

Abstract
CONFLICT OF INTEREST: NONE DECLARED
Distance learning refers to use of technologies based on health care delivered on distance and covers areas such as electronic health, tele-health (e-health), telematics, telemedicine, tele-education, etc. For the need of e-health, telemedicine, tele-education and distance learning there are various technologies and communication systems from standard telephone lines to the system of transmission digitalized signals with modem, optical fiber, satellite links, wireless technologies, etc. Tele-education represents health education on distance, using Information Communication Technologies (ICT), as well as continuous education of a health system beneficiaries and use of electronic libraries, data bases or electronic data with data bases of knowledge. Distance learning (E-learning) as a part of tele-education has gained popularity in the past decade; however, its use is highly variable among medical schools and appears to be more common in basic medical science courses than in clinical education. Distance learning does not preclude traditional learning processes; frequently it is used in conjunction with in-person classroom or professional training procedures and practices. Tele-education has mostly been used in biomedical education as a blended learning method, which combines tele-education technology with traditional instructor-led training, where, for example, a lecture or demonstration is supplemented by an online tutorial. Distance learning is used for self-education, tests, services and for examinations in medicine i.e. in terms of self-education and individual examination services. The possibility of working in the exercise mode with image files and questions is an attractive way of self education. Automated tracking and reporting of learners’ activities lessen faculty administrative burden. Moreover, e-learning can be designed to include outcomes assessment to determine whether learning has occurred. This review article evaluates the current status and level of tele-education development in Bosnia and Herzegovina outlining its components, faculty development needs for implementation and the possibility of its integration as official learning standard in biomedical curricula in Bosnia and Herzegovina. Tele-education refers to the use of information and communication technologies (ICT) to enhance knowledge and performance. Tele-education in biomedical education is widely accepted in the medical education community where it is mostly integrated into biomedical curricula forming part of a blended learning strategy. There are many biomedical digital repositories of e-learning materials worldwide, some peer reviewed, where instructors or developers can submit materials for widespread use. First pilot project with the aim to introduce tele-education in biomedical curricula in Bosnia and Herzegovina was initiated by Department for Medical Informatics at Medical Faculty in Sarajevo in 2002 and has been developing since. Faculty member’s skills in creating tele-education differ from those needed for traditional teaching and faculty rewards must recognize this difference and reward the effort. Tele-education and use of computers will have an impact of future medical practice in a life long learning. Bologna process, which started last years in European countries, provide us to promote and introduce modern educational methods of education at biomedical faculties in Bosnia and Herzegovina. Cathedra of Medical informatics and Cathedra of Family medicine at Medical Faculty of University of Sarajevo started to use Web based education as common way of teaching of medical students. Satisfaction with this method of education within the students is good, but not yet suitable for most of medical disciplines at biomedical faculties in Bosnia and Herzegovina.
Key words: Medical education, Distance learning, Bosnia and Herzegovina
1. MEDICAL EDUCATION: CONCEPTS, PROGRAMMES, 1. METHODS
Medical education is considered a very significant strategy in ensuring the quality of health protection. It represents the most dynamic structural element of good quality of protection (1,2,3).
The term medical education means acquiring knowledge and psychological/motoric skills, while medicinal training means acquisition of positive values and attitudes (4).
Medical education and training is not good unless the student acquired the nucleus or the minimum knowledge (cognitive aspect), the minimum of required skills (psychological/motoric aspect) and minimum of obligatory conduct values (affective aspect)(4).
The role of a doctor is to be an organiser, communicator and therapist in the following five activities:
health promotion,
disease prevention,
treatment of the diseased,
rehabilitation of the recovered,
constant learning.
The World Medical Association defined medical education principles adapted at the assembly in Madrid in 1987.
1.1. Medical education principles are the following:
Basic Medical Education Principles medical education includes education leading to the first professional degree (the title of the General Practitioner or GP), clinical education which is the preparation for general medical practice or specialty and obligatory continuous, life-long education of each doctor.
Profession, University and other educational institutions as well as the government share responsibility for guaranteeing high standards and quality of medical education (1,2,3,4,5,6,7,8,9)
Undergraduate Medical Education
The aim of medical education is to educate doctors who are entitled to practice their profession with no restrictions, based on what they learned.
The first professional degree means completing the curriculum which qualifies the student for a range of difference choices in his/her career, including the treatment of the diseased, public health service, clinical and basic research, or further medical education. Any further career choice requires additional education apart from that leading to the first professional degree.
University Education
Undergraduate education has to be led by a well-organised university. The university has to have adequate academic qualifications which can be achieved only through theory and practice.
The selection of university should be based on individual qualifications regardless of age, sex, race, nationality, religion pr political orientation.
The university is responsible for creating an academic environment where learning and research can progress in the optimal manner. For the purpose of improvement of medical knowledge and providing the best quality of health protection, active medical research, as such, has to be performed under academic conditions, in order to meet the highest medical standards.
The aim, programme, form and assessment of educational experience are included in the responsibility of universities with the participation of the national medical association.
The university is responsible for providing the obligatory basic curriculum in a free academic environment where learning and research will progress in the best way possible. Given the needs of the community and practitioners’ participation, the curriculum has to be frequently revised, in order for the extent of community needs not to reflect in the medical education quality. Recognition of the university requires the availability of the library fund, research laboratories, clinical capacities and reading rooms to a sufficient degree in order to meet the needs of each student.
In addition, appropriate administrative structure. Moreover, there should be adequate academic structure, and appropriate scientific records should be kept.
When all the necessary elements are available, clinical education of future GPs and specialists can be sponsored by either the university or the hospital.
Medical Education Programme
Education process should include both biological and social sciences as a social/economic aspect of health care. These sciences are a basis for understanding clinical medicine. Critical opinion and self-education as well as solid ethical principles the profession is based on are also required.
Clinical education
The clinical component of medical education has to be focused on patient examination and include direct experience in the diagnostic and disease therapeutic treatment. The clinical component should include personal diagnostic and therapeutic experience with gradual access to higher responsibility.
Care should also be taken of the adequate number of training participants and teachers which would be present at each patient’s bed.
Before he/she starts working independently, each doctor should complete a formal programme of clinical education. The programme, taking usually a year, should be characterised with supervision, gradual increase of responsibility and solving clinical problems.
University is responsible for making sure that students who achieved their first professional degree get basic clinical medicine knowledge, basic skills for solving clinical problems and that adequate and timely steps are taken as well as that they have an ethical position and character.
Student Selection
Broad general education is quite desirable prior to enrolling for medical studies. Students should be selected based on their intellectual abilities, motivation, prior education and character. The number of enrolled students may not exceed the number of students the university is capable of educating as regards available material resources and community needs. Student selection may not be conditioned by students’ age, sex, race, religion, political orientation or nationality.
Post-Graduate Medical Education
It is desirable for each doctor to enrol in postgraduate studies upon completing his/her undergraduate education and choose a specialty in treatment of the diseased, public health service, clinical or basic research or medical education. The formal programme of clinical education should be preceded by independent work i.e. without supervision in the general medical practice or a specialty. Medical profession is responsible for upgrading the programme of clinical education which is met after undergraduate studies.
Continuous Medical Education
Doctors are destined to lifelong learning. Education experience is important if doctors want to keep up with medical progress and if they are aware that only knowledge and skill can ensure a high quality of health care; scientific achievements are important for providing adequate health care to people.
1.2. Bologna Process
Demand fro health care provision, disease treatment and medical advice requires the highest standards of undergraduate, post-graduate and continuous medical education.(3)
The aim of Bologna process is harmonisation, and therefore it is not a path to “standardisation” or “equalisation” of higher education in Europe. The basic principles of autonomy and diversity are respected (6,7,8).
In addition to legal reforms undertaken by governments of signatory countries, in certain higher education fields, the goal is to achieve shorter study period, double grading structures, grading system, external evaluation and higher autonomy with responsibility. Another trend refers to erasing boundaries between different integral subsections of higher education, and preparing a common teaching plan and programme, organising joint journeys in trans-Atlantic countries and the scheme of degree recognition all over the world.
The deadline for providing European conditions for higher education is 2010. In order for Sarajevo universities to meet current requirements and trends of ‘’Europeisation’’ of teaching plan and programmes, that is, teaching programmes and methods and methodologies and their realisation relatively quickly, one of the basic tasks and goals, advocated, among other things, with the Bologna process principles is adequate and continuous assessment of the quality of realised lessons, their contents and those conducting the teaching process. Modern, ICT-supported education and at the sae time internal and external evaluation of teaching process quality by adequate quality variables is advocated. The variables have not been defined yet by adequate and relevant experts at our faculty and the University, and there are no such standardised variables in current laws and bylaws at the Sarajevo University or other universities in BiH (1,5,6).
2. INFORMATION AND COMMUNICATION TECHNOGOLGIES IN BIOMEDICINE
2.1. The Role of the Internet in the Communication System
The Internet is an infrastructure connecting computers by telecommunication, i.e. the Internet is a world computer network. This literally means that this is the biggest network in the world connecting millions of PCs, local (LAN) and wide (WAN) are network in a single network. Computers and particular networks are connected to the Internet in different ways. Thus there are several types of connections used by the Internet. Computers in a network can be connected by coaxial cable, optical cable, telephone lines, radio waves, satellite, laser links etc.
The Internet can be defines as a work computer information network, consisting of a large number of smaller interconnected computer networks, enabling information transfer between computers in a network. Therefore, the Internet could be defined as a network of all networks. This factually means that it is the largest network connecting millions of personal computers, LANs and WANs in a joint network. Computers and networks are connected in different ways. There are several types of Internet connections. On one hand, an average user in most parts of the world connects to the Internet by a modem. On the other hand, there are computer connections by so-called servers, hosts or nods. They are in most cases especially strong computers capable of processing enormous quantities of data, and it is exactly by this means that people connect to the Internet through a modem. Servers are most often integrated in a network by satellite and radio connections and fiberoptic and telephone cables. Those computers are connected by specialised computers called routers. Routers check where data moving in the Internet are directed and determine which way to send them through (10,11,12,13,14,15).
2.2. Internet in Medicine and Medical Education
One of especially significant new ICT-a is the Internet, a world wide computer network connecting millions of computers and ensuring the use of a set of network instruments called the World Wide Web (or shortly Web). It is often said that expansion of the Internet is comparable with the significance of Gutenberg’s discovery of printing technology. While printing accelerated manipulation of information stored by then in the form of hand-written texts, the Internet enormously accelerated information manipulation by applying the today’s electronic technology. In this manner, an unforeseen extent of access to information generated all around the world in various fields of human activity is allowed, which greatly affects medical science and everyday work as well (9,10,11,12,13).
By late 1994, the Internet included 3.2 million computer nodes spread across more than 57,000 institutions in more then 80 countries, with an estimated 30 million users. By the end of the century the Internet linked more then 400 million persons.
The 2002 Eurobarometer survey showed that an average of 78% of EU medical GPs were online, with at the highest level – 98% in Sweden and 97% in United Kingdom. Number of “online patients” grows every day as well. The 2003 Eurobarometer survey on health information sources shows that 23% of Europeans use Internet for health information and that 41% of the European population considers that Internet is a good source of information on health (3).
2.2. Internet Development
The development of the Internet as a global network primarily depended on the development of communication means. Invention of telegraph, telephone, radio and computer was the basis for Internet creation. Therefore, it is no wonder that the Internet was invented in the second half of the 20th century, at the time of high tension between the East and the West. It is this constant war danger that gave birth to a desire to be ahead of the opponent, which gave the world various products and technological innovations which would never have been possible if Cold War had not taken place. Thus some historians think the Internet is one more side effect of the War. The Internet was established in 1969, when ARPA (Advanced Research Projects Agency), founded and financed by the American government within the USA Ministry of Defence was assigned with a task to redesign the manner in which computers function. The result of this work was the creation of ARPANET, the first computer network. ARPANET was originally designed for enabling high efficacy in communication among the USA research centres, universities and governmental organisations and soon grew into an international network available to everybody (16,17,18,19,20).
The Internet development can be viewed in the following chronology:
1969 – the USA Ministry of Defence builds the first test network and ARPANET is created;
1971 – Ray Tomlinson creates the first programme for electronic mail and E-mail is created;
1972 – Telnet is developed which allows work on distant computers;
1973 – FTP (File Transfer Protocol) is established which becomes the standard for data transfer within the network;
1979 – USENET news server network with thematic groups is created;
1983 – TCP/IP protocol is standardised and the term ‘INTERNET’ as a name for a ‘network of all networks’ is first used;
1986 – NNTP (Network News Transfer Protocol) becomes the standard for the connection between news servers connected in the USENET network on the Internet;
1989 – the number of computers exceeds 100.000.
1991 – the WWW (World Wide Web) is developed, and the number of computers connected to the Internet exceeds 1 000.000.
Expansion of Internet use in medicine is truly spectacular. If we take the expansion of the number of papers with the Internet as descriptor in the Medline bibliography data base as an indication, we find that from one paper recorded in 1991 the number of prepares exceeded one thousand in 1998, and till the end of 2002, that is, a bit more than a century, 14.000 papers on the Internet in medicine and medical practice were published. Apart from the fact that more and more papers on the Internet in medicine were written, there were also first bibliography lists aiming at making medical IT experts as well as a broader medical community familiar with the Internet. The following was ensured in medicine by the Internet:
“doing old things in a new way”, (1)
“doing new things” (2)
“contributions beyond the field of medical IT science”.(3)
In the set of purposes under Item (1), any person who connected to the Internet was allowed to access a great number of data bases with bibliographic, epidemiological, pictorial and other medical information. Health assessment and medical decision-making systems, with a series of expert systems and clinical work support systems became directly accessible, and its application in medical lessons expanded. The new possibilities under Item (2), especially included e-publishing, the development of new graphic methods for data viewing and direct real-time monitoring, which is considered particularly significant for clinical practice. The Internet allowed the development of new methods for clinical workers’ cooperation, consultation and debates, as well as electronic communication between the patient and the doctor. The contributions under Item (3) include data security and confidentiality issues of the broader community, and data management based on medical ethics principles.
The Internet period in medicine has shown that the exponential increase of medical data and knowledge is still a major problem in medicine. It was noticed that, while the quantity of information grows, the capacity of their assimilation, nevertheless, does not. It is understood that the contemporary development and trends induce deep impact on the role of the public in making one’s own health decisions. At the end of the 20th century it became clear that information revolution, triggered by the Internet, will seriously reflect on medicine, as well as in other disciplines. With the Internet, information on health was no longer available exclusively to health workers, because they became accessible to the public. The growth was so fast, which was reflected in both the increase in the quantity of information and in the number of its users, and proportionally, more patients than doctors had Internet access. It proved that health care information on the Internet is of significant use to patients. All this is a challenge for both information users and creators, and various issues started coming up, such as information quality, privacy, the rights of use etc. Thus the traditional manner of interaction between patients and doctors started changing, since patients became able to access making decisions on his/her treatment and participate in the active partnership with various groups of decision-makers (doctors, politicians and researchers). Internet use became necessary in health care as well, and in one of expert medical magazines the following message was published for doctors “Get online–or get left behind”.
2.3. Traditional vs. Modern (Web-Based) Medical Education Concept
The traditional static concept of medical education should be changed into the dynamic. A passive doctor who is to be compelled to education becomes a creative doctor focused on a problem he/she wants to solve in practice (self-directed). At the same time, medicine incorporates its part of electronic revolution.
Expansive development of biomedical sciences put each doctor in a situation to get information on latest medical achievements with delay and apply a relatively out-of-date technique in treatment – meaning, he/she makes mistakes. Continuous medical education (CME) should decrease the unavoidable delay. In many countries, continuous education is structured and compulsory, but it stimulates free selection of problems and activities in specialisation as a new cultural model (14,15,16,17,18).
Continuous medical education is an opportunity for interactive exchange of knowledge, positions and experience during which a doctor checks and modifies his/her perception on what kind of a doctor he/she is, and the kind of doctor he/she should be. The extent of this discrepancy dictates the need for changes and motivates the change of conduct, for a start. Considering continuous medical education first occurred as a response to expressed doubt in some doctors’ professionalism.
It is considered today that each doctor or a senior medical student medicine becomes an educator in further professional process (for younger colleagues, nurses, personnel, patients and people in general). Each doctor is “role-model” in his/her work. He/she should accept the responsibility immanent in competency development and exert constructive influence on his/her environment. Only in the USA, there are around 100 web sites offering on-line continuous medical education courses.1
The number of continuous medical education requests increase when education and education technology are significantly developed. Such development is allowed today by the CME for better meeting of CRISIS criteria for effective continuous medical education as follows: convenience, relevance, individualisation, self-assessment, independent learning and systematic approach. The International Virtual Medical School (IVIMEDS)2 provides a case study illustrating how fast development of the Internet and e-learning can change undergraduate medical education and the possibility of changing the nature of CME.3
2.4. The Internet and Telemedicine
In addition to information and education, there are new possibilities of the use of the Internet and network technologies in medicine: telemedicine is a term for distance medical procedure, pertaining to both diagnostic and therapeutic procedure or to distance support in decision-making, which is nowadays realised in practice more by doctors’ consultation with their specialist colleagues in specialist and hospital institutions for the purpose of solving medical problems in certain cases, where in synchronous and asynchronous communication pictorial and other records and findings are often exchanged. Moreover, today a doctor and his/her patient can communicate through a network, which shall probably be more used in the future, and systems for distant patient monitoring (e.g. at home). All this should improve the quality of doctors’ work. Despite the possibilities provided by the contemporary ICT to doctors in finding and exchanging information on medicine and health care, its application is still far from a level it actually deserves. The reasons for this are numerous and they refer to technical preconditions for ICT use, including (non)-possession of equipment and (non)existence of computer skills on the part of the doctor, as well as of other health care personnel, on one hand, and sensitivity of procedure and information exchanged in health care, which require the introduction of new registries and organisational solutions, on the other. Technical possibilities for faster telemedicine development already exist, and organisational and infrastructural solutions are yet to be developed, where one of the major obstacles is insufficient IT literacy, especially of older generations of doctors, caused by a low level of computer use. One of rare published researches indicates that, even recently, only 10% of family doctors used the computer, and only 5% used the Internet, and mostly for e-mail and information source searching. It should be noted that, according to the same research, doctors were mostly motivated to use the Internet and search the Web by the need to solve their patients’ medical problems (3,6,19,20,21,22).
Information technologies in medicine and health care represent all medical technologies in health care activities, of which work process, supervision and evaluation are performed by computer technologies.4
We have recently been witnesses of an impressive progress of information and telecommunication technologies. The use of computers in medicine allows permanent data storage, data transfer from one work station to another, data searching and processing, data availability at any moment, monitoring the patient’s condition during time etc. can significantly improve medical profession. Nowadays, medicine is one of the most intensive users of all types of information and telecommunication technologies. Fast and reliable data storage and transfer (text, images, sound etc.) ensures significant relief and improvement in almost all medical procedures. Moreover, data transfer to places remote from medical centres can be of invaluable use, especially in emergencies.
Information technologies are becoming a tool today without which further education of both medical students and doctors is not possible, since the quantity of information and the need for their fast search have become possible only by using these technologies. Today it can be freely claimed that a bad doctor is the one who does not use information technologies, because he/she does not new facts which might mean a lot to his/her patients in time.
2.5. Internet in the Future
IT long proved to be by far the most unpredictable of all human activities. Therefore, any forecast related to computer industry is a more or less a struggle doomed to be lost. From the very beginning, the glorious future of the Internet could not be foreseen by anyone. Thus “great experts” claimed that it will never be possible to connect PCs to the Internet since Internet Protocols are too complex for performance on such machines. Furthermore, it claimed that the WWW will never achieve the popularity of Gopher (WWW precursor). We can only speculate today which direction the Internet will develop. Its future will surely depend on the future of the Web. Internet connections will certainly improve on a daily basis, and the WWW will increasingly be introduced in households. For this, the growth of financial exploitativeness of the Internet is important which is a basic precondition for further investments in the very infrastructure of the Internet without which the Web would be otherwise worthless. It is already not early to say that in 10-15 years most world population will, if nothing else, at least be able to send an e-mail and use the WWW. Why? Primarily because its possibilities are almost immense. We can already buy a book, a car or a computer via WWW. We can study, watch films, listen to the radio and TV programmes operation only on the Internet, we can do gardening with a robot, browse VRML photos of an apartment we want to buy, play games with about 30 people at the same time, exchange all types of information etc. in a nutshell, the Web possibilities are unlimited (23,24,25).
Expansion of the Internet use in medicine is undoubtedly a very dynamic process where all participants gave a fantastic contribution with noticeable results and immense possibilities in the future.
Its future will surely depend on the future of the Web. Internet connections will certainly improve on a daily basis, and the WWW will increasingly be introduced in households. For this, the growth of financial exploitativeness of the Internet is important which is a basic precondition for further investments in the very infrastructure of the Internet without which the Web would be otherwise worthless. It is already not early to say that in 10-15 years most world population will, if nothing else, at least be able to send an e-mail and use the WWW. (7/8)
Internet security is definitely one of the biggest problems of the Internet. Of course, here we can refer to different types of security. Due to decentralised Internet system which is a pretty stable, the danger of collective subversion of the entire system is slight. On the other hand, the most serious problem is security of networks of companies and various governmental associations intruded by hackers. This is within the financial crime domain and the increase of this security is one of important issues for financial survival of the WWW. Internet security is taken care of by the CERT (Computer Emergency Response Team) which records and tries to suppress system intrusions.
3. LEARNING RESOURCES SUPPORTING TELE-EDUCATION
Thanks to the growth of educational technologies and the Internet, the number of online resources available to educators has dramatically increased. Within medical education, repositories or digital libraries have been established to manage access to e-learning materials. Although few at this time, such repositories offer a vision of expanded access to a large number of high-quality, peer-reviewed, sharable e-learning materials (6,8,10) (Table 1).
TABLE 1.
Medical organizations supporting tele-education
| MedEdPortal, Assosiation of American Medical Colleges (AAMC) http://www.aamc.org/mededportal |
Repository All digital content types Material linked to educational competencies Peer reviewed” Virtual patients” |
| End of Life/Paliative Education Resource Center (EPERC) http://www.eperc.mcw.edu/ |
Repository Digital content in end-of-life issues Peer reviewed Links to other online resources |
| The Health Education Assets Library (HEAL) http://www.healthcentral.org/ | Repository Large number of learning assets Growing number of learning objects Peer reviewed. |
| Multimedia Educatiuonal Resource for Learning and Online teaching (MERLOT) http://www.merlot.org/ |
Repository for higher education Links to other online resources with peer-review comments Growing science and technology section |
| International Virtual Medical School (IVIMEDS) http://www.ivimeds.org/ Master thesis of dr. Bernard Sklar – http:// www.cmelist.com |
A consortium of medical schools Setting standards in medical education Repository for member schools Review of sorts of E-learning teaching materials for retrieving |
Examples include the Association of American Medical Colleges’ (AAMC’s) MedEdPortal, a repository for curriculum and assessment materials organized around core competencies in medical education and populated with up-to-date, peer- reviewed teaching and assessment materials (11) (Figure 1).
FIGURE 1.

Association oof American Medical Colleges wesite
The End of Life/Palliative Education Resource Center is a free- access repository of digital content for health profession educators involved in palliative care education (12).
The health Education Assets Library (HEAL) provides high-quality digital materials for health sciences educators (13) and promotes the preservation and exchange of useful educational assets such as individual graphic, video, or audio elements, while respecting ownership and privacy. HEAL has begun a peer-review process for all e-learning materials submitted to the library. (13)
The Multimedia Educational Resource for Learning and Online Teaching (MERLOT) is designed primarily for faculty and students of higher education (14). The service collects links to online learning materials, along with annotations such as users’ reviews and assignments. MERLOT contains a growing science and technology section that includes health care education e- learning materials (14).
The International Virtual Medical School (IVIMEDs) is an international organization whose mission is to set new standards for e-learning in medical education through a partnership of medical schools and institutions, using a blended-learning approach. IVIMEDS hosts a repository for use by its member medical schools (15). Most of the materials in this repository are free to use, although some materials have clearly defined conditions for use (figure 2).
FIGURE 2.

IVIMEDS website
4. HISTORICAL BACKGROUND OF E-LEARNING IN BOSNIA AND HERCEGOVINA
Teleeducation and distance learning in Bosnia and Herzegovina has made a great progress (4). Possibilities of introduction of distance learning in medical curriculum are the title of project which has been realizing at Department of Medical Informatics, Medical Faculty since year 2002. The Project was approved by Federal and Cantonal ministries of science and education. The purpose of this project was to support improvement educational process at biomedical faculties using contemporary methods, methodologies and information technologies in accordance with strategy and objectives given by Bologna declaration. The pilot project realized during three years, the theoretical and practical parts of the subject Medical Informatics are adapted to modern concepts of education using world trends of distance learning. One group of students from the Medical Faculty was involved in this project, which was finalized by electronic registration of an exam and electronic testing on 20 June 2005, in public in the Physiological amphitheatre of the Medical faculty in Sarajevo (6,7,8). The Bologna process which started in last years in European countries, enable us to promote and introduce modern educational methods of education at biomedical faculties in Bosnia and Herzegovina. The Cathedra of medical informatics and the Cathedra of Family medicine at the Medical Faculty of the University of Sarajevo started to use web based education as a common way of medical students teaching (6). Lecture contents are presented in a virtual classroom. In this “classroom”, learning materials, power point lecture presentations as well as practice exercises with step-by-step instructions, are easily accessible to students. Moreover, on this web site, students will be able to find subject relating literature as well as the English version of the presentations (8). Satisfaction with this method of education within the students is good, but not yet suitable for most of medical disciplines at biomedical faculties in Bosnia and Herzegovina. (4). Web sites of the Cathedra for Medical Informatics and Family Medicine are shown in figure 3.
FIGURE 3.
Website of Cathedra for Medical informatics at Medical Faculty in Sarajevo
Platform of the course for distance learning was established in collaboration with University tele-information Center (UTIC).
UTIC, established as part of University of Sarajevo and first ISP in Bosnia and Herzegovina in 1996. it is a scientific-organizational unit of the University of Sarajevo for improvement of scientific-research work. UTICs objectives are among many to develop an integration of of informatics computer technologies in education, to create flexible infrastructure which will enable e-Learning to be accessible to all student at the University of Sarajevo, improvement of digital literacy of academic population, development of top educational content which could be integrated in the actual European process of e-learning revolution. With their help center for distance learning “LUCIS CENTRUM” was created (6).
On UTIC web site , seven students enrolled at Medical Faculty, are able to learn from distance about Medical Informatics subject. so far, teaching staff uploaded eleven lectures at the web site. Besides the learning material it is possible to upload and download the following: practical and seminar works, links, plan and program, quiz, schedule examination results (16) figure 4.
FIGURE 4.
Screenshot of student exam interface
Bosnian society for Medical Informatics (BHSMI) is very proactive in promoting telemedicine and teleeducation as part of it and last organized was a special Topic Conference named eHealth and eEducation in December 2005 (1) with support by International society for Telemedicine and e-Health, which till now organized 12 world Congresses of Telemedicine on all continents. Our society (www.bhsmi.ba) is member of this scientific association since 2005.
5. DISTANCE LEARNING AS MODERN METHOD OF MEDICAL EDUCATION
Distance learning is conventionally defined as: any educational or learning process or system in which the teacher and instructor are separated geographically or in time from his or her students; or in which students are separated from other students or educational resources (1,2,3). The most important factor which influences the changes occurring in education has been the installation and development of the Internet and electronic multimedia techniques. Distance learning does not preclude traditional learning processes; frequently it is used in conjunction with in-person classroom or professional training procedures and practices.
Distance learning is used for self-education, tests, services and for the examinations in medicine, i.e. in terms of self-education and individual examination services. The possibility to work in the exercise mode will image files and questions is an attractive way for self-education (4,5,6,7). The standard format of the notation files enables to elaborate the results by commercial statistic packets in order to estimate the scale of answers and to find correlation between the obtained results. The method of multi-criterion grading excludes unlimited mutual compensation of the criteria, differentiates the importance of particular courses and introduces the quality criteria. By using computers and teleconferencing technology and through partnerships with local communities, institutions and the private sector, an open, effective, virtual learning community is now in place. sites are located in college and university campuses, hospitals, schools, libraries, community centres and private companies. Courses are also being delivered to private homes.
For the need of e-Health, telemedicine, and Tele-education there are various technologies and communication systems from standard telephone lines to the system of transmission digitalized signals with modem, optical fibber, satellite links, wireless technologies, etc. There is no doubt that Internet causes “revolution” in all above, and the latest its possibilities are distribution of virtual medical instruments and medical data in real time and possibility of use in primary health care, even for some diseases with bed prognosis. This revolution how information is stored, transmitted and accessed has extremely important implication for the health sector, especially now when embarking on a global effort to renew the tenets of health for All based on primary health care and disease prevention, health promotion and costumer education, in the context of service delivery guided by the equity, quality, effectiveness and efficiency. According to Grimson at al in Dublin, “the need to participate in continuing professional development or continuing medical education is considered to be at the very least highly desirable and more likely mandatory. The use of Information Communication Technologies (ICT) is one way by which this can be facilitated in a timely and cost-effective manner” (7,8,9,10,26,27,28,29,30).
5.1 Traditional way of learning and learning from the distance
The latest researches shows that the format of instructions itself has no important influence on the students’ achievements if access and availability to information technologies is assured as well as usage of the adequate content of education. In the assessment of the authentic situation the following issues should be addressed:
Results of different tests prepared by lectors has trend to show advantages in comparison with traditional learning methods and there is significant distinction in affirmative attitude to educational materials between distance and traditional learning
Traditional methods demonstrate better organization and they are clearer in respect to distance learning
Organization and needs for more efficient influence of distance learning very often improve traditional methods by teachers
Future research should be focus on critical factors in determining student involvement in development of educational process.
The variety of teaching and learning options provided by technology allows education to be provided in an appropriate manner to a broader student demographic then ever before.
5.2. Facts about Distance learning (E-learning) and Tele-education
Distance learning enables permanent learning (lifelong learning), students can improve themselves professionally and independently, at their own tempo, at place and time that they choose by themselves, they can choose great deal of subjects which offer different institutions, teachers-individuals; students go through materials for learning by speed of their own and as many times as they want. The place can be chosen – it depends on media which is used for learning material (they can learn at work or from home). Themes access which are not offered by studies in that field – students find and attend the programs which they are interested in, although they are not offered by educational or business institutions in place where they live in or work. Taking part in top-quality and most prestigious programs – student can “attend” at least some studies at the top-quality institutions or studies held by lecturers that are very famous experts without changing their place of living. Choosing this way of learning – active or passive learning, different kinds of interaction: “Classical” written material and writing down their own lecture notes, interactive simulations, discussion with other students (e-mail, Teleconferences).
Practical work with different technologies – they get not just information about that they learn, but additional knowledge and skills about using computer, CD players and video recorders. Independent learning – teachers learn too from students who independently ask for information source.
The meaning of education (learning) to distance can be expressed by the definition: That is a form of education which is in process permanently, or most of the time, all or most of the tasks of teaching and learning separately during the time and space between teacher and student. Pedagogical and organizational improvements have fundamental importance. It is in use both interaction teacher – student and interaction student – student. Phases of synchronized and synchronized learning are combined. Individual and group works are also combined. If all these forms are involved in educational process, they mutually supplement each other, as a last resort. Traditional education as well as contemporary education is supported by informatics technologies in unique system of flexible education. In order to use advantages of flexible education, it is necessary to combine different forms of learning, during the preparation phase and development of every educational course in appropriate way.
Distance learning is not simply a set infrastructure, but rather a concept of learning that incorporates different technologies and learning media. Within the province, different video, audio and computer teleconferencing systems, along with Computer Based Training, Computer Managed Instructional systems and other media are being integrated technologically, instructionally and organizationally. The Tele-education concept crosses all jurisdictions among institutions both within and outside the province, public and private, at any level of education, to anywhere including institutions, workplaces and the home. Tele-education, Tele-teaching, Tele-training, Tele-mentoring, and Tele-accreditation have been clearly demonstrated and are now common practice.
5.3. Implementation of E-learning in medical curricula at Medical faculty, University of Sarajevo
In spite of fact that Bosnia and Herzegovina is last or second before last country in Europe in use of Internet technologies, there is a group of enthusiastic people accompanying prof. dr. Izet Masic at Medical Faculty and University of Sarajevo who have been making significant effort to improve poor digital literacy in the University and among medical professionals. E.g. every 60th citizen of Bosnia and Herzegovina uses Internet (50.000 citizens of 3.000.000 citizens in Bosnia and Herzegovina) and in Slovenia every forth Slovenian is familiar and uses Internet technologies (31,32,33,34,35,36,37,38,39,40).
In October 2003, University of Sarajevo began with Distance learning education, opening University Distance Learning Centre. Opening the University Distance Learning Centre, as coordination body and leader in all activities in connection to Distance learning, has provided opportunity for development and growth of this kind of lifelong education (6,8).
In correlation with above project conducted by the University Tele-information Centre (UTIC) and as continuation of two-year project Possibilities of introduction of Distance learning in Medical curriculum, the Cantonal Ministry approved and supported a new project; Introduction and implementation of Distance learning in medicine. Platform for the course of distance learning is achived in collaboration with UTIC. University Tele-information Centre, established as part of University of Sarajevo and first ISP in Bosnia and Herzegovina in 1996 (www.utic.net.ba). It is scientific-organizational unit of the University of Sarajevo for improvement of scientific-research work and through UTIC members of the University can be gathered in the unique computer-communication structure. ). Objectives of UTIC are: to connect members of the University with similar institution in the country and abroad due to more efficient use of scientific, research and educational resources, use of educational data bases and other information for the needs of the University and its members. Also, development an integration of informatics computer technologies in education, creation of flexible infrastructure which will enable e-Learning to be accessible to all students and University staff, improvement of general digital literacy of academic population, development of top quality educational content which could be integrated in the actual European processes of e-Learning revolution. With their help center for distance learning, “LUCUS CENTRUM”, is created (Figure 4). We hope that this is just a beginning step towards improvements of the B&H education system and that this project will serve as an indicator towards that future.
On UTIC web site, seven students enrolled from Medical faculty, for the subject Medical Informatics are able to learn from the distance location. so far, teaching staff uploaded eleven lectures at the web site: hardware and software, Medical documentations, Medical informatics, Methods of data manipulation, Nomenclatures and classification systems, Data organization, Data, information and knowledge, Lectures 1, system and communication, structure and data organization and Expert systems. Beside the materials it is possible to upload and download the following: Practical works, seminar work, Information, Recommended links, Plan and programs, Quiz, schedule, Recommended readings, Examination schedule and Examination results.
Basically software application has two interfaces: teacher and student interface. Access from any of these is very simple and fast (1,6,8).
5.4. Education content OF DISTANCE LEARNING
Lecture contents will be presented in our virtual classroom. In our case, learning material from the subject of medical informatics, and later, hopefully from other medical subjects, will be available on web site, www.e-learning.ba
In this “classroom,” learning materials, power point lecture presentations as well as practice exercises with step-by-step instructions, are easily accessible to students. Moreover, on this web site, students will be able to find subject relating literature as well as English version of the presentations. To access this information requires only one click on a download option (Figure 5.) as well as one second patience depending on student’s internet speed connection. In short, our virtual classroom gives students the opportunity to access needed information, at any time, and in any place without having to be bound to the classroom. Student is able to browse through the “classroom” using standard navigations. Using these simple navigations, maximal efficiency and fast access to needed material is possible.
FIGURE 5.
Uploaded materials for subject Medical Informatics
As we can see on the picture, all links are in chronological order according to the plan and program of the lecture as well as practice. special attention is given to the link “kvizovi”.
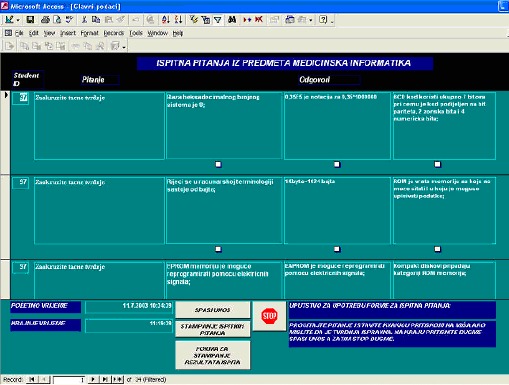
In order for the student to check his/hers progress (to test his/hers knowledge of the lecture he/she studied), every lecture is followed by quizzes. Quiz questions are multiple choice questions) and they are based on the lecture content. After every quiz, student receives “feedback” regarding his/hers progress. Results are given in terms percentages (one needs 51% right answers to pass the quiz). On this way student has absolutely control over his/hers work. When students passed lectures, tested themselves a few times, officially can make exam electronically (Figure 6 and 7) using special created data bases with more then 1.000 questions (multiple-choice) covered by subjects from the Medical informatics books 1 and 2, written by Izet Masic and Zoran Ridjanovic (Avicena, Sarajevo, 2004).
FIGURE 6.
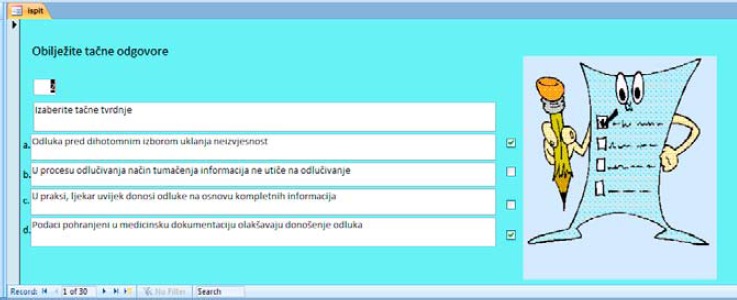
Screen window of exam questions
FIGURE 7.

First electronic exam and held on 20 June 2005, publicly, in the Physiology amphitheatre of the Medical faculty in Sarajevo, Bosnia and Herzegovina
5.5. Electronic Examination
Both part of exam are performed using computers. Students must perform some of the task that includes preparation of information that should be analyzed, gathering of data, data manipulation, and finally analysis of data. Student must recognize the importance of every step and show that he is ready for medical data manipulation. First step is creation of data carrier that contains all data that must be analyzed. Second step is creation of database and final step is data analysis and descriptive analysis with statistical analysis. These steps are performed according to written instruction. The student use data that are provided together with written instructions. The student must know how to prepare and manipulate with data to pass first part of exam.
The Theoretical part of examination is done using the multiple choice answer form provided by special software with randomly selected questions for each student. The final knowledge check of the students is also performed using the Data Base Management system Ms Access specifically designed to cover full teaching and training material by using question sets in the data base which encircled nearly 1500 question combinations. In such way, using the combinations of questions it is possible to give different set of questions to each student. At the beginning of test, each student fills up the information about his name and index number. The time of solving all questions is limited to one hour. After exam it is possible to se result immediately. The students prefer this method because it is much easier to them to solve the test and they no need to wait for results as it is case when we perform the classic multiple choice test. The usual number of questions to be solved is twenty. There are six different scores that can be obtained. The mark “five” means that student did not pass the exam. Other marks are marks from 6 to 10 meaning that ten is the best mark. At least eleven questions must be answered correctly to pass exam and get mark six. For the best mark students need to answer 19 or 20 questions correctly. The student use mouse pointer to check correct answers in check boxes beside answers (Figure 6)
6. ADVANTAGES AND DISADVANTAGES OF DISTANCE LEARNING
Distance learning compared to the traditional way of learning have many its advantages as well as disadvantages (8,17). some of the main advantages of distance learning are: the economical factor; a student has 24 hour access to needed information; he/she is given the opportunity to learn the subject in his/hers own time and speed; he/she can access learning materials independently of a place or time; he/she is given the opportunity to learn how to work independently; using e-mail or chat rooms he/she is able to contact a professor or his/hers assistant if there are any questions or confusions regarding lectures; etc. Many critics consider that using e-mail or chat rooms to obtain a contact with the professor is actually the main disadvantage of this system of learning. A question arises whether this way of the professor-student communication is helpful to students as the face-to-face contact is missing as well as the opportunity of student-professor relationship building. However, in many universities across Bosnia and Herzegovina student’s contact with a professor is almost impossible (unless one needs to take the exam orally), due to many professors having other jobs or responsibilities; students are mainly able to communicate with professor’s assistants. Moreover, through the traditional way of teaching, during the lectures, students obtain from their professors mostly the information, which they can find in the literature or on the Internet. Rarely, there is a student-professor interaction or lecture discussion during the class. From this one can conclude that an ambitious student using tele-education will experience minimum lose (8).
Distance learning compared to traditional way of learning had many its advantages as well as disadvantages. some of the main advantages of distance learning are: the economical factor; student has 24 hour access to needed information; he/she is given the opportunity to learn the subject in his/hers own time and speed; he/she can access learning material independently of place or time; he/she is given the opportunity to learn how to work independently; using e-mail or chat rooms he/she is able to contact professor or his/hers assistant if there are any questions or confusions regarding lectures; etc. (2,3).
Fundamental advantages of flexible education in terms of classical education are:
More efficiency;
Increase capacities of educational institutions;
Education can be easily adopted to the needs of education on-the-job;
Costs of educational process are smaller;
It is possible to distribute the education uniformly, thus the new educational programs are available for fields outside of educational and economic centres;
It enables the possibility of access to the foreign educational resources to the various institutions;
Superior quality of the knowledge gained.
Many critics consider that using e-mail or chat rooms to obtain contact with the professor is actually the main disadvantage of this system of learning. Question arises whether this way of professor-student communication is helpful to students because face-to-face contact is missing as well as the opportunity of student-professor relationship building. However, in many universities across Bosnia and Herzegovina students’ contact with professors are almost impossible (unless one needs to orally take the exam), due to many professors other jobs or responsibilities; students are mainly able to communicate with professor’s assistants. Moreover, thru traditional way of teaching, during the lectures, students from their professors obtain mostly the information which they can find in the literature or on the internet. Rarely, there is student-professor interaction or lecture discussion during the class. From this one can conclude that an ambitious student using tele-education will experience minimum lose.
We live in “Age of Information”. These technologies are changing the way we perceive the world, how wee think and communicate with another. Established cultures are being transformed and new cultures are forming. New virtual environment affects the way we build our sense of who we are. Some characteristics of the Internet with which are people in B&H know a little are:
Large volume of users and potential users,
Lack of physical boundaries which allows for the manipulation of time and space,
Information can be accessed in a concurrent fashion using different media,
Concept of redundancy.
In the virtual environment we are applying for information in a way that is expanding our senses and one must to take into account that experience is occurring in the context of the virtual environment. Information without a context has no meaning.
7. OUR EXPERIENCES IN APPLICATION OF E-LEARNING AT BIOMEDICAL UNIVERSITIES IN B&H
The greatest progress was made in the area of tele-education and distance learning in Bosnia and Herzegovina. Distance learning does not preclude traditional learning processes; frequently it is used in conjunction with in-person classroom or professional training procedures and practices. Distance learning is used for self-education, tests, services and for the examinations in medicine, i.e. in terms of self-education and individual examination services. The possibility to work in the exercise mode will image files and questions is an attractive way for self-education [1].
Very first serious initiative was generated by WUS Austria (World university service of Austria) in BiH. During 2002 and 2003 WUS Austria, through its programs, Distance learning 2002 and Distance learning 2003 year, supported the development of the educational processes at BiH universities. At Medical faculty of university of Sarajevo at Cathedra for Medical informatics since 2002 is in progress realization of the project named: “Possibilities of introducing of distance learning in medical curriculum”, approved by the Federal and the Cantonal ministry of science and education. The purpose of the project is to facilitate improvement of educational process at biomedical faculties, applying contemporary educational methods, methodologies and information technologies in accordance with strategy and goals proclaimed by Bologna declaration. Pilot project was realized during three past school years (2003-2005), theoretical and practical education of subject Medical informatics are adapted to the new concepts of education using world trends of education from the distance. One group of students was included in the project finalized by electronic exam registration and electronic exam on 20 June 2005, publicly, in the Physiology amphitheatre of the Medical faculty in Sarajevo (Figure 7).
Bologna process, which started last years in European countries, provides us to promote and introduce modern educational methods of education at biomedical faculties in Bosnia and Herzegovina. Cathedra of Medical informatics and Cathedra of Family medicine at Medical Faculty of University of Sarajevo started to use web based education as common way of teaching of medical students. Satisfaction with this method of education within the students is good, but not yet suitable for most of medical disciplines at biomedical faculties in Bosnia and Herzegovina. Web sites of Cathedra for Medical Informatics and Family Medicine and UTIC (University Tele-information Centre) are shown in the Figure 8.
FIGURE 8.

Web sites of Cathedra for Medical Informatics, UTIC and Cathedra for Family Medicine
Bosnian society for Medical Informatics (BHSMI) is very proactive in promoting telemedicine and teleeducation as part of it. The last event organized by BHSMI was special Topic Conference named e-health and e-Education held in December 2005 (Figure 9).
Distance learning in medicine has impact on telemedicine and practicing medicine as well. Basic skills of the use of computers and networks must be a part of all future medical curricula. The impact of technical equipment between patient and the doctor must be understood, and the situation where the diagnosis based on live voice or picture is different from a normal doctor-patient contact. In some areas telemedicine requires unique techniques. Tele-robotically discipline guaranties differ from what surgeons normally learn. Telemedicine, and distance learning as a prerequisite for it, is lest suited for doctor-to-doctor consultation, and the first contact to a doctor should always be a face-to-face consultation [15,16,17,18,19].
8. INTEGRATING E-LEARNING INTO MEDICAL EDUCATION
Integration of tele-education as an official standard of education is a decision which has to be made by faculty management. It is result of faculty’s a well designed plan according to current possibilities. Although some institutions have tried to use distance learning as a stand-alone solution to updating or expanding their curricula, it is best to begin with an blended strategy that considers the benefits and burdens of blended learning before revising the curriculum. In medical education content can be delivered either synchronously or asynchronously (18). Synchronous delivery refers to real-time, instructor-led e-learning, where all learners receive information simultaneously and communicate directly with other learners. With asynchronous delivery, the transmission and receipt of information do not occur simultaneously. The learners are responsible for pacing their own self- instruction and learning. The instructor and learners communicate using e-mail or feedback technologies, but not in real time. Synchronous content delivery is hard to achieve in medical education without some preconditions needed at biomedical faculties in Bosnia and Herzegovina: high speed Internet connections, free access to computers and computer skills of students and teachers. The Cathedra for Medical Informatics has shown that it is possible to introduce tele-education. It is upon the faculty management to recognize the need for introduction of new forms of education and also to reward faculty members for their effort in developing tele-education. For tele-education to be further developed and maintained it is highly recommendable to have a centers which can provide a wide range of services, including system deployment and administration, training of faculty and administrators, assistance in content development, supervision, maintenance, research, and consultation.
9. THE FUTURE OF E-LEARNING
Pilot project from Medical Informatics at Medical Faculty in Sarajevo has started and will work further in order to develop and integrate information and communication technologies in medical education. The project has created a tele-education infrastructure which will develop further giving access to tele-education to educators.
Developments in e-learning and technologies are creating the groundwork for a revolution in education. The Internet2 is a University-led project with the aim to develop extremely fast speed, complex real-time multimedia capabilities, and quality of service would provide educators enormous potential to develop tele-medicine (19). Larger bandwidth offers the promise of sophisticated immersive simulations and the use of full-motion video in real time, in both asynchronous and synchronous modes of instruction, delivered to any desktop computer (19). Many medical schools and health care organizations are already producing high-fidelity e-learning materials, such as virtual patient simulations, that could soon be within the reach of any educator and learner (20,21,22). Quantitative and qualitative studies of collaborative learning in medicine have shown higher levels of learner satisfaction, improvements in knowledge, self-awareness, understanding of concepts, achievement of course objectives, and changes in practice (23,24).
An evolving emphasis within medical education on lifelong learning and competency-based education has forced educators to reevaluate their traditional roles. In this changing paradigm, educators no longer serve as the sole distributors of content, but are becoming facilitators of learning and assessors of competency (25).
Distance learning or learning from the distance represents the educational technique which occupies significant place in the actual medical education of the health care professionals abroad, especially in postgraduate and continuous medical education. With two projects in this area Possibilities of introduction of Distance Learning in Medical Curriculum and Introduction and Implementation of Distance Learning in Medicine, the Cathedras for Medical Informatics, Medical faculty, University of Sarajevo and Tuzla have made tremendous progress in education of undergraduate students and medical professional in Bosnia and Herzegovina. Also, this paper gives recommendation for sustainable Distance Learning and really lifelong educational process.
Distance learning in medicine has impact on telemedicine and practicing medicine as well. Basic skills of the use of computers and networks must be a part of all future medical curricula. The impact of technical equipment between patient and the doctor must be understood, and the situation where the diagnosis based on live voice or picture is different from a normal doctor-patient contact. In some areas telemedicine requires unique techniques. Tele-robotical guaranties differ from what surgeons normally learn. Telemedicine, and distance learning as a prerequisite for it, is lest suited for doctor-to-doctor consultation, and the first contact to a doctor should always be a face-to-face consultation.
Expected outcomes of the project Introduction and Implementation of Distance learning in medicine are:
Development and integration of informatics-computer technologies in medical education
Creation of flexible infrastructure which will enable access to e-Learning by all students and teaching staff
Improvement of digital literacy of academic population
Ensure high educational standards to students and teaching staff and
To help medical staff to develop “Lifelong learning way of life”.
The health sector is one of the most evident potential beneficiaries of the Internet revolution and World Wide Web resource in the present and in the future, when the tools now available and the system’s reliability and efficacy as a whole will be further incremented and improved.
In order to have Distance Learning minimum of requirements should be in place: Minimal infrastructure: equipment and software, from laptop to notebook, projector and scanner to reliable and quality software, appropriate marketing in Bosnia and Herzegovina environment, education of the educators and administrators, Electronic archive (and digital library), support from the officials (moral and financial) and sustainable funding.
10. CONCLUSION
Distance learning in medicine is a project started by Prof. dr. Izet Masic and his team at Cathedra of Medical Informatics of Faculty of Medicine at University of Sarajevo in year 2002 as first pilot study of introduction of Distance learning education at biomedical faculties in Bosnia and Herzegovina for improving the educational system in our country. Distance learning is a trend used in many developed countries spreading fast throughout the rest of the world. We hope that this will be just a starting ground to our attempts of improvement of our education system. Web site of Cathedra of Medical Informatics of Faculty of Medicine at university of Sarajevo is www.unsamedinfo.org. This is for the first time in B&H that students are able to apply for exam, have exam and results on the web site as well as his/her picture and all other significant data.
REFERENCES
- 1.Masic I, Novo A, Kudumović M, Mašić Z. Edukacija iz Medicinske informatike na medicinskim fakultetima u BiH. AIM, 2005; 13(1): 3-8 [Google Scholar]
- 2.Masic I, Novo A, Kudumovic M, Masic Z. E-learning at Medical Faculty of University of Sarajevo. AIM; 2005; 13(3): 132-5 [Google Scholar]
- 3.Masic Z, Novo A, Masic I, Kudumovic M, Toromanovic S, Rama A, Dzananovic A, Bander I, Masic M, Guso E, Balta E. Distance Learning at Biomedical Faculties in Bosnia and Herzegovina. Stud Health Technol Inform, 2005: 267-72 [PubMed] [Google Scholar]
- 4.Engelbrecht R, Ingenerf J, Reiner J. Educational standards - terminologies used. Stud Health Technol Inform. 2004; 109: 95-113 [PubMed] [Google Scholar]
- 5.Hovenga J. Bricknell L. Current and Future Trends in Teaching and Learning. Stud Health Technol Inform. 2004; 109: 131-142 [PubMed] [Google Scholar]
- 6.Mantas J. Comparative educational systems. Stud Health Technol Inform. 2004; 109:8-17 [PubMed] [Google Scholar]
- 7.Sosa-Iudicissa M, Oliveri N, Gamboa CA, Roberts J. Internet, Telematics and health. IOS Press, 1997; 36: 5-53 [Google Scholar]
- 8.Glinkowski W. et al. Advances in International Telemedicine and ehealth. Vol. 1 – Around the world. MedPage Ltd, Warsaw, 2006; 28-36 [Google Scholar]
- 9.Masic I. Quality Assessment of Medical Education - why Bologna? Mat Soc Med, 2007; 19(2): 122-4 [Google Scholar]
- 10.Masic I. Five years on from the introduction of the method of “Distance learning” in medical curriculullm in B&H. Med-e Tel, Louxembourg, 18-20 April, 2007, Proceedings: 97-8 [Google Scholar]
- 11.Mašić I. Virtuelno učenje - za i protiv. AIM, 2000; 8(1-2): 3-4 [Google Scholar]
- 12.Pašić E, Mašić I. Računarske mreže i komunikacije računara. AIM, 2000; 8(3-4): 101-6 [Google Scholar]
- 13.Mašić I. Edukacija iz medicinske informatike i njene perspektive. AIM, 2001; 9(3-4): 59-60 [Google Scholar]
- 14.Ahmetović A, Mašić I, Jakupović S, Mašić Z.Zaštita podataka na Internetu. AIM, 2001;9(3-4):97-100 [Google Scholar]
- 15.Mašić I, Ademović A, Jakupović S, Mašić Z, Žunić L. Internet mreža i njena sigurnost. Med Arh, 2002; 56(1): 51-5 [PubMed] [Google Scholar]
- 16.Ramić-Čatak A, Mašić I. Distance learning – učenje sa distance u medicinskoj edukaciji. AIM, 2002; 10(2): 63-6 [Google Scholar]
- 17.Mašić I, Kudumović M. Učenje na daljinu u medicinskom obrazovanju. AIM, 2002; 10(3-4): 129-32 [Google Scholar]
- 18.Omerhodžić I, Banjanović B, Mašić I. Mogućnosti uvođenja i primjene učenja na daljinu na Medicinskom fakultetu u Sarajevu. AIM, 2002; 10(3-4): 149-52 [Google Scholar]
- 19.Pašić E, Mašić I. Teleispit na Medicinskom fakultetu Univerziteta u Sarajevu. AIM, 2002; 10(3-4): 157-8 [Google Scholar]
- 20.Mašić I, Pašić E, Pandža H, Kudumović M. Edukacija iz Medicinske informatike na Medicinskom fakultetu u Sarajevu. AIM, 2002; 10(3-4): 159-64 [PubMed] [Google Scholar]
- 21.Mašić I. Edukacija iz informatike i medicinske informatike. AIM, 2003; 11(1-2): 5-16 [Google Scholar]
- 22.Mašić I, Hadžiahmetović Z, Toromanović S, Kudumović M. Telemedicina, virtuelna realnost, teleoperacije – hirurški aspekti. Med Arh, 2003; 57(3, supl. 1): 48-9 [Google Scholar]
- 23.Kudumović M, Mašić I, Novo A, Mašić Z, Omerhodžić I. Učenje na daljinu u medicinskoj edukaciji. Med Arh, 2004; 58(1, supl. 2): 95-7 [PubMed] [Google Scholar]
- 24.Novo A, Masic I, Kudumovic M, Masic Z. Teleeducation at biomedical faculties in B&H. AIM, 2004; 12(3-4): 67-70 [Google Scholar]
- 25.Husić-Selimović A, Mašić I. Teleedukacija u porodičnoj medicini. AIM, 2004; 12(3-4): 87-9 [Google Scholar]
- 26.Masic I, Novo A, Kudumovic M, Masic Z. Teleeducation in B&H. health and Medical Informatics Applications. Proceedings of the EFMI special Topic Conference Athens, 19.-20. March 2005: 121-3 [Google Scholar]
- 27.Masic I, Novo A, Kudumovic M, Masic Z. E-learning at Medical Faculty of University of Sarajevo. AIM, 2005; 13(3): 132-5 [Google Scholar]
- 28.Masic I, Novo A. Medical Informatics Education in Bosnia and Herzegovina. AIM, 2005; 13(4): 184-8 [PubMed] [Google Scholar]
- 29.Mašić I, Kudumović M, Novo A, Rama A, Mašić Z, Bander I, Bašić M, Gušo E, Balta E. Mogućnosti uvođenja učenja na daljinu u medicinski curriculum. Med Arh, 2005; 59(4): 269-70 [PubMed] [Google Scholar]
- 30.Masic I, Kudumovic M, Novo A, Rama A, Masic Z, Dzananovic A. Distance Learning at the Medical University of Sarajevo. European Journal for Biomedical Informatics (EJBI), 2005; 1(1): 11-6 [Google Scholar]
- 31.Masic I, Novo A, Kudumovic M, Rama A, Masic Z, Dzananovic A, skrbo A. E-learning at Medical faculty of University of Sarajevo. Medicinska Informatika, 2005; 7: 29-35 [Google Scholar]
- 32.Masic Z, Novo A, Masic I, Kudumovic M, Dzananovic A, Toromanovic S. E-learning as modern method of medical education. second Congress of Medical Informatics of Turkey. Antalia, Turkey, 17-19-2005. Proceedings: 33-8 [Google Scholar]
- 33.Masic I, Kudumovic M, Novo A, Masic Z, Guso E, Basic M. Learning from distance in Bosnia and Herzegovina. AIM, 2005; (4,suppl1): 21-5 [Google Scholar]
- 34.Masic I, Novo A, Masic Z. Web based medical informatics education. In: Integrating Biomedical Information: “from e-CELL to e-PACIENT”. Timisoara 6-8 april 2006: 260-2 [Google Scholar]
- 35.Masic I, Novo A, Kudumovic M, Rama A, Dzananovic A, Guso E, Basic M. Web Based Distance Learning at Faculty of Medicine of Sarajevo University. Bosnian Journal of Basic Medical sciences, May 2006; year VI, number 2: 71-5 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Masic I, Novo A, Deljkovic S, Toromanovic S. Contemporary education of medical students by use of information technologies. Mat Soc Med, 2006; 18(2): 69-72 [Google Scholar]
- 37.Masic I, Novo A. Telemedicine in Bosnia and Herzegovina. AIM, 2006; 14(2): 103-5 [Google Scholar]
- 38.Mašić I, Novo A, Kudumović M, Mašić Z. Medicinska informatika na medicinskim fakultetima u Bosni i hercegovini. Acta Med Croatica, 2006; 60(5): 463-9 [PubMed] [Google Scholar]
- 39.Valjevac A, Masic I, Nakas-Icindic E, Kudumovic M. Perspective of teleeducation development in biomedicine in Bosnia and Herzegovina. AIM, 2007; 15(1): 31-5 [Google Scholar]
- 40.Masic I, Jamakovic M, Cimic A. Information technologies in medical education. AIM; 2007; 15(2): 88-94 [Google Scholar]