

Abstract
CONFLICT OF INTEREST: NONE DECLARED
Evidence based medicine (EBM) is the conscientious, explicit, judicious and reasonable use of modern, best evidence in making decisions about the care of individual patients. EBM integrates clinical experience and patient values with the best available research information. It is a movement which aims to increase the use of high quality clinical research in clinical decision making. EBM requires new skills of the clinician, including efficient literature-searching, and the application of formal rules of evidence in evaluating the clinical literature. The practice of evidence-based medicine is a process of lifelong, self-directed, problem-based learning in which caring for one’s own patients creates the need for clinically important information about diagnosis, prognosis, therapy and other clinical and health care issues. It is not “cookbook” with recipes, but its good application brings cost-effective and better health care. The key difference between evidence-based medicine and traditional medicine is not that EBM considers the evidence while the latter does not. Both take evidence into account; however, EBM demands better evidence than has traditionally been used. One of the greatest achievements of evidence-based medicine has been the development of systematic reviews and meta-analyses, methods by which researchers identify multiple studies on a topic, separate the best ones and then critically analyze them to come up with a summary of the best available evidence. The EBM-oriented clinicians of tomorrow have three tasks: a) to use evidence summaries in clinical practice; b) to help develop and update selected systematic reviews or evidence-based guidelines in their area of expertise; and c) to enrol patients in studies of treatment, diagnosis and prognosis on which medical practice is based.
Key words: Evidence Based Medicine, health, patients, decision making
1. INTRODUCTION
During the last decade, concept of Evidence Based Medicine (EBM) caused great interest among health professionals. According to definition Evidence Based Medicine represents integration of clinical expertise, patient’s values and best available evidence in process of decision making related to patients health care. Medical knowledge grows every day, so that previously accepted facts rapidly become old and it seems impossible to follow such explosion of scientific information. There are clear difficulties when clinician needs to keep step with the new achievements published in medical journals: for example, general practitioner should read 19 articles every day (1), and we know that many of them have only one hour per week for this. The problem of academic isolation or armchair phenomenon occurs, where the doctor should spend most of its work hours only to review all published articles and studies. On the other side, even if the doctors find the time to read all of them, they would be lack the time to evaluate the value of the study, its methodology, outcome and transparency. That is why a need occurs that the doctor, with his limited time, read selectively, make effective selection of what he reads, and what not (1). Family medicine, by its nature, is very complicated discipline which is featured among other things, high proportion of poorly differentiated problems overlapping with the biological, psychological and social factors. EBM - Evidence Based Medicine, which originated in the second half of the 19th Century and earlier, means conscious and reasonable use of current, best scientific evidences in making decisions in treatment of each individual patient. Evidence based medicine is the conscientious, explicit, judicious and reasonable use of current best evidence in making decisions about the care of individual patients.
EBM application means relating individual clinical signs, individual clinical experience with the best scientific evidences obtained by the clinical research (2). The revised and improved definition of evidence-based medicine is a systematic approach to clinical problem solving which allows the integration of the best available research evidence with clinical expertise and patient values. Under the individual clinical noticing we thought of the ability, skill that doctors acquired during years of clinical practice, and clinical experience is necessary and indispensable part that makes a good doctor. The best scientific evidence is considered to be a randomized controlled clinical study conducted on the amount of respondents that can prove the effectiveness of many drugs, as well as the harm and the inefficacy of others in comparison with the best existing therapy (3). The practice of evidencebased medicine is a process of lifelong, self-directed, problem-based learning in which caring for one’s own patients creates the need for clinically important information about diagnosis, prognosis, therapy and other clinical and health care issues.
Instead of routinely reviewing the contents of dozens of journals for interesting articles, EBM suggests that you target your reading to issues related to specific patient problems. Developing clinical questions and then searching current databases may be a more productive way of keeping current with the literature. Evidence-based medicine “converts the abstract exercise of reading and appraising the literature into the pragmatic process of using the literature to benefit individual patients while simultaneously expanding the clinician’s knowledge base.”
Evidence based medicine is not “cookbook” medicine. Because it requires a bottom up approach that integrates the best external evidence with individual clinical expertise and patients’ choice, it cannot result in slavish, cookbook approaches to individual patient care. External clinical evidence can inform, but can never replace, individual clinical expertise, and it is this expertise that decides whether the external evidence applies to the individual patient at all and, if so, how it should be integrated into a clinical decision. Similarly, any external guideline must be integrated with individual clinical expertise in deciding whether and how it matches the patient’s clinical state, predicament, and preferences, and thus whether it should be applied. Clinicians who fear top down cookbooks will find the advocates of evidence based medicine joining them at the barricades.
2. NEED FOR EVIDENCE BASED APPROACH IN MAKING DECISIONS IN FAMILY MEDICINE
Core of Family medicine in relation doctor-patient. One of the central aspects of this relationship is the decision-making process, which can vary from simple types of clinical decisions (e.g., the patient has a sore throat, larynx was red, but without suppuration - whether it should prescribe antibiotic?) or (patient complains about frontal headache for two weeks, she was present when a patient walked - do you need to perform CT of the head?), etc. (4)
3. 3. DIFFERENCE BETWEEN EVIDENCE BASED MEDICINE AND EVIDENCE BASED HEALTH CARE
It is useful to make a difference between these two terms. Evidence Based Medicine is a conceptual approach of the physician in making decisions related to the individual patient. Unlike this, Evidence Based health Care is somewhat broader concept that includes advanced approach to understanding the patients, families and doctors beliefs, values and attitudes. Evidence Based Health Care, also relies on evidence, but primarily those on population level (5).
4. GAP BETWEEN RESEARCH AND PRACTICE
One of the main reasons why there is such a great interest in approach to Evidence Based Medicine is the growing number of examples, in which current medical practice cannot cape pace with the available clinical evidences. So, for example, despite the strong evidences during seventies of the last century that the treatment such as thrombolytic therapy and use of aspirin are efficient in treatment of acute myocardial infarction, it took almost one decade that these treatments become routine in treatment procedures for the patients with acute myocardial infarction. Similar to this, there are examples that some-where were available scientific research (evidences) and their practical application is complex. On one side, there is a lack of firmness which will synthesize and make systematic results of the primary scientific researches. On the other side, that indicates inability of available evidences obtained in research which will gain relevant information which consumers of health services and medical professional needs to make decisions. In broader sense, that reflects lack of appropriate frames, systems and strategies which will more efficiently influence of professional conduct.
5. COMPLEXITY OF THE PRIMARY HEALTH CARE (FAMILY MEDICINE)
It is known that the patients come to the family doctor with poorly defined symptoms and large clinical variations – the number of such patients is for sure largest in family practice. They are so called symptoms of illness in the “grey zone”, usually multiple complains of the patients on different organic systems. Rarely that is a single problem. The fact is that only small number of cases can be solved during the first meeting doctor-patient. Family doctor often is forced to make plan of care for the patients, because it is a case of complex issues, and it is difficult to make care plan. Complex nature of work in general practice means that the patient seeks assistance in aspect of illness (feeling ill) for which it does not have strong proofs about efficiency of any intervention. Report by Gill and colleagues (6) is based on retrospective analysis of series of doctor-patients meetings has shown that in high percent (81%) intervention in general practice can be supported by the evidences from the randomized controlled studies and (or) convincing non experimental evidences. There is still need to refine in which manner should be incorporated in the complexity of doctor-patient relation within Family medicine. One of the important concepts of EBM is the hierarchy in validating evidences based on which decision is made, which means that before making decisions it is important to evaluate value of evidences. According to that concept most valuable evidence, for example efficacy of the single therapeutic mean, comes from the results of the multicenter, randomized, comparison, controlled clinical study. Evidences of least value are based on studies of the physiology functions and clinicians observations.
6. CLASSIFICATION OF EVIDENCE – INFORMATION LEVELS
Evidence-based medicine categorizes different types of clinical evidence and ranks them according to the strength of their freedom from the various biases that beset medical research.
-
1.
Evidences obtained by meta-analysis of several randomized controlled research (RCR).
-
1b.
Evidences from only one RCR.
-
2a.
Evidences from well designed controlled research RCR.
-
2b.
Evidences from one quasi experimental research.
-
3.
Evidences from non experimental studies (comparative research, case study), according to some, for example Textbooks.
-
4.
Evidences from experts and clinical practice.
The principle of EBM emphasizes, above all, that the foundation of any medical decisions regarding the optimal diagnostic or therapy procedure are scientific evidences from clinical research, and clinical experience and intuition are of great help, but not the main basis in decision-making. New in the application of EBM is that making decisions about treatment for each individual patient is a complex process that allows doctors and patients to select the best possible solutions for each individual patient. As the EBM includes the routine use of the best scientific evidences obtained by clinical research, they are actually impossible before electronic databases in the early 90’s occurred (5,6).
While some find traces of evidence-based medicine’s origin in ancient Greece, (1,2) others trace its roots to ancient Chinese medicine. (3,4) Although testing medical interventions for efficacy has existed since the time of Avicenna’s The Canon of Medicine in the 11th century, (5,6) it was only in the 20th century that this effort evolved to impact almost all fields of health care and policy. Professor Archie Cochrane, a Scottish epidemiologist, through his book Effectiveness and Efficiency: Random Reflections on Health Services (1972) and subsequent advocacy, caused increasing acceptance of the concepts behind evidence-based practice. Cochrane’s work was honoured through the naming of centres of evidence-based medical research — Cochrane Centres — and an international organization, the Cochrane Collaboration. The explicit methodologies used to determine “best evidence” were largely established by the McMaster University research group led by David Sackett and Gordon Guyatt. The term “evidence based” was first used in 1990 by David Eddy. (7,8) The term “evidence-based medicine” first appeared in the medical literature in 1992 in a paper by Guyatt et al. (9).
The idea of EBM appeared at the Mc Master University in Canada in 1988, but during the 1990s became known throughout the world. However, the founder of EBM is considered to be English epidemiologist Archie Cochrane, who lived in the 19th century and which has already pointed out the impossibility of monitoring all the new discoveries in medical science. During the last ten years in the world rapidly is growing the interest in the application of EBM. The reason for this is the application of electronic records, the Internet phenomenon, an increasing number of different clinical tests that doctors cannot track, as well as increase in cost of health care (7).
Today, in almost all western countries doctors apply EBM in treatment for every patient with the support of the governments of these countries, the ministries of health and pharmaceutical
industry. This includes practical guidelines for different diseases, a database with the best scientific evidence from each category, which is edited by special experts and which is continuously updated with new data, medical journals and literature available with the latest objective information. (8)
In recent years EBM has become especially useful in answering questions on which there is no intuitive answers or for which our clinical observations can cause more harm than good. It is a long list of procedures that appeared useful at one moment, and afterwards shown to be inefficient or even harmful. Example of this is the application of thalidomide during pregnancy and as consequence of that children was born with anomalies.
7. HOW TO START: 5 STEPS PROCESS FOR USE OF EVIDENCE ORIENTED APPROACH IN FAMILY MEDICINE
How will family medicine doctors start, if they want to apply evidence based approach in their daily practice? Group for Evidence Based Medicine Resource from McMaster University identified the approach in 5 steps that each individual physician in the application of this approach must follow.
problem definition,
search for wanted sources of information,
critical evaluation of the information,
application of information of the patient,
efficacy evaluation of this application on a patient.
7.1. Step 1. Defining problem
Each doctor several times a day is in the position of making various medical decisions. Often in the process of medical decision-making occur questions such as: for and against the use of certain therapies, whether to use a diagnostic test or screening procedure, the risk or prognosis of a particular disease or cost-effectiveness of specific interventions. It is clear that the already busy doctor, will not be able to answer in this way all the questions that come in practice and therefore must resort to the process of determining priorities, as well as refining issues that needs to be asked.
A clinician starts his or her search for the best and newest data needed to solve individual patient’s problem by formulating an answerable clinical question. Good clinical question must be clear, directly focused on the problem, and answerable by searching the medical literature.
-
PICO format
A good clinical question should have four essential components structured in the PICO format (Patient or problem, Intervention, Comparison, Outcome).
PICO format:
the patient or problem – who are the relevant patients, what kind of problem we try to solve?
the intervention – what is the management strategy, diagnostic test or exposure (drugs, diagnostic test, foods or surgical procedure)?
comparison of interventions – what is the control or alternative management strategy, test or exposure that we will compare?
the outcome – what are the patient-relevant consequences of the exposure in which we are interested?
-
Type of clinical question
The most common type of clinical question is about how to treat a disease or condition. Such questions are questions about intervention.
Types of clinical questions:
questions about intervention
questions about etiology and risk factors
questions about frequency and rate
questions about diagnosis
questions about prognosis and prediction
question about cost-effectiveness
question about phenomena
7.2. Step 2. Search for wanted sources of information
After formulating the clinical question, which stems from a concrete patient, the next step is to search for relevant evidence that will provide the answer to the question.
This is not always easy, especially in Family medicine, in which the problems caries the poorlydefined problems in the start. However, there are numerous sources of information that may be of assistance, including medical journals, which treat certain problems in the field of Family medicine, search of electronic databases and communication with colleagues.
The ideal information source is valid (contains high quality data), relevant (clinically applicable), comprehensive (has data on all benefits and harms of all possible interventions), and is user-friendly (is quick and easy to access and use).
7.3. Step 3. Critical evaluation of the information
When we decide which magazine to read, it is important to read it carefully, because not all the published information is of equal importance and value. Critical assessment of the articles is a process that involves careful reading and analysis of methodology, contents and conclusions. A key question that should be kept in mind is “Do I believe in the results enough that I’ll be ready to a similar approach, or in achievement of similar results with my patients?” Skills to obtain the ability of critical evaluation should be learned and practiced as any other clinical skills.
7.4. Step 4. Application of information of the patient
The fourth step in the process of the use of Evidence Based Medicine in practice is the decision how to apply acquired information on the special circumstances pertaining to each patient. This is probably a crucial step in the process, if not the most complex. Now it is necessary to decide whether there is something in relation to our patient because of which it would be necessary to discard the acquired information.
The questions that we should ask before the decision to apply the results of the study are:
Are the participants in the study similar enough to my patient?
Is the treatment available and is health care system prepared to fund it?
What alternatives are available?
Do the potential side effects of the drug or procedure outweigh the benefits?
Are the outcomes appropriate to the patient? Does the treatment conflict with the patient’s values and expectations?
If something does not exist, it is necessary to weigh the potential harm from the benefit and do all that in partnership with the patient, where our decision in the end, in fact, will be shared.
7.5. Step 5. Efficacy evaluation of EBM application on a patient
The final step is the evaluation of Evidence - based approach and efficiency of its application to a specific patient. During this process it is important to assess whether certain evidence, which is applied to the patient, caused changes to better and that to the extent that it is confirmed by research. If the data differ significantly, it would be necessary to investigate why some patients did not respond to the changes introduced in the expected way and what can be done to change it.
The EBM-oriented clinicians of tomorrow have three tasks:
To use evidence summaries in clinical practice;
To help develop and update selected systematic reviews or evidence-based guidelines in their area of expertise; and
To enrol patients in studies of treatment, diagnosis and prognosis on which medical practice is based.
COHRANE COLLABORATION AND COHRANE LIBRARY
Important sources of evidence include online electronic resources. Physicians should use websites and texts that are revised at least once a year, select and appraise evidence in explicit way, and cite evidence in support of statements about clinical care.
Sources of evidence
There are different web sources of evidence. The search for best evidence should begin by looking at the highest-level source available for the problem in question. Evidence-based journals of secondary publication select from the biomedical literature original and review articles, summarize them, and present comments by clinical experts (1).
There are several online evidence-based databases. The Cochrane Library (available on a CD ROM or via the Internet site or via Ovid’s service) is the best source of reliable evidence about the effect of health care.
The Cochrane Library is a collection of databases in medicine and other healthcare specialties provided by the Cochrane Collaboration and other organisations. The Cochrane Collaboration is an international not-for-profit and independent organization, dedicated to making up-to-date, accurate information about the effects of healthcare readily available worldwide. It produces and disseminates systematic reviews of healthcare interventions and promotes the search for evidence in the form of clinical trials and other studies of interventions. The Cochrane Collaboration was founded in 1993 and named after the British epidemiologist, Archie Cochrane.
The major product of the Collaboration is the Cochrane Database of Systematic Reviews which is published quarterly as part of The Cochrane Library (2).
At its core is the collection of Cochrane Reviews, a database of systematic reviews and meta-analyses which summarise and interpret the results of highquality medical research. The Cochrane Library aims to make the results of well-conducted controlled trials readily available and is a key resource in evidence-based medicine.
It consists of a regularly updated collection of evidence-based medicine databases:
The Cochrane Database of Systematic Reviews (Cochrane Reviews)
The Database of Abstracts of Reviews of Effects (DARE)
The Cochrane Central Register of Controlled Trials (CENTRAL)
The Cochrane Database of Methodology Reviews (Methodology Reviews)
The Cochrane Methodology Register (Methodology Register)
Health Technology Assessment Database (HTA)
NHS Economic Evaluation Database (NHS EED) (2).
Clinical Evidence is an updated database of the best evidence for effective health care, put together by the BMJ. It summarizes the best available evidence and focuses on the effects of preventive and therapeutic interventions as demonstrated by randomized controlled trials (RTC) and systematic reviews.
Centre for Reviews and Dissemination Databases (CRD database) provides DARE and
NHS EED database, which contains over 6,000 abstracts of quality assessed economic evaluation, aims to assist decision-makers by systematically identifying and describing economic evaluations, appraising their quality, and highlighting their relative strengths and weaknesses (1).
Evidence-based databases:
The Cochrane Library (through the Cochrane Collaboration, http://www.cochrane.org)
The Cochrane database of systematic reviews: a collection of full text systematic reviews of the effects of health care, presents the best evidence, abstracts of reviews are freely available; http://www.cochrane.org/reviews/index.htm
The DARE: includes systematic reviews that have been published outside of the Cochrane collaboration, all quality-assesses and with structured summaries, freely available on the Web outside the Cochrane library through Centre for reviews and dissemination databases; http://www.crd.york.ac.uk/crdweb
The Cochrane Controlled Trials Register (CENTRAL): a bibliography of some 200,000 controlled trials, not freely available
Clinical Evidence; http://www.clinicalevidence.com; not freely available
CRD database; http://www.crd.york.ac.uk/crdweb: freely available (1).
Good doctors apply their clinical observation and experience, together with the best scientific evidence from medical literature. Without monitoring of new medical achievements treatment may become outdated, and, sometimes, on harm of patients. EBM reduces the value of intuition, non-systematic clinical experience and pathophysiology as sufficient basis in making clinical decisions, and emphasizes the value of evidence obtained by clinical research. Today, patients and other health care users themselves search the Internet and find information that often does not correspond to scientific knowledge, so the estimate of the validity of evidence and new knowledge should be left to doctors. (9). In England, in Oxford local health institutions are regularly use EBM system in negotiations with the doctors, the patients, the pharmaceutical industry and government on the application of new very expensive method of treatment which sometimes have uncertain outcomes (10).
EBM requires new knowledge from physicians, primarily access to medical databases, the ability to search medical literature and basic skills in the interpretation of epidemiological and statistical results. This should be used, not only by doctors but also nurses, patients themselves and health institutions. In our country the importance of EBM becomes every day more and more acknowledged. Each doctor should use more in treating their patients scientific evidence, and not only, which is often the case, his clinical experience and intuition.
8. ASKING QUESTIONS
During the last months I had in my practice 120 adolescents. Which preventive action should I take in case of these patients? Question can be put differently: What are effective preventive activities in adolescents?
9. SEARCHING ON PUBMED
Search criteria: adolescent prevention (Limits: no limit). Result: 11095 articles
Who can read all this?
Search criteria: adolescent prevention family medicine (no limits). Result: 167 articles
Can someone read this? In what time?
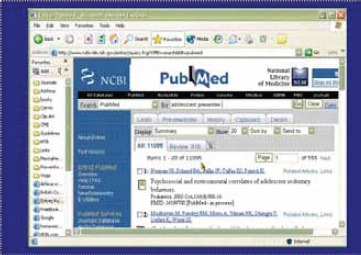
9.1. Search on PubMed
Search criteria: adolescent prevention family medicine (Limits) Meta-Analysis 0 articles
9.2. Search on PubMed
Search criteria: adolescent prevention family medicine (Limits) RCR. Result: 13 articles
From read summaries – clinical guideline for preventive activities among children and adults.
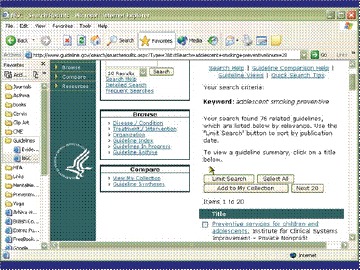
9.3. Search on PubMed
Search of adolescent prevention on www.guideline.gov. Result: 20 guidelines
9.4. Results
Institute for Clinical Systems Improvement (ICSI). Preventive services for children and adolescents. Bloomington (MN): Institute for Clinical Systems Improvement (ICSI); 2004 Sep. 33 p. [24 references]
10. MAIN GUIDELINES
Incorporate need assessment for preventive activities and counseling and education in acute visit if it is possible.
Estimate patient’s risk factors during visits and provide counseling and education for identified risks. All clinical visits, whether acute or chronic, are opportunity for preventive counseling and planned care for pediatric patients.
There are specific intervals when a healthy child should visit a doctor. For adolescents – twice in age between 13 and 18 years.
10.1. Specific guidelines for adolescents - screenings
Risk estimation
Interval anamnesis
Estimation of physical and mental development
Physical examination
Blood pressure
Papa test (starts with age of 18 or since beginning of sexual activity within maximal intervals of 3 years)
10.2. Specific guidelines for adolescents - additional screening for those under high risk
Tuberculosis test
Lipid levels
Examination of testicles
Testing on sexually transmitted diseases
10.3. Specific guidelines for adolescents – counseling and education
Good evidences to be included in practice:
Limited intake of saturated fats
Supplement with folic acid
Stop smoking
Problem alcohol drinking
10.4. Specific guidelines for adolescents – counseling and education
Fairly evidences to be included in practice:
Caloric and nutritional balance in nutrition
Physical activity
Drinking and driving
Use of seat belts
Prevention of unwanted pregnancy
Protection from the ultraviolet (UV) radiation
Dental and periodontal diseases
11. PRACTICAL APPLICATION
Incorporate in each visit preventive activities.
Conduct screening and additional screenings for those under increased risk.
Involve counseling and education for which exist good or fair evidences.
12. CONCLUSION
Evidence based medicine (EBM) is conscious, specific, reasonable use of modern, best evidences in making decisions about treatment of individual patients. It is not a medical cook-book with recipes, but its good application brings cost-effective and better health care. Its real purpose is that by the use of the best possible evidence doctor chooses for his patient the best possible solution, wanting to provide to him the optimum health care in every aspect. It is also used to avoid major mistakes in the course of treatment, and by this raises the quality of provided health care to the patient. In a wider context, it can save the lives of our patients. EBM requires new knowledge from the physician, which means knowledge of English language and work on the computer, which provides access to medical databases, the ability to search medical literature and basic skills in the interpretation of epidemiological and statistical results. Once the physician masters the search technique and the use of EBM he/she gets mighty “ally “in their daily noble work. Since each physician must, in one way or another, seek valid information, we can say that the proper use of EBM saves doctors time and raises his level as well as the quality of provided medical services, and increases satisfaction of the health professionals.
FIGURE 1.

Evidence based medicine triad
FIGURE 2.

Types of research
REFERENCES
- 1.Mašić I. Medicina bazirana na dokazima. U: Porodična/ Obiteljska Medicina principi i praksa, Avicena Sarajevo, 2007: 115-23 [Google Scholar]
- 2.Sackett DL, Richardson WS, Rosenberg W, Haynes RB. Evidence-based medicine: how to practice and teach. 2. ed. Edinburgh: Churchill-Livingstone, 2000 [Google Scholar]
- 3.Sackett DL, Rosenberg W, Mc Gray JA, Haynes RB, Richardson WS. Evidence-based medicine: what it is and what it isn’t. BMJ, 1996; 312: 71-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ridsdale L. Evidence-Based Practice in Primary Care. Churchill Livingstone, Edinburgh, London, New York, Sydney, Toronto, 1999: 9-30 [Google Scholar]
- 5.A report of the working party on medical education London: British Medical Association, 1995 [Google Scholar]
- 6.Evidence-based medicine and its place (editorial). Lancet, 1995; 346: 785. [PubMed] [Google Scholar]
- 7.Evidence-based medicine working group. Evidence based medicine. A new approach to teaching the practice of medicine. JAMA, 1992; 268: 2420-5 [DOI] [PubMed] [Google Scholar]
- 8.Silverman WA: Where is the evidence? Debates in modern medicine. Oxford: Oxford University Press; 1998 [Google Scholar]
- 9.Clinical Evidence Issue 6, December 2001, London, UK: BMJ Publishing Group, 2001 [Google Scholar]
- 10.Gill P, Dowell AC, Neal RD, Smith N, Heywood P, Wilson AR. Evidence based general practice: a retrospective study of interventions in one training practice. BMJ, 1996; 312: 819-21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Bordley DR, Fagan M, Theige D. Evidence-based medicine: a powerful educational tool for clerkship education. Am J Med, 1997. May; 102(5): 427-32 [DOI] [PubMed] [Google Scholar]
- 12.Geyman PJ, Deyo RA, Ramsey SC. Evidence-Based Clinical Practice: Concepts and Approaches. Global Releaf. Butter-worth-Henemann; Woburn, 2000: 13-40 [Google Scholar]
- 13.Brater DC, Daly WJ.Clinical pharmacology in the Middle Ages: Principles that presage the 21st century, Clinical Pharmacology & Therapeutics, 2000; 67 (5): 447-50 [DOI] [PubMed] [Google Scholar]
- 15.Daly WJ, Brater DC. Medieval contributions to the search for truth in clinical medicine, Perspectives in Biology and Medicine, Johns Hopkins University Press, 2000; 43 (4): 530–40 [DOI] [PubMed] [Google Scholar]
- 16.Eddy DM. Practice policies: where do they come from?. JAMA, 1990; 263 (9): 1265-9 [DOI] [PubMed] [Google Scholar]
- 17.Eddy DM. Evidence-based medicine: a unified approach. Health affairs (Project Hope), 2005; 24 (1): 9-17 [DOI] [PubMed] [Google Scholar]
- 18.Guyatt G, Cairns J, Churchill D, et al. ‘Evidence-Based Medicine Working Group’, Evidence-based medicine. A new approach to teaching the practice of medicine. JAMA, 1992; 268: 2420-5 [DOI] [PubMed] [Google Scholar]
- 19.Huić M. Evidence-based medicine. In: Marušić M. editor. Principles of Research in Medicine. Zagreb: Medicinska naklada; 2007: In press. [Google Scholar]
- 20.Craig JC, Irwig LM, Stockler MR. Evidence-based medicine: useful tools for decision making. MJA, 2001; 174: 248-53 [DOI] [PubMed] [Google Scholar]
- 21.Mašić I, Toromanović S, Smajkić A. Socijalna medicina sa osnovama zdravstvene njege u zajednici i polivalentnoj patronaži. AVICENA. Sarajevo, 2008: 279-92 [Google Scholar]
- 22. http://www.cochrane.org [Google Scholar]