

Abstract
Cholecystectomy is a common procedure. Abnormalities in the anatomy of the biliary system are common but an abnormal location of the gallbladder is much rarer. Despite frequent pre-operative imaging, the aberrant location of the gallbladder is commonly discovered at surgery. This article presents a case of a patient with the gallbladder located to the left of the falciform ligament in the absence of situs inversus totalis that presented with right upper quadrant pain. A laparoscopic cholecystectomy was performed and it was noted that the cystic duct originated from the right side. The presence of a left sided gall bladder is often associated with various biliary, portal venous and other anomalies that might lead to intra-operative injuries. The spectrum of unusual positions and anatomical gallbladder abnormalities is reviewed in order to facilitate elective and emergent cholecystectomy as well as other hepatobiliary procedures. With proper identification of the anatomy, minimally invasive approaches are still considered safe.
Keywords: Left sided gallbladder, Laparoscopic cholecystectomy, Sinistroposition of the gallbladder, Situs inversus, Bile duct anomaly, Liver anomalies, Portal vein anomaly, Liver transplant
Core tip: In the absence of situs inversus, left sided gallbladders are rare anomalies. They are most commonly encountered during surgery as they usually present with right sided pain and routine preoperative testing fails to identify them. Various biliary, portal venous and other anomalies are associated with left sided gallbladders and their spectrum is reviewed in this article. Recognition of these associated anomalies will help achieve safety in hepatobiliary procedures and prevent injuries.
INTRODUCTION
Located to the left side of the falciform ligament, left sided gallbladders are rare anomalies and a result of a distinct embryological process. They are seldom identified pre-operatively, and as they are associated with various biliary, portal venous, and other anomalies, the surgeon must be familiar with the potential variations that he might encounter. A left sided gallbladder was encountered during a laparoscopic cholecystectomy at our institution in a patient that presented with right sided abdominal pain. Careful dissection revealed that the cystic duct was crossing from the right side and that critical view was established with the identification of the cystic artery. The spectrum of the possible anomalies associated with left sided gallbladders is wide but does not preclude the successful performance of a minimally invasive cholecystectomy or any other hepatobiliary procedure.
CASE REPORT
The patient is a 64-year-old female with multiple medical problems including type II diabetes mellitus, a history of deep venous thrombosis and pulmonary embolism, kidney stones and hypertension who presented to the hospital with a five day history of sharp, right-sided abdominal pain radiating to her epigastric area, chest, bilateral back, right flank and right shoulder. This was the first time patient experienced this kind of pain, and she denied history of prior cholecystitis. She had a history prior extracorporeal shockwave ureteral lithotripsy, but the admitting discomfort was different from that of prior renal colic. Three months prior to the admission, the patient had colonoscopy and esophagogastroduodenoscopy, which were normal.
On physical examination she had stable vital signs and was afebrile. The abdomen was nondistended and nontender. Laboratory data on admission revealed a normal white call count, normal total bilirubin, normal alkaline phosphatase, normal aspartate aminotransferase (AST) and normal alanine aminotransferase (ALT) amylase and lipase were not elevated. An abdominal ultrasound revealed gallbladder sludge with small calculi, no gallbladder wall thickening and no dilatation of the biliary tract. Computed tomography (CT) of the abdomen and pelvis showed gallstones without CT-evidence of cholecystitis, and biliary dilatation up to 9 mm. Secondary to the dilatation of the common bile duct (CBD) on the CT, magnetic resonance cholangiopancreatography (MRCP) was performed and demonstrated cholelithiasis without signs of choledocholithiasis.
During this admission, laparoscopic cholecystectomy was performed. Upon insertion of the camera into the umbilical port, the gallbladder was visualized and was located immediately to the left of the falciform ligament, and below segment III of the liver. The gallbladder wall was mildly edematous. The cystic duct and the cystic artery were identified, and it was observed that the artery was to the right of the duct. After the identification of the critical view of safety, the cystic artery and the cystic duct were clipped and divided in a standard fashion. The operation was completed without difficulties and the patient recovered and was discharged home on the second postoperative day. Pathological evaluation identified multiple small, less that 1 mm stones and the thickness of the gallbladder wall measured 3 mm, consistent with chronic cholecystitis and cholelithiasis.
The CT scan of the abdomen did not appear to demonstrate an abnormal location of the gallbladder (Figure 1A) but the finding of the gallbladder to the left of the falciform ligament was present on preoperative MRCP (Figure 1B).
Figure 1.
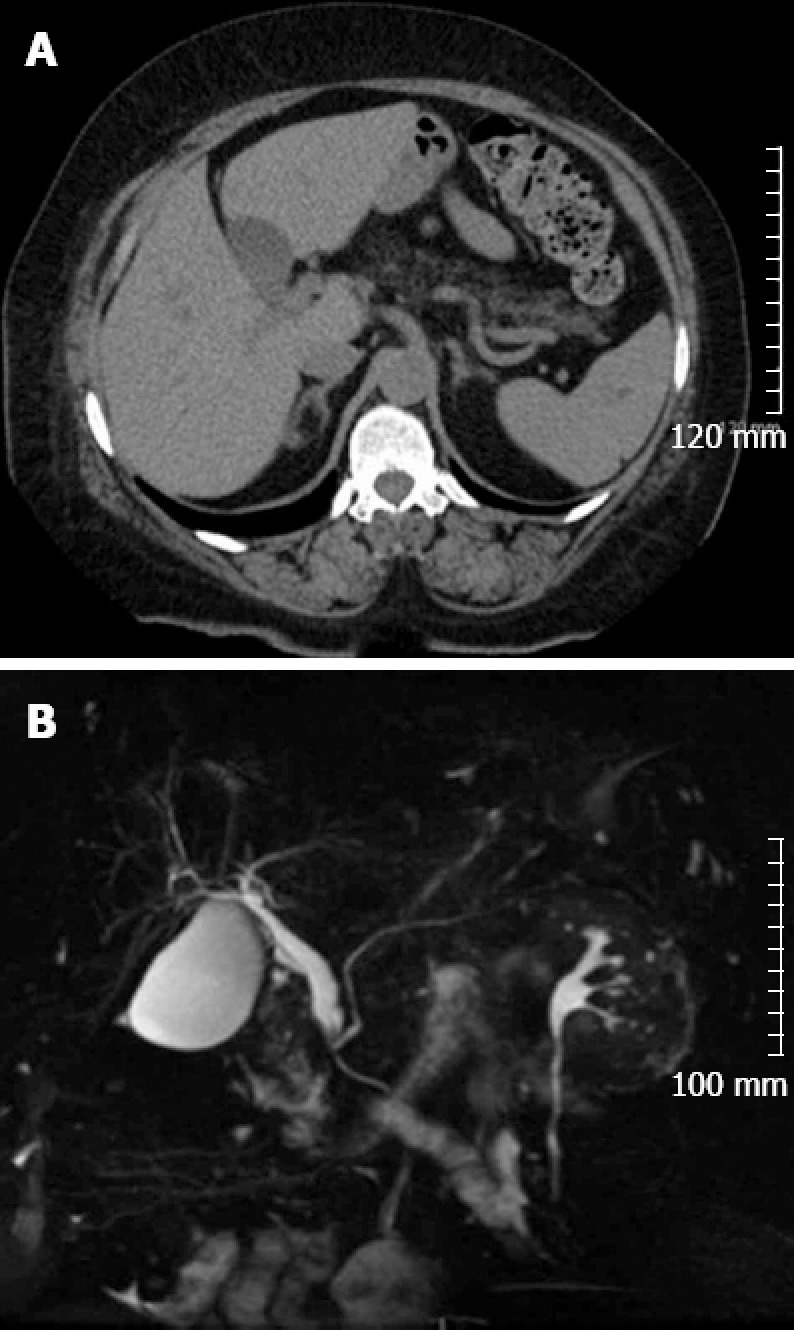
Radiological images of the abdomen. A: Computed tomography scan without contrast demonstrating the gallbladder to the left of the falciform ligament; B: Magnetic resonance cholangiopancreatography showing a dilated common bile duct on coronal view.
DISCUSSION
Left sided gallbladders without situs inversus are rare and have a prevalence of 0.04%-0.3%[1,2]. A distinction should be made between gallbladders that are truly left sided also referred to as sinistroposition and gallbladders located to the left of abnormally located right-sided round ligaments[3]. True left sided gallbladders exist because of two possible embryological etiologies. The first mechanism is due to the attachment and migration of the gallbladder to the left lobe in which case the cystic duct is in a normal anatomic position and crosses in front of the common duct from right to left, as is the case in the case reported herein[4]. The second mechanism is formation of the gallbladder by budding directly from the left side in which case the cystic duct joins the CBD or left hepatic duct from the left side[4,5]. Right-sided round ligaments on the other hand, are associated with a normal position and anatomy of the cystic duct, and with anomalous portal venous branching, which is crucial during the performance a hepatectomy, for example[3].
Despite being truly left-sided, gallbladders with sinistroposition almost always cause right-sided symptoms when they become symptomatic making their preoperative diagnosis difficult[2]. It is believed that the visceral nerve fibers do no transpose with the gallbladder causing right-sided pain[6]. In the present case, the abnormal position of the gallbladder was only discovered at surgery, despite the patient having undergone preoperative ultrasound, CT, MRCP and endoscopic ultrasound, which is consistent with other case reports[2,3,7]. However, an intraoperative finding of a left sided gallbladder should not preclude the decision to proceed laparoscopically with minor modifications in the standard approach and port placement. Donthi et al[8], for example, placed their ports in a mirror image to a typical right-sided standard laparoscopic cholecystectomy, achieving adequate exposure and traction for dissection. Keeping in mind the possible anatomic variations associated with the condition along with careful dissection and the establishment of the critical view of safety, with or without intra-operative cystic duct cholangiography, will minimize complications. Ligation and division of the cystic duct and artery should be close to the gallbladder. The surgeon should make every effort to identify key anatomic landmarks as one would attempt to do during a standard cholecystectomy. Cases of single port cholecystectomy have even been reported in patients with situs inversus without adverse occurrences[9,10]. A more comprehensive literature review of patients with left sided gallbladders without situs inversus undergoing surgery is summarized in Table 1.
Table 1.
Literature review of previously reported left-sided gallbladders without situs inversus undergoing surgery
| Ref. | Location | Reported number of patients | Clinical presentation | Diagnosis made pre-op? | Surgical treatment (cholecystectomy) | Comments |
| [1] | Hungary | 1 in 2536 | Right sided abdominal pain | No | Open | |
| [2] | The Netherlands | 5 in 1764 | Right sided abdominal pain | 1 of 5 | Laparoscopic | Sinistroposition |
| [3] | Japan | 3 in 1621 | cholecystitis, 2 incidental during liver surgery | No | Open | Emphasis on right sided round ligament/reported 105 cases in literature until then |
| [5] | India | Case report | Right sided abdominal pain | No | Laparoscopic | |
| [6] | India | 1 in 1258 | Right sided abdominal pain | No | Laparoscopic | Dextrocardia present |
| [7] | United Kingdom | Case report | Right sided abdominal pain | No | Open | |
| [11] | Japan | Case report | Incidental/liver cancer | Yes | Open | Used drop infusion cholangiography for diagnosis and CT scan |
| [12] | Greece | Case report | Epigastric pain | No | Laparoscopic | |
| [13] | Ohio, United States | Case report | Right sided abdominal pain | No | Laparoscopic | Duplication of CBD |
| [14] | Serbia | 2 patients | 1 asymptomatic/1 right sided abdominal pain | No | Open | Associated with liver cysts |
| [15] | India | Case report | Right sided abdominal pain | No | Open | |
| [16] | United Kingdom | Case report | Epigastric pain | Yes | Open | Diagnosis by radio-opaque stone on the left side |
| [17] | Florida, United States | Case report | Right sided abdominal pain | No | Laparoscopic | Intra-op cholangiogram performed |
| [18] | New York, United States | Case report | Right sided abdominal pain | No | Open | Association with giardia lamblia infection |
| [19] | Tunis | Case report | Right sided pain | No | Laparoscopic | Normal intra-op cholangiogram |
| [20] | Japan | Case report | Back pain | No | Laparoscopic | Associated right portal vein anomaly |
| [21] | St. Louis, United States | Case report | Right sided pain | No | Laparoscopic | CBD injury because of anomalous left sided common hepatic duct |
| [22] | South Korea | Case report | Right sided pain | No | Laparoscopic | Pre-op percutaneous cholecystostomy with hepatic injury |
| [23] | Japan | Case report | Right sided pain | Yes | Laparoscopic | Preop diagnosis with DIC CT and lap CBD exploration |
| [24] | South Korea | 3 | Omphalocele with herniated liver | Yes | None | Association with omphalocele |
| [25] | Japan | 2 | Right sided pain | No | Laparoscopic | |
| [26] | Japan | Case report | Right sided pain | No | Open | Associated with hypoplasia of the left lobe of the liver |
| [27] | Japan | Case report | Right sided pain | No | Open | Right sided round ligament |
| [28] | Japan | Case report | Living donor transplant | No | Open | Association with portal vein anomalous branching |
| [29] | South Africa | Case report | Right sided pain | Yes | Laparoscopic | Diagnosed on CT pre-op |
| [30] | China | 3 | Living donor transplant | Suspected | Open | Biliary, arterial, and portal venous anomalies |
| [31] | Italy | Case report | Right sided pain | No | Laparoscopic | |
| [32] | Japan | 3 | Living donor transplant | Yes | Open | Portal venous anomaly |
CBD: Common bile duct; DIC: Drop infusion cholangiography; MRCP: Magnetic resonance cholangiopancreatography; CT: Computed tomography.
In a conclusion, a left-sided gallbladder is an unusual anatomic variant. Patients commonly present with typical biliary colic and cholecystitis symptoms. The abnormal location might not be discovered until the start of the laparoscopic procedure. Proper anatomic identification of key landmarks will permit most or all of these procedures to be performed using minimally invasive techniques.
Footnotes
P- Reviewers Garg P, Liu XB S- Editor Wen LL L- Editor A E- Editor Ma S
References
- 1.Rozsos I, Ferenczy J, Vincze K, Rainer S. Left-sided gallbladder. Magy Seb. 2002;55:329–330. [PubMed] [Google Scholar]
- 2.Idu M, Jakimowicz J, Iuppa A, Cuschieri A. Hepatobiliary anatomy in patients with transposition of the gallbladder: implications for safe laparoscopic cholecystectomy. Br J Surg. 1996;83:1442–1443. doi: 10.1002/bjs.1800831037. [DOI] [PubMed] [Google Scholar]
- 3.Nagai M, Kubota K, Kawasaki S, Takayama T, BandaiY M. Are left-sided gallbladders really located on the left side. Ann Surg. 1997;225:274–280. doi: 10.1097/00000658-199703000-00006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gross RE. Congenital anomalies of the gallbladder. Arch Surg. 1936;32:131–162. [Google Scholar]
- 5.Reddy PK, Subramanian RV, Yuvaraja S. Laparoscopic cholecystectomy for left-sided gallbladder (sinistroposition) JSLS. 2005;9:356–357. [PMC free article] [PubMed] [Google Scholar]
- 6.Sadhu S, Jahangir TA, Roy MK. Left-sided gallbladder discovered during laparoscopic cholecystectomy in a patient with dextrocardia. Indian J Surg. 2012;74:186–188. doi: 10.1007/s12262-011-0261-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wong LS, Rusby J, Ismail T. Left-sided gall bladder: a diagnostic and surgical challenge. ANZ J Surg. 2001;71:557–558. doi: 10.1046/j.1440-1622.2001.02195.x. [DOI] [PubMed] [Google Scholar]
- 8.Donthi R, Thomas DJ, Sanders D, Schmidt SP. Report of laparoscopic cholecystectomy in two patients with left-sided gallbladders. JSLS. 2001;5:53–56. [PMC free article] [PubMed] [Google Scholar]
- 9.Han HJ, Choi SB, Kim CY, Kim WB, Song TJ, Choi SY. Single-incision multiport laparoscopic cholecystectomy for a patient with situs inversus totalis: report of a case. Surg Today. 2011;41:877–880. doi: 10.1007/s00595-010-4387-9. [DOI] [PubMed] [Google Scholar]
- 10.de Campos Martins MV, Pantaleão Falcão JL, Skinovsky J, de Faria GM. Single-port cholecystectomy in a patient with situs inversus totalis presenting with cholelithiasis: a case report. J Med Case Rep. 2012;6:96. doi: 10.1186/1752-1947-6-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Abe T, Kajiyama K, Harimoto N, Gion T, Shirabe K, Nagaie T. Resection of metastatic liver cancer in a patient with a left-sided gallbladder and intrahepatic portal vein and bile duct anomalies: A case report. Int J Surg Case Rep. 2012;3:147–150. doi: 10.1016/j.ijscr.2012.01.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zografos GC, Lagoudianakis EE, Grosomanidis D, Koronakis N, Tsekouras D, Chrysikos J, Filis K, Manouras A. Management of incidental left-sided gallbladder. JSLS. 2009;13:273–275. [PMC free article] [PubMed] [Google Scholar]
- 13.Bender EA, Springhetti S, Shemisa K, Wittenauer J. Left-sided gallbladder (sinistroposition) with duplication of the common bile duct. JSLS. 2007;11:148–150. [PMC free article] [PubMed] [Google Scholar]
- 14.Colovic R, Colovic N, Barisic G, Atkinson HD, Krivokapic Z. Left-sided gallbladder associated with congenital liver cyst. HPB (Oxford) 2006;8:157–158. doi: 10.1080/13651820410016642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dhulkotia A, Kumar S, Kabra V, Shukla HS. Aberrant gallbladder situated beneath the left lobe of liver. HPB (Oxford) 2002;4:39–42. doi: 10.1080/136518202753598726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Qureshi I, Awad Z. Aberrant presentation of the gallbladder during laparoscopic cholecystectomy. JSLS. 2009;13:605–607. doi: 10.4293/108680809X12589999538075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McGowan JM, Nussbaum CC, Burroughs EW. Cholecystitis due to Giardia Lamblia in a Left-sided Gallbladder. Ann Surg. 1948;128:1032–1037. doi: 10.1097/00000658-194811000-00026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Strong RW, Fawcett J, Hatzifotis M, Hodgkinson P, Lynch S, O’Rourke T, Slater K, Yeung S. Surgical implications of a left-sided gallbladder. Am J Surg. 2013;206:59–63. doi: 10.1016/j.amjsurg.2012.10.035. [DOI] [PubMed] [Google Scholar]
- 19.Makni A, Magherbi H, Ksantini R, Rebai W, Safta ZB. Left-sided gallbladder: an incidental finding on laparoscopic cholecystectomy. Asian J Surg. 2012;35:93–95. doi: 10.1016/j.asjsur.2012.04.011. [DOI] [PubMed] [Google Scholar]
- 20.Kawai R, Miyata K, Yuasa N, Takeuchi E, Goto Y, Miyake H, Nagai H, Hattori M, Imura J, Hayashi Y, et al. True left-sided gallbladder with a portal anomaly: report of a case. Surg Today. 2012;42:1130–1134. doi: 10.1007/s00595-011-0093-5. [DOI] [PubMed] [Google Scholar]
- 21.Moo-Young TA, Picus DD, Teefey S, Strasberg SM. Common bile duct injury following laparoscopic cholecystectomy in the setting of sinistroposition of the galladder and biliary confluence: a case report. J Gastrointest Surg. 2010;14:166–170. doi: 10.1007/s11605-009-0989-1. [DOI] [PubMed] [Google Scholar]
- 22.Jung HS, Huh K, Shin YH, Kim JK, Yun CS, Park CH, Jang JB. Left-sided gallbladder: a complicated percutaneous cholecystostomy and subsequent hepatic embolisation. Br J Radiol. 2009;82:e141–e144. doi: 10.1259/bjr/59092209. [DOI] [PubMed] [Google Scholar]
- 23.Matsumura N, Tokumura H, Yasumoto A, Sasaki H, Yamasaki M, Musya H, Fukuyama S, Takahashi K, Toshima T, Funayama Y. Laparoscopic cholecystectomy and common bile duct exploration for cholecystocholedocholithiasis with a left-sided gallbladder: report of a case. Surg Today. 2009;39:252–255. doi: 10.1007/s00595-008-3837-0. [DOI] [PubMed] [Google Scholar]
- 24.Si-Youn R, Poong-Man J. Left-sided gallbladder with right-sided ligamentum teres hepatis: rare associated anomaly of exomphalos. J Pediatr Surg. 2008;43:1390–1395. doi: 10.1016/j.jpedsurg.2008.03.033. [DOI] [PubMed] [Google Scholar]
- 25.Kanazumi N, Fujiwara M, Sugimoto H, Fujii T, Nomoto S, Inoue S, Takeda S, Nakao A. Laparoscopic cholecystectomy for left-sided gallbladder: report of two cases. Hepatogastroenterology. 2007;54:674–676. [PubMed] [Google Scholar]
- 26.Noritomi T, Watanabe K, Yamashita Y, Kitagawa S, Oshibuchi M, Shirakusa T. Left-sided gallbladder associated with congenital hypoplasia of the left lobe of the liver: a case report and review of literature. Int Surg. 2004;89:1–5. [PubMed] [Google Scholar]
- 27.Fujita N, Shirai Y, Kawaguchi H, Tsukada K, Hatakeyama H. Left-sided gallbladder on the basis of a right-sided round ligament. Hepatogastroenterology. 1998;45:1482–1484. [PubMed] [Google Scholar]
- 28.Shimizu T, Hayashi M, Inoue Y, Komeda K, Asakuma M, Hirokawa F, Miyamoto Y, Snawder BJ, Tanaka K, Uchiyama K. Living-donor liver transplantation from donor with a left-sided gallbladder with portal vein anomaly. Transplantation. 2012;94:e60–e61. doi: 10.1097/TP.0b013e31826e5947. [DOI] [PubMed] [Google Scholar]
- 29.Alharthi S, Bernon M, Krige JE. Beware the left-sided gallbladder. S Afr J Surg. 2012;50:88–89. doi: 10.7196/sajs.1301. [DOI] [PubMed] [Google Scholar]
- 30.Hwang S, Lee SG, Park KM, Lee YJ, Ahn CS, Kim KH, Moon DB, Ha TY, Cho SH, Oh KB. Hepatectomy of living donors with a left-sided gallbladder and multiple combined anomalies for adult-to-adult living donor liver transplantation. Liver Transpl. 2004;10:141–146. doi: 10.1002/lt.20007. [DOI] [PubMed] [Google Scholar]
- 31.Gui D, Magalini S, Prete F, Sermoneta D. What’s right when the gallbladder’s left A case report. Surg Endosc. 2002;16:1637. doi: 10.1007/s00464-002-4217-2. [DOI] [PubMed] [Google Scholar]
- 32.Asonuma K, Shapiro AM, Inomata Y, Uryuhara K, Uemoto S, Tanaka K. Living related liver transplantation from donors with the left-sided gallbladder/portal vein anomaly. Transplantation. 1999;68:1610–1612. doi: 10.1097/00007890-199911270-00031. [DOI] [PubMed] [Google Scholar]