

Abstract
Purpose
This study evaluated the efficacy of neoadjuvant chemotherapy combining 5-flurouracil/folinic acid with irinotecan (FOLFIRI) in colorectal multiple liver metastases regardless of resectability.
Methods
Forty-four patients with multiple (at least two) colorectal liver metastases were enrolled at seven tertiary referral hospitals between May 2007 and September 2010. All patients received the FOLFIRI chemotherapeutic regimen. Response to chemotherapy was assessed after three cycles (6 weeks) and once more after six cycles (12 weeks) of treatment.
Results
Objective response was noted in 27 patients (61.4%) and 4 patients (9.1%) had progressive disease. Of 44 patients, 10 patients (22.7%) underwent curative surgery (R0 resection) and 34 patients did not receive R0 resection. Grades 3 to 4 hematological toxicity was noted in 12 patients (27.3%) and grades 3 to 4 nonhematologic toxicity was identified in 5 patients (11.4%).
Conclusion
FOLFIRI chemotherapy as a neoadjuvant chemotherapy for multiple colorectal liver metastases regardless of resectability demonstrated the possibility of R0 resection, high rate of objective response, and tolerable toxicities in this study.
Keywords: Colorectal cancer, Neoadjuvant therapy, Metastasis, Chemotherapy
INTRODUCTION
Colorectal cancer (CRC) is one of the most common cancers occurring worldwide and the second leading cause of cancer-related deaths in Europe and the United States [1,2]. Approximately 50% of CRC patients will experience metastases [3], and patients with stage IV disease were deemed incurable, previously. However, if patients with colorectal liver metastases treated with extirpative surgery and proper chemotherapy, 5-year survival rates would reach up to 58% in the recent reports [4-6]. But, this survival benefit is limited among patients with liver metastases since only 10% to 20% of these patients are candidates for liver resection [4]. There are several reasons for unresectable liver metastases, including large size of metastasis, multiple bilateral lesions, and close proximity of major vessels (the hepatic veins, the inferior vena cava or the liver hilum). This indicates that 80% to 90% of patients with liver metastases received palliative or neoadjuvant chemotherapy.
Commonly available chemotherapy for liver metastases consists of 5-flurouracil (5-FU) with leucovorin (LV), irinotecan or oxaliplatin. Significant response rates of up to 56% have been reported by combining 5-FU/LV with irinotecan (FOLFIRI) or oxaliplatin (FOLFOX) for metastatic CRC [5-7]. Moreover, good responses to palliative chemotherapy enabled surgical resection with curative intent for some patients who initially had unresectable liver metastases by downsizing and downstaging the effect of chemotherapy [8]. In the past, the use of neoadjuvant chemotherapy was indicated for patients with unresectable colorectal liver metastasis, but recently, current trends of neoadjuvant chemotherapy is expanding to patients with initially resectable colorectal liver metastasis using an innovative combination of chemotherapeutic regimens. The most recent, a systematic review of neoadjuvant systemic chemotherapy for resectable colorectal liver metastases, demonstrated that objective responses of neoadjuvant chemotherapy can improve disease-free survival in patients with resectable colorectal liver metastases [9]. Furthermore, The National Comprehensive Cancer Network guideline recommended neoadjuvant chemotherapy for 2-3 months in patients with resectable colorectal metastases [10]. Thus, neoadjuvant chemotherapy prior to hepatectomy has become the standard treatment option. Herein, we attempted to develop a treatment strategy in the treatment of multiple colorectal liver metastases by using the FOLFIRI regimen. Patients who have more than two colorectal liver metastases were initiated with FOLFIRI chemotherapy, and then resectability was determined after three or six cycles of chemotherapy. Surgical treatment was performed in resectable cases, or, if progressive disease (PD) was observed during chemotherapy regimen-changed chemotherapy was delivered. If metastatic tumor showed controlled disease after 6 cycles of chemotherapy, further treatment was determined through resectability evaluation.
The aim of our prospective study was to evaluate the efficacy of neoadjuvant chemotherapy with FOLFIRI in colorectal multiple liver metastases regardless of resectability. The primary end point of the study was to observe the effects of treatment on the response rate. The secondary objectives were to observe R0 resection rate, complete response (CR) rate, and chemotherapy safety.
METHODS
Patients
Patients with multiple (at least two) colorectal liver metastases were enrolled in this study. Patients were recruited at seven tertiary referral hospitals. This study was approved by the Institutional Review Board of participating hospitals and written informed consent was obtained from each patient. Inclusion criteria were as follows: 1) histologically proven adenocarcinoma of colon and rectum, 2) multiple liver metastases confirmed by imaging study regardless of extrahepatic metastases, 3) age more than 18 years, 4) Eastern Cooperative Oncology Group performance status ≤2, 5) no history of previous chemotherapy, immunotherapy, or radiotherapy, 6) adequate bone marrow function (neutrophil counts, ≥1.5 × 109/L; hematocrit, ≥30%; and platelets, ≥100 × 109/L), liver function (total bilirubin ≤1.5 × the upper limit of normal), and renal function (serum creatinine ≤1.25 × the upper limit of normal). Patients having previously received adjuvant chemotherapy for a stage III colorectal cancer were eligible if the treatment had ended more than 6 months prior to enrollment in this study. Exclusion criteria included liver involvement of more than 70%, other malignancy, severe cardiac or pulmonary disease, pregnancy, severe medical disease, and intestinal obstruction or perforation.
Pretreatment evaluation included a physical examination, abdominopelvic computed tomography (CT), and carcinoembryonic antigen (CEA) assay. Positron emission tomography (PET) scanning was performed when possible.
Chemotherapy
Chemotherapy consisted of a regimen of irinotecan 180 mg/m2 administered intravenously over 30-90 mimutes, LV 400 mg/m2 (200 mg/m2 if L form was used) infused over 2 hours, 5-FU 400 mg/m2 intravenous bolus, and 5-FU 2,400 mg/m2 continuously infused for 46 hours on day 1. Treatment was delayed for 1 week in cases of neutropenia (≤1.5 × 109/L), platelet reduction (≤100 × 109/L) or significant nonhematological toxicity. Irinotecan and 5-FU doses were reduced by 25% in cases of grade 3/4 neutropenia or grade 3/4 diarrhea. In cases of grade 3/4 stomatitis, 5-FU doses were also only reduced by 25%. The treatment was interrupted in cases of grade 4 hematological toxicity or grade 4 gastrointestinal toxicity lasting for >1 week after a previous dose reduction or a delay in dose administration exceeding 2 weeks. The treatment was repeated every 2 weeks and response was assessed after completion of 3 cycles (6 weeks). If disease progression was identified, another chemotherapeutic regimen was begun in case of unresectable metastases or curative resection was performed in case of resectable metastases. If response was noted at the first assessment, chemotherapy was resumed until the completion of the other 3 cycles (6 weeks). After the second assessment was done, curative surgery was performed in case of resectable metastases or continuation of chemotherapy with another chemotherapeutic regimen was administered in cases of disease progression according to the discretion of the investigators in each institution (Fig. 1).
Fig. 1.

Study design. SD, stable disease; PD, progressive disease; FOLFIRI, 5-flurouracil/leucovorin with irinotecan; CTx, chemotherapy.
Assessments
Disease unresectability at the study outset was established for all patients by the hepatobiliary surgeon, oncologist and a radiologist from each institution. Criteria for initial unresectability of hepatic metastases were: unfavorable location of the metastases (contiguity with at least two hepatic veins, the inferior vena cava or the liver hilum); the number of metastases (more than six synchronous metastases in the same lobe and a major hepatectomy [resection of at least four segments] required, or more than three metastases in each of the two involved lobes both for synchronous and metachronous metastases); the size of the lesions (largest diameter >5 cm in at least one metastasis if there were six lesions in the same lobe, or three lesions if there was bilobar involvement); insufficient liver reserve (>70% of the liver was involved); and the presence of extrahepatic disease. Resectability of metastases following chemotherapy was assessed by the same team and was based on the response of lesions to chemotherapy and the likelihood of achieving R0 resection. Response to chemotherapy was assessed after three cycles (6 weeks) of treatment, and repeated one more time after six cycles (12 weeks) of treatment. Responses to chemotherapy were determined using World Health Organization criteria: an objective response was defined as either a CR (disappearance of all known disease) or a partial response (PR; ≥50% reduction in the size of the lesion from baseline). Following the assessment of response to chemotherapy, suitability for liver resection was determined. Toxicity was assessed by a combined oncologist/surgeon team, according to National Cancer Institute Common Toxicity Criteria, before each dose administration, at the operability assessment, and before the chemotherapy was re-started after intervention.
Statistical analysis
The main objective of this study was to assess the response rate of FOLFIRI chemotherapy in multiple colorectal liver metastases. On the basis of three phase II clinical trials using the FOLFIRI regimen for colorectal liver metastasis, the estimated response rate was 46.8% [7,11,12]. A response rate of 45% (P0) was considered as the minimum activity level of interest, while a response rate of 60% (P1) was promising. According to the two-stage phase II study of Simon's Optimal Design, 44 patients were calculated with β power of 80% and α error level of 0.05. Clinical response rates, resectability rates, and toxicity were calculated with 95% confidence interval.
RESULTS
Between May 2007 and September 2010, 44 patients were accrued. The characteristics of the 44 were summarized in Table 1. They consisted of 33 men and 11 women aging from 34 to 83 years (median, 62 years). Forty-two patients (95.6%) had more than clinical T3 stage and 39 patients (88.6%) had clinical N positive stage. The numbers of liver metastasis were as follows: 2 in 7 patients (15.9%), 3 in 9 patients (20.5%), 4 in 8 patients (18.2%), and 5 or more in 20 patients (45.4%). Imaging showed 161 liver metastases before chemotherapy in the 44 patients in the study. Of these, 128 had lesions smaller than 5 cm, 30 had lesions larger than 5 cm, and 3 were not identified.
Table 1.
Patient characteristics
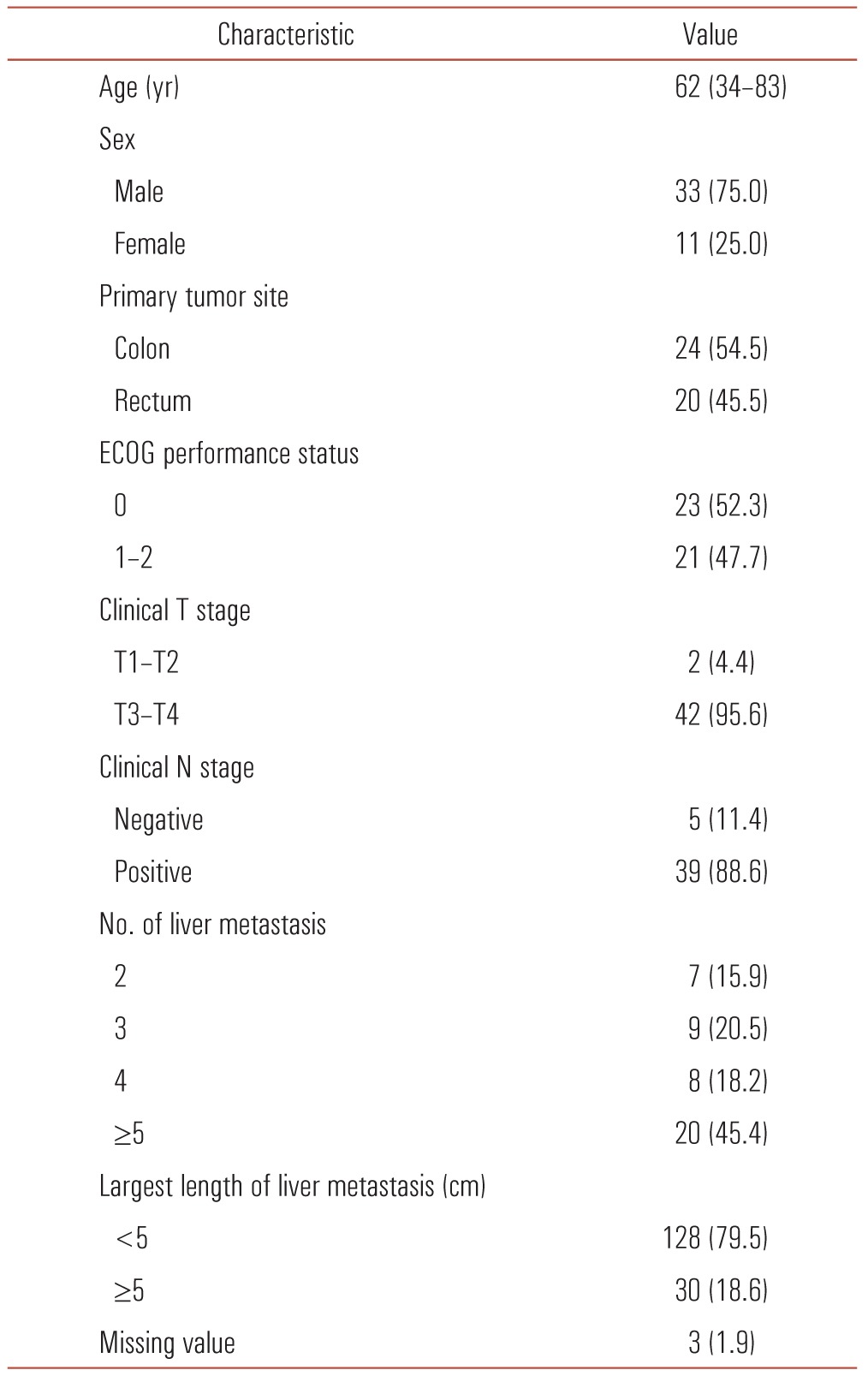
Values are presented as median (range) or number (%).
ECOG, Eastern Cooperative Oncology Group.
Of the 44 included patients, 27 patients (61.4%) had objective response (1 CR and 26 PR), and 4 patients (9.1%) had PD. Among patients with PD, aggravation of liver metastases was found in 3 cases and lung metastases were in 1 case (Table 2).
Table 2.
Response to chemotherapy
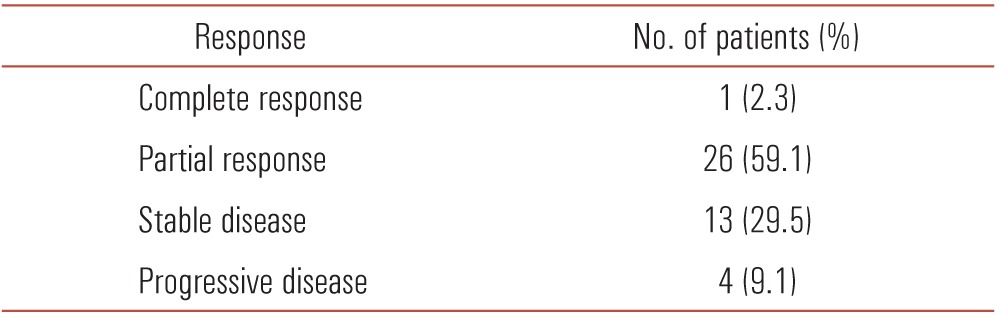
Objective response = complete response + partial response
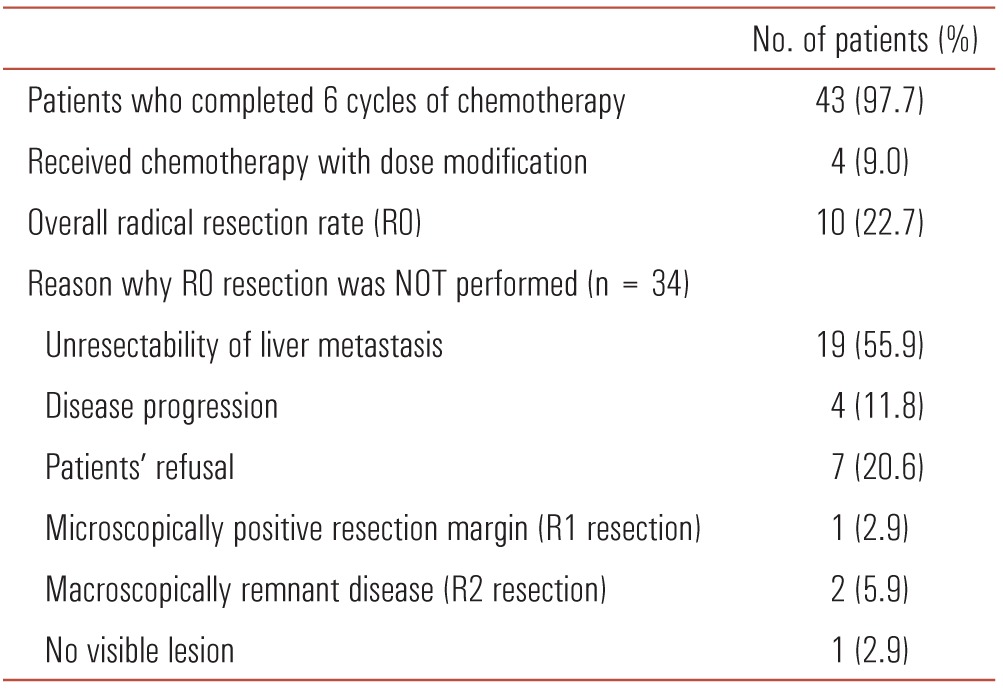
Forty-three patients (97.7%) completed six cycles of chemotherapy. The remaining one patient had to change the chemotherapeutic regimen because PD was noted after three cycles of chemotherapy (Fig. 2). Of the 44 patients enrolled, 10 patients (22.7%) underwent curative surgery (R0 resection) and 34 patients did not receive R0 resection. The reason for no R0 resection is described in Table 3.
Fig. 2.

Flowchart. CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease.
Table 3.
Treatment summary and R0 resection
Toxicities during chemotherapy were usually mild and tolerable. Grades 3 to 4 hematological toxicity consisted of anemia in 2 patients (4.5%) and neutropenia in 10 patients (22.6%). Grade 3 neutropenic fever was observed in 3 patients (13.6%). Grade 3 mucositis, nausea or vomiting, and diarrhea occurred in one, one, and three patients, respectively (Table 4). Dose modification of irinotecan and FU was necessary in 4 patients (9.0%) who showed grade 4 neutropenia.
Table 4.
Common adverse effect (NCI CTC ver. 2.0) (n = 44)
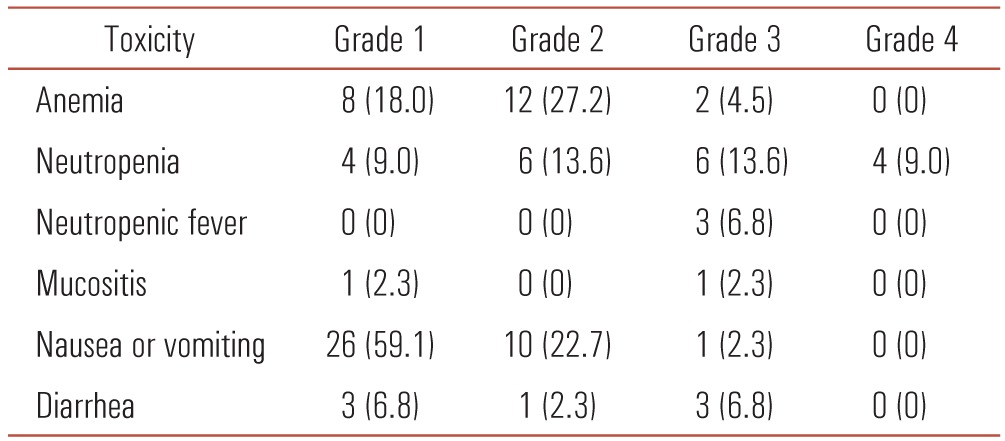
Values are presented as number (%).
NCI CTC, National Cancer Institute Common Terminology Criteria.
DISCUSSION
Systemic chemotherapy base of 5-fluorouracil with leucovorin has been considered standard regimen for colorectal cancer. However, its response rate is relatively low. A recently available chemotherapeutic regimen of 5-FU with irinotecan or oxaliplatin significantly improved oncologic outcomes in terms of progression-free survival, overall survival, and response rates [7,13-15]. Response rates were almost two times higher in 5-FU combined with irinotecan or oxaliplatin than 5-FU alone. These remarkable response rates led to evaluating the efficacy of neoadjuvant chemotherapy for colorectal liver metastases [9,13]. The efficacy of neoadjuvant chemotherapy for unresectable liver metastases has expanded its indication to patients with resectable colorectal liver metastases. Phase II studies using oxaliplatin- or irinotecan-based regimens have suggested efficacy and feasibility of neoadjuvant chemotherapy for resectable colorectal liver metastases [16,17]. A recent randomized controlled phase III trial, EORTC (European Organization for Research and Treatment of Cancer) inter group trial 40983, demonstrated that increased 3-year progression-free survival rates in perioperative chemotherapy group as compared with surgery alone group in patients with resectable colorectal liver metastases occurred [18]. In our study, objective response rate was 61.4%. This response rate was relatively high compared to similar clinical trials using FOLFIRI regimen [7,11,12]. However, neoadjuvant chemotherapy has several disadvantages. First, administration of preoperative chemotherapy may be associated with liver injury causing increased perioperative morbidity and mortality [19-21]. Combination of 5-FU and LV can develop hepatic steatosis [19]. Oxaliplatin-based regimens can increase the risk of vascular abnormalities in the liver [20,21]. Administration of irinotecan-based chemotherapy has been associated with steatosis and steatohepatitis [22,23]. Second, some liver metastases may disappear on radiologic imaging after neoadjuvant chemotherapy and these lesions may not be treatable. Benoist et al. [24] reviewed 66 liver metastases that had disappeared on CT scan. This study showed that 55 of 66 resolved liver metastases (83%) revealed residual cancer or early recurrence in situ. Therefore, they concluded that CR on CT scan did not mean cured. Another disadvantage of neoadjuvant chemotherapy is that some metastases become unresectable if they do not respond to chemotherapy. In the EORTC intergroup phase III study 40983, disease progression was identified in 12 out of 182 patients (7%) during systemic chemotherapy [18]. Thus, early decision of surgical resection should be considered if disease progression is identified in patients with neoadjuvant chemotherapy. In this study, neoadjuvant chemotherapy was indicated in patients with more than two liver metastases regardless of resectability, and resection or continuous chemotherapy using changed chemotherapeutic regimen was designed for disease progression.
The rate of R0 resection of 22.7% is one of the highest results among the studies using neoadjuvant chemotherapy for colorectal liver metastases. Moreover, a relatively high rate of objective response (61.4%) was demonstrated in our study. These results might be attributed to the effectiveness of FOLFIRI regimen for colorectal liver metastases and the inclusion of some patients who had initially resectable disease. The superiority of the FOLFIRI regimen was demonstrated in the BICC-C (bolus, infusional, or capecitabine with camptostar-celecoxib) study [25]. In the BICC-study, three different irinotecan-containing regimens (FOLFIRI, irinotecan plus bolus FU/LV, and irinotecan plus oral capecitabine) were compared in the first-line treatment of metastatic colorectal cancer. The median progression-free survival for FOLFIRI was 7.6 months as opposed to 5.9 months for irinotecan plus bolus FU/LV (P = 0.004) and 5.8 months for irinotecan plus oral capecitabine (P = 0.015). In contrast, studies comparing FOLFIRI with FOLFOX in patients with metastatic colorectal cancer showed similar efficacy [14,26]. Therefore, the addition of targeted agents to FOLFIRI or FOLFOX has been focused on the efficacy in the metastatic colorectal cancer currently. The efficacy of first-line treatment with cetuximab plus FOLFIRI has been evaluated in clinical trials in patients with epidermal growth factor receptor-expressing metastatic colorectal cancer. The CRYSTAL (Cetuximab Combined with Irinotecan in First-Line Therapy for Metastatic Colorectal Cancer) trial was a landmark phase III study to make a head-to-head comparison of the efficacy of cetuximab plus FOLFIRI and FOLFIRI alone for metastatic colorectal cancer [27]. In the subgroup of patients with KRAS wild type tumors, cetuximab plus FOLFIRI demonstrated more favorable oncologic outcomes than FOLFIRI alone with regard to both median progression-free survival (9.9 months vs. 8.7 months; hazard ration [HR], 0.68; 95% confidence interval [CI], 0.5 to 0.94) and overall survival (24.9 months vs. 21.0 months; HR, 0.84; 95% CI, 0.64 to 1.11). Moreover, cetuximab plus FOLFIRI group had a higher response rate than FOLFIRI alone (59.3% vs. 43.2%; odds ratio, 1.91; 95% CI, 1.24 to 2.93). The overall objective response rate was 46.9% in cetuximab plus FOLFIRI and 38.7% in FOLFIRI alone, respectively (P = 0.004). The higher objective response rate of our study compared to that of the CRYSTAL trial was due to the inclusion of some patients who had initially resectable disease as mentioned above.
The addition of bevacizumab to irinotecan-based chemotherapy in patients with metastatic colorectal cancer showed improved oncologic outcomes in first-line therapy according to the Hurwitz trial [28]. Hurwitz et al. [28] showed improved median duration of survival (20.3 months vs. 15.6 months, P < 0.001) and median duration of progression-free survival (10.6 months vs. 6.2 months, P < 0.001) in the bevacizumab plus irinotecan, bolus fluorouracil, and leucovorin (IFL) group than IFL alone. Bevacizumab plus FOLFIRI has been considered an upfront treatment strategy for stage IV colorectal cancer although no randomized controlled trial comparing FOLFIRI and FOLFIRI plus bevacizumab was conducted to confirm the Hurwitz trial results.
Our study showed that most of the patients (91%) completed the chemotherapy without dose modification. The toxicities of neoadjuvant chemotherapy were mild and manageable, and there was no mortality related to chemotherapy. The most frequent grade 3 or 4 toxicities were neutopenia (22.6%), neutropenic fever (6.8%), diarrhea (6.8%). anemia (4.5%), mucositis (2.3%), and nausea or vomiting (2.3%). These frequencies of grade 3 or 4 toxicities were reported similarly in other studies with the FOLFIRI regimen [29,30].
In conclusion, possibility of R0 resection, high rate of objective response, and tolerable toxicities after neoadjuvant chemotherapy for multiple colorectal liver metastases regardless of resectability, look promising in this study. However, early decision of surgical resection or changed chemotherapeutic regimen should be considered if disease progression is identified.
ACKNOWLEDGEMENTS
This work was supported by the research grant of the Chungbuk National University in 2012.
Footnotes
This study was presented at the Korean Surgical Society Annual Autumn Congress, Seoul, November 24 to 26, 2011
No potential conflict of interest relevant to this article was reported.
References
- 1.Boyle P, Langman JS. ABC of colorectal cancer: Epidemiology. BMJ. 2000;321:805–808. doi: 10.1136/bmj.321.7264.805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Landis SH, Murray T, Bolden S, Wingo PA. Cancer statistics, 1999. CA Cancer J Clin. 1999;49:8–31. 1. doi: 10.3322/canjclin.49.1.8. [DOI] [PubMed] [Google Scholar]
- 3.Steele G, Jr, Ravikumar TS. Resection of hepatic metastases from colorectal cancer. Biologic perspective. Ann Surg. 1989;210:127–138. doi: 10.1097/00000658-198908000-00001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Abdalla EK, Vauthey JN, Ellis LM, Ellis V, Pollock R, Broglio KR, et al. Recurrence and outcomes following hepatic resection, radiofrequency ablation, and combined resection/ablation for colorectal liver metastases. Ann Surg. 2004;239:818–825. doi: 10.1097/01.sla.0000128305.90650.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Choti MA, Sitzmann JV, Tiburi MF, Sumetchotimetha W, Rangsin R, Schulick RD, et al. Trends in long-term survival following liver resection for hepatic colorectal metastases. Ann Surg. 2002;235:759–766. doi: 10.1097/00000658-200206000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Fong Y, Blumgart LH. Hepatic colorectal metastasis: current status of surgical therapy. Oncology (Williston Park) 1998;12:1489–1498. [PubMed] [Google Scholar]
- 7.Pozzo C, Basso M, Cassano A, Quirino M, Schinzari G, Trigila N, et al. Neoadjuvant treatment of unresectable liver disease with irinotecan and 5-fluorouracil plus folinic acid in colorectal cancer patients. Ann Oncol. 2004;15:933–939. doi: 10.1093/annonc/mdh217. [DOI] [PubMed] [Google Scholar]
- 8.Bismuth H, Adam R, Levi F, Farabos C, Waechter F, Castaing D, et al. Resection of nonresectable liver metastases from colorectal cancer after neoadjuvant chemotherapy. Ann Surg. 1996;224:509–520. doi: 10.1097/00000658-199610000-00009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Chua TC, Saxena A, Liauw W, Kokandi A, Morris DL. Systematic review of randomized and nonrandomized trials of the clinical response and outcomes of neoadjuvant systemic chemotherapy for resectable colorectal liver metastases. Ann Surg Oncol. 2010;17:492–501. doi: 10.1245/s10434-009-0781-1. [DOI] [PubMed] [Google Scholar]
- 10.National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology (NCCN Guidelines): Colon/rectal cancer. ver. 1. 2010 [Internet] Fort Wathington: NCCN; c2012. [cited 2013 Apr 24]. Available from: http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. [Google Scholar]
- 11.Ho WM, Ma B, Mok T, Yeo W, Lai P, Lim R, et al. Liver resection after irinotecan, 5-fluorouracil, and folinic acid for patients with unresectable colorectal liver metastases: a multicenter phase II study by the Cancer Therapeutic Research Group. Med Oncol. 2005;22:303–312. doi: 10.1385/MO:22:3:303. [DOI] [PubMed] [Google Scholar]
- 12.Zelek L, Bugat R, Cherqui D, Ganem G, Valleur P, Guimbaud R, et al. Multimodal therapy with intravenous biweekly leucovorin, 5-fluorouracil and irinotecan combined with hepatic arterial infusion pirarubicin in non-resectable hepatic metastases from colorectal cancer (a European Association for Research in Oncology trial) Ann Oncol. 2003;14:1537–1542. doi: 10.1093/annonc/mdg404. [DOI] [PubMed] [Google Scholar]
- 13.Lévi F, Zidani R, Misset JL. Randomised multicentre trial of chronotherapy with oxaliplatin, fluorouracil, and folinic acid in metastatic colorectal cancer. International Organization for Cancer Chronotherapy. Lancet. 1997;350:681–686. doi: 10.1016/s0140-6736(97)03358-8. [DOI] [PubMed] [Google Scholar]
- 14.Tournigand C, Andre T, Achille E, Lledo G, Flesh M, Mery-Mignard D, et al. FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced colorectal cancer: a randomized GERCOR study. J Clin Oncol. 2004;22:229–237. doi: 10.1200/JCO.2004.05.113. [DOI] [PubMed] [Google Scholar]
- 15.Saltz LB, Cox JV, Blanke C, Rosen LS, Fehrenbacher L, Moore MJ, et al. Irinotecan plus fluorouracil and leucovorin for metastatic colorectal cancer. Irinotecan Study Group. N Engl J Med. 2000;343:905–914. doi: 10.1056/NEJM200009283431302. [DOI] [PubMed] [Google Scholar]
- 16.Wein A, Riedel C, Bruckl W, Merkel S, Ott R, Hanke B, et al. Neoadjuvant treatment with weekly high-dose 5-Fluorouracil as 24-hour infusion, folinic acid and oxaliplatin in patients with primary resectable liver metastases of colorectal cancer. Oncology. 2003;64:131–138. doi: 10.1159/000067772. [DOI] [PubMed] [Google Scholar]
- 17.Taïeb J, Artru P, Paye F, Louvet C, Perez N, Andre T, et al. Intensive systemic chemotherapy combined with surgery for metastatic colorectal cancer: results of a phase II study. J Clin Oncol. 2005;23:502–509. doi: 10.1200/JCO.2005.05.082. [DOI] [PubMed] [Google Scholar]
- 18.Nordlinger B, Sorbye H, Glimelius B, Poston GJ, Schlag PM, Rougier P, et al. Perioperative chemotherapy with FOLFOX4 and surgery versus surgery alone for resectable liver metastases from colorectal cancer (EORTC Intergroup trial 40983): a randomised controlled trial. Lancet. 2008;371:1007–1016. doi: 10.1016/S0140-6736(08)60455-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Peppercorn PD, Reznek RH, Wilson P, Slevin ML, Gupta RK. Demonstration of hepatic steatosis by computerized tomography in patients receiving 5-fluorouracil-based therapy for advanced colorectal cancer. Br J Cancer. 1998;77:2008–2011. doi: 10.1038/bjc.1998.333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rubbia-Brandt L, Audard V, Sartoretti P, Roth AD, Brezault C, Le Charpentier M, et al. Severe hepatic sinusoidal obstruction associated with oxaliplatin-based chemotherapy in patients with metastatic colorectal cancer. Ann Oncol. 2004;15:460–466. doi: 10.1093/annonc/mdh095. [DOI] [PubMed] [Google Scholar]
- 21.Aloia T, Sebagh M, Plasse M, Karam V, Levi F, Giacchetti S, et al. Liver histology and surgical outcomes after preoperative chemotherapy with fluorouracil plus oxaliplatin in colorectal cancer liver metastases. J Clin Oncol. 2006;24:4983–4990. doi: 10.1200/JCO.2006.05.8156. [DOI] [PubMed] [Google Scholar]
- 22.Kooby DA, Fong Y, Suriawinata A, Gonen M, Allen PJ, Klimstra DS, et al. Impact of steatosis on perioperative outcome following hepatic resection. J Gastrointest Surg. 2003;7:1034–1044. doi: 10.1016/j.gassur.2003.09.012. [DOI] [PubMed] [Google Scholar]
- 23.Fernandez FG, Ritter J, Goodwin JW, Linehan DC, Hawkins WG, Strasberg SM. Effect of steatohepatitis associated with irinotecan or oxaliplatin pretreatment on resectability of hepatic colorectal metastases. J Am Coll Surg. 2005;200:845–853. doi: 10.1016/j.jamcollsurg.2005.01.024. [DOI] [PubMed] [Google Scholar]
- 24.Benoist S, Brouquet A, Penna C, Julie C, El Hajjam M, Chagnon S, et al. Complete response of colorectal liver metastases after chemotherapy: does it mean cure? J Clin Oncol. 2006;24:3939–3945. doi: 10.1200/JCO.2006.05.8727. [DOI] [PubMed] [Google Scholar]
- 25.Fuchs CS, Marshall J, Mitchell E, Wierzbicki R, Ganju V, Jeffery M, et al. Randomized, controlled trial of irinotecan plus infusional, bolus, or oral fluoropyrimidines in first-line treatment of metastatic colorectal cancer: results from the BICC-C Study. J Clin Oncol. 2007;25:4779–4786. doi: 10.1200/JCO.2007.11.3357. [DOI] [PubMed] [Google Scholar]
- 26.Colucci G, Gebbia V, Paoletti G, Giuliani F, Caruso M, Gebbia N, et al. Phase III randomized trial of FOLFIRI versus FOLFOX4 in the treatment of advanced colorectal cancer: a multicenter study of the Gruppo Oncologico Dell'Italia Meridionale. J Clin Oncol. 2005;23:4866–4875. doi: 10.1200/JCO.2005.07.113. [DOI] [PubMed] [Google Scholar]
- 27.Van Cutsem E, Kohne CH, Hitre E, Zaluski J, Chang Chien CR, Makhson A, et al. Cetuximab and chemotherapy as initial treatment for metastatic colorectal cancer. N Engl J Med. 2009;360:1408–1417. doi: 10.1056/NEJMoa0805019. [DOI] [PubMed] [Google Scholar]
- 28.Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J, Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leucovorin for metastatic colorectal cancer. N Engl J Med. 2004;350:2335–2342. doi: 10.1056/NEJMoa032691. [DOI] [PubMed] [Google Scholar]
- 29.Ychou M, Hohenberger W, Thezenas S, Navarro M, Maurel J, Bokemeyer C, et al. A randomized phase III study comparing adjuvant 5-fluorouracil/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer. Ann Oncol. 2009;20:1964–1970. doi: 10.1093/annonc/mdp236. [DOI] [PubMed] [Google Scholar]
- 30.Bathe OF, Ernst S, Sutherland FR, Dixon E, Butts C, Bigam D, et al. A phase II experience with neoadjuvant irinotecan (CPT-11), 5-fluorouracil (5-FU) and leucovorin (LV) for colorectal liver metastases. BMC Cancer. 2009;9:156. doi: 10.1186/1471-2407-9-156. [DOI] [PMC free article] [PubMed] [Google Scholar]