

Abstract
This study describes the epidemiology of hemorrhagic fever with renal syndrome (HFRS) in the past 10 yr (2001-2010) in Korea. During this period, a total of 3,953 HFRS patients and an average prevalence rate of 0.81 per 100,000 population were recorded, with a total of 40 fatal cases, corresponding to a case fatality rate of 1.01%. More HFRS cases were found in men than in women (57% vs 43%), and a higher prevalence rate of HFRS was observed in patients older than 40 yr (82.1%). The highest numbers of HFRS cases were found amongst farmers (35.6%). The majority of HFRS cases (71.3%) occurred in the last quarter of the calendar year (October to December). More HFRS cases occurred in the western part than in the eastern part of Korea (68.9% vs 31.1%). The incidence of HFRS was significantly higher (P < 0.001) in rural areas than in urban areas (80.3% vs 19.7%). HFRS still occurs commonly among men, in autumn, and in western rural area of Korea.
Keywords: Hemorrhagic Fever with Renal Syndrome, Epidemiology, Autumn, Rural Area
Hantavirus infection induces 2 different diseases, hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS), mainly in Korea, far east Russia, and China and in the United States, respectively (1, 2). The viruses are transmitted to humans by the inhalation of excreta of rodents infected with hantaviruses (3). HFRS was first recognized during the Korean War in the early 1950s, and although a hantavirus vaccine has been developed, the disease remains a serious problem in Asia and Europe (1, 4), and especially among soldiers in Korea (5, 6). A 2006 report describes HFRS epidemiology in endemic regions in Korea during a relatively short period, 1995-1998 (7); however, an updated epidemiological study is necessary to better understand the current status of HFRS in Korea. This study provides a comprehensive epidemiological overview of HFRS during the past decade in Korea.
Raw data were utilized from the National Notifiable Disease Surveillance System (NNDSS) website of the Korean Center for Disease Control and Prevention (KCDC) (2001-2010) (8), and "HFRS," Incidence for Communicable Diseases (Category III), Yearbook of Health and Welfare Statistics by the Ministry of Health and Welfare, Republic of Korea (MHW, ROK), 2001-2010 (9). During the period 2001-2010, there were 3,953 patients and 40 fatal cases of HFRS (Table 1). The prevalence rate (PR) of HFRS per 100,000 population and case fatality rate (CFR) were estimated by the criteria established by the World Health Organization (WHO), and the upper and lower limits of the 95% confidence interval (CI) were calculated. Statistically significant differences between the epidemiological aspects were determined at P < 0.05 and P < 0.01 using the chi-square test or the paired t-test. The data analyses were carried out using the statistical system software included in Microsoft Excel 2007.
Table 1.
Prevalence rate, case fatality rate, and other aspects of HFRS
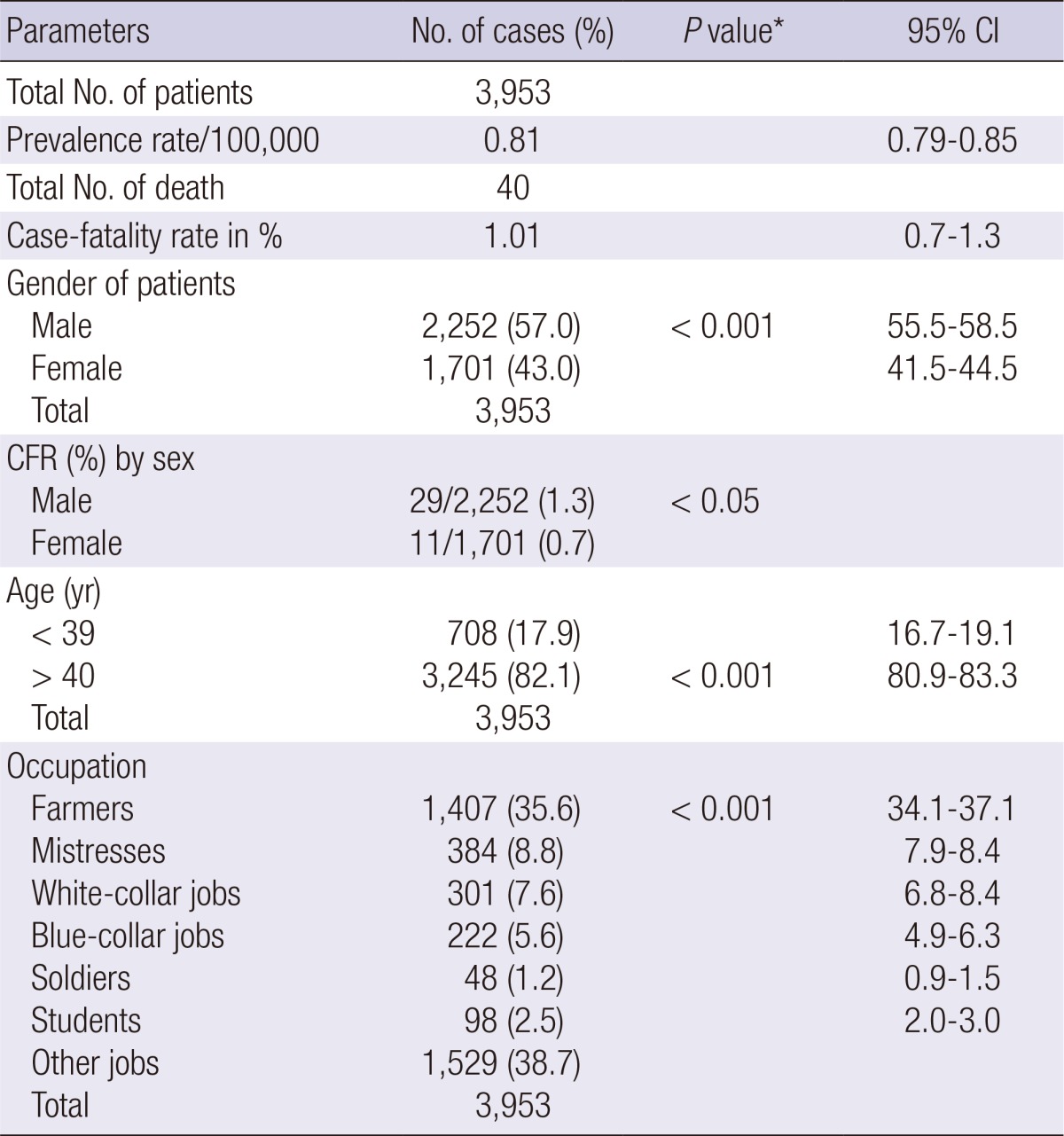
95% CI, Confidence interval of 95% of the rate; CFR, Case fatality rate.
*Chi-square analysis indicated a significant difference from the total value.
As shown in Table 1, the HFRS cases were analyzed according to the PR, CFR, gender, age, and occupation of the infected individuals. There were a total of 3,953 HFRS patients with an average PR of 0.81 (95% CI, 0.79-0.85) per 100,000 population and a total of 40 fatal cases with a CFR of 1.01% (95% CI, 0.7-1.3). A significantly higher number (P < 0.001) of men were infected than women (57% vs 43%). The CFR was also significantly higher (P < 0.05) in men than in women (1.3% vs 0.7%). The distribution of HFRS cases by age clearly showed a significantly higher incidence of HFRS in people older than 40 yr (P < 0.001). When the HFRS patients were analyzed by occupation, significantly higher (P < 0.001) number of infections occurred among farmers (35.6%) than among those in other job groups (38.7%).
HFRS cases were analyzed by season, geography, and resident area of individuals. The PR of HFRS in spring, summer, autumn, and winter was 7.0%, 9.1%, 61.4%, and 22.5%, respectively. The PR of HFRS in autumn was significantly higher than that in other seasons (P < 0.001). The HFRS cases predominantly occurred during the last quarter of the calendar year (October, November, and December). A significantly higher number of HFRS cases (P < 0.001) was reported in the western part (provinces of Gyeonggi, Chungnam, Jeonbuk, Jeonnam, and Jeju and major cities of Seoul, Incheon, Daejeon, and Gwangju, 68.9%) than in the eastern part (provinces of Gangwon, Chungbuk, Gyeongbuk, Gyeongnam and major cities of Daegu, Ulsan, and Busan, 31.1%) of Korea (Fig. 1). Finally, HFRS cases were significantly higher (P < 0.001) in rural areas (80.3%) than in urban areas (19.7%).
Fig. 1.

Number of HFRS cases by administrative provinces and special cities of Korea during 2001-2010.
This study provides a more updated HFRS prevalence status in the whole population of Korea during the past decade. A previous report addressed annual prevalence and incidence rates of HFRS during the late 1990s only in endemic areas near the demilitarized zone (DMZ) between South and North Korea (7). The prevalence rate per 100,000 population of HFRS determined in this study was 0.81. In contrast, the annual prevalence of HFRS determined in the previous study was 40-64 per 100,000 military population in the DMZ areas. Therefore, the prevalence of HFRS could be seriously affected by the regions and populations examined.
This study confirmed that the incidence of HFRS significantly increased in the autumn. In the previous report, an almost identical pattern of HFRS incidence was identified in soldiers in endemic areas (7). Higher incidence of HFRS in the autumn, versus other seasons, could be attributed to the high numbers of hantavirus-infected rodents in Korea during this time (10, 11). Seroprevalence of hantaviruses in wild rodents in Korea confidently demonstrated that most wild rodent hantavirus infections occur in the autumn. Therefore, increased outdoor activity of people in the autumn, especially in rural areas, would increase the probability of hantavirus infection, leading to a higher incidence of HFRS in the autumn among farmers.
In this study, the HFRS patient numbers and CFR were significantly higher in men than in women. However, a recent study conducted in China reported that the incidence of HFRS is greater in men, but the CFR is higher in women than in men (12). The discrepancy of CFRs between Korean and Chinese HFRS patients is an interesting question that requires more thorough epidemiological studies to resolve. In addition, many more HFRS patients were identified in people older than 40 yr and in the western part of Korea. This could be partially explained by a larger population in the western part of Korea and the advanced ages of farmers.
In conclusion, HFRS still occurs commonly among men, in autumn, and in western rural area of Korea. These comprehensive epidemiological data would be valuable for developing HFRS control strategies in Korea.
Footnotes
This paper was supported by Konkuk University in 2013.
The authors have no conflicts of interest to disclose.
References
- 1.Jonsson CB, Figueiredo LT, Vapalahti O. A global perspective on hantavirus ecology, epidemiology, and disease. Clin Microbiol Rev. 2010;23:412–441. doi: 10.1128/CMR.00062-09. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lee HW, Lee PW, Johnson KM. Isolation of the etiologic agent of Korean Hemorrhagic fever. J Infect Dis. 1978;137:298–308. doi: 10.1093/infdis/137.3.298. [DOI] [PubMed] [Google Scholar]
- 3.Lee HW, van der Groen G. Hemorrhagic fever with renal syndrome. Prog Med Virol. 1989;36:62–102. [PubMed] [Google Scholar]
- 4.Smadel JE. Epidemic hemorrhagic fever. Am J Public Health Nations Health. 1953;43:1327–1330. doi: 10.2105/ajph.43.10.1327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Park K, Kim CS, Moon KT. Protective effectiveness of hantavirus vaccine. Emerg Infect Dis. 2004;10:2218–2220. doi: 10.3201/eid1012.040684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Song JW, Moon SS, Gu SH, Song KJ, Baek LJ, Kim HC, Kijek T, O'Guinn ML, Lee JS, Turell MJ, et al. Hemorrhagic fever with renal syndrome in 4 US soldiers, South Korea, 2005. Emerg Infect Dis. 2009;15:1833–1836. doi: 10.3201/eid1511.090076. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Song JY, Chun BC, Kim SD, Baek LJ, Kim SH, Sohn JW, Cheong HJ, Kim WJ, Park SC, Kim MJ. Epidemiology of hemorrhagic fever with renal syndrome in endemic area of the Republic of Korea, 1995-1998. J Korean Med Sci. 2006;21:614–620. doi: 10.3346/jkms.2006.21.4.614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Korea Center for Disease Control and Prevention. Hemorrhagic fever with renal syndrome: statistical system of the national notifiable disease surveillance system (2001-2010) Available at http://www.cdc.go.kr.
- 9.Ministry of Health and Welfare, Republic of Korea (MHW, ROK) Hemorrhagic fever with renal syndrome, Incidence for communicable diseases (category III). Yearbook of Health and Welfare Statistics (2001-2010) Seoul: Ministry of Health and Welfare; 2010. [Google Scholar]
- 10.Lim MY, Ryou J, Kim SY, Shin EH, Yoo YJ, Yun SM, Noh YT, Han MG, Ju YR. Seroprevalence of hantaviruses in small wild mammals trapped in South Korea from 2005 to 2010. J Vector Ecol. 2012;37:97–101. doi: 10.1111/j.1948-7134.2012.00205.x. [DOI] [PubMed] [Google Scholar]
- 11.Ryou J, Lee HI, Yoo YJ, Noh YT, Yun SM, Kim SY, Shin EH, Han MG, Ju YR. Prevalence of hantavirus infection in wild rodents from five provinces in Korea, 2007. J Wildl Dis. 2011;47:427–432. doi: 10.7589/0090-3558-47.2.427. [DOI] [PubMed] [Google Scholar]
- 12.Klein SL, Marks MA, Li W, Glass GE, Fang LQ, Ma JQ, Cao WC. Sex differences in the incidence and case fatality rates from hemorrhagic fever with renal syndrome in China, 2004-2008. Clin Infect Dis. 2011;52:1414–1421. doi: 10.1093/cid/cir232. [DOI] [PMC free article] [PubMed] [Google Scholar]