomes in developing countries. Lancet. 2007;369:145–57. doi: 10.1016/S0140-6736(07)60076-2. [DOI] [PubMed] [Google Scholar]
- 38.Buschmann A, Jooss B, Rupp A, Feldhusen F, Pietz J, Philippi H. Parent based language intervention for 2-year-old children with specific expressive language delay: A randomised controlled trial. Arch Dis Child. 2009;94:110–6. doi: 10.1136/adc.2008.141572. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Davis-Kean PE. The influence of parent education and family income on child achievement: The indirect role of parental expectations and the home environment. J Fam Psychol. 2005;19:294–304. doi: 10.1037/0893-3200.19.2.294. [DOI] [PubMed] [Google Scholar]
- 40.Magnuson K. Maternal education and children's academic achievement during middle childhood. Dev Psychol. 2007;43:1497–512. doi: 10.1037/0012-1649.43.6.1497. [DOI] [PubMed] [Google Scholar]
- 41.Sidhu M, Malhi P, Jerath J. Paper presented at the 3rd Annual Conference of the Human Development and Capability Association (HDCA) New Delhi, India: 2008. Sep, Impact of parental education on intelligence of children from low income families. [Google Scholar]
- 42.Walker SP, Wachs TD, Grantham-McGregor S, Black MM, Nelson CA, Huffman SL, et al. Inequality in early childhood: Risk and protective factors for early child development. Lancet. 2011;378:1325–38. doi: 10.1016/S0140-6736(11)60555-2. [DOI] [PubMed] [Google Scholar]
- 43.Engle PL, Fernald LC, Alderman H, Behrman J, O’Gara C, Yousafzai A, et al. Strategies for reducing inequalities and improving developmental outcomes for young children in low- and middle-income countries. Lancet. 2011;378:1339–53. doi: 10.1016/S0140-6736(11)60889-1. [DOI] [PubMed] [Google Scholar]
- 44.Shonkoff JP. Building a new biodevelopmental framework to guide the future of early childhood policy. Child Dev. 2010;81:357–67. doi: 10.1111/j.1467-8624.2009.01399.x. [DOI] [PubMed] [Google Scholar]
- 45.O’Hare AE. Wayward words and watchful waiting: Should clinicians be more proactive for the preschooler with uncomplicated expressive language delay? Arch Dis Child. 2009;94:80–2. doi: 10.1136/adc.2008.148528. [DOI] [PubMed] [Google Scholar]
- 46.Vazir S, Kashinath K. Influence of the ICDS on psychosocial development of rural children in Southern India. J Indian Acad of Appl Psychol. 1999;25:11–24. [Google Scholar]
- 47.Rao N. Children's rights to survival, development, and early education in India: The critical role of the integrated child development services programme. Int J Early Child. 2005;37:15–31. [Google Scholar]