

Abstract
(1) Objective
to find longitudinal evidence of the effect of targeted peer victimization (TPV) on depressive cognitions as a function of victimization type and gender.
(2) Method
Prospective relations of physical and relational peer victimization to positive and negative self-cognitions were examined in a one-year, two-wave longitudinal study. Self-reports of cognitions and both peer nomination and self-report measures of peer victimization experiences were obtained from 478 predominantly Caucasian children and young adolescents (grades 3 through 6 at the beginning of the study) evenly split between genders.
(3) Results
(a) peer victimization predicted increases in negative cognitions and decreases in positive cognitions over time; (b) relational victimization was more consistently related to changes in depressive cognitions than was physical victimization; (c) the prospective relation between victimization and depressive cognitions was stronger for boys than for girls; and (d) when the overlap between relational and physical TPV was statistically controlled, girls experienced more relational TPV than did boys, and boys experienced more physical TPV than did girls.
(4) Conclusions
Peer victimization, particularly relational TPV, has a significant impact on children’s depressive cognitions. This relation seems particularly true for boys. Implications for future research, clinical work with victimized youth at risk for depression, and school policy to help both victims and bullies are discussed.
Keywords: Cognitions, Human Sex Differences, Peer Relations, Victimization, Bullying, Depression
The likelihood of being targeted for victimization by peers is especially high in middle childhood and early adolescence. Targeted peer victimization (TPV) is defined as “the experience among children of being a target of the aggressive behavior of other children” (Hawker & Boulton, 2000, p. 441). Although TPV has been linked to a variety of negative outcomes, the connection to depression is especially strong (e.g., Hawker & Boulton, 2000; Boivin, Hymel, & Bukowski, 1995). The reasons for this association are not clear. Various cognitive models of depression suggest that the development of a tendency to embrace negative views of self, world, others, and future and the tendency to deny more adaptive, positive views constitute cognitive diatheses for depression (Nolen-Hoeksema, Girgus, & Seligman, 1992; Hankin & Abramson, 2001; Abela & Hankin, 2009). Research supports such models in children and young adolescents (Abela, 2001; Kercher & Rapee, 2009). We contend that TPV represents one pathway to the development of such cognitive diatheses. TPV constitutes painful social feedback to victims about their social status and personal liabilities, and given that middle childhood is a time when both positive and negative self-relevant cognitions are under construction, Cole, Maxwell, Dukewich, and Yosick (2010) suggested that one mechanism underlying the TPV-depression connection involves the effect of TPV on cognitive diatheses that predispose depression (e.g., Abela, & Hankin, 2008, 2009). Differential effects of TPV on depressive cognitions may vary with the type of victimization and with the gender of the victim; however, most research supporting these relations has been cross-sectional. Consequently, the over-arching goal of the current study was to seek longitudinal evidence of the effect of TPV on depressive cognitions, as a function of TPV type and gender.
Most studies on the effect of TPV on depressive cognitions have been cross-sectional (e.g., Boulton & Smith, 1994; Callaghan & Joseph, 1995; Gibb, Abramson, & Alloy, 2004; Cole et al., 2010). As cross-sectional studies cannot control for prior levels of the dependent variable, their estimates of the TPV-cognition relation are poor proxies for the prospective relation (Cole & Maxwell, 2009). The few longitudinal studies that have been conducted have tended to ignore differences in type of victimization, neglect differences between the sexes, and/or focus on other dependent variables such as attributional style, rumination, and negative affect (e.g., Gibb & Abela, 2008; Barschia & Bussey, 2010; Dill, Vernberg, Fonagy, Twemlow, & Gamm, 2004).
Victimization has been divided into various important subtypes. We focus on two: overt/physical victimization and covert/relational victimization. Overt/physical victimization occurs when a child is controlled or physically harmed by attacks or physical threats (Crick & Bigbee, 1998). Covert/relational victimization involves behavior designed to damage peer relationships, friendships, and social acceptance, often by excluding the victim from peer activities, withdrawing friendship, or spreading rumors (Crick & Bigbee, 1998; Grotpeter & Crick, 1996; Hawker & Boulton, 2000). Historically, overt/physical victimization has received more attention than covert/relational victimization. In recent years, however, researchers have begun to realize that covert/relational forms of victimization are strongly associated with increased internalizing problems, even more so than physical victimization (Cole, Maxwell, Dukewich, & Yosick, 2010; Hunter & Boyle, 2002; Juvonen and Graham, 2001; Olweus 1995; Pepler, Craig, Yuile, & Connolly, 2004). For example, Woods, Done, and Kalsi (2009) found that victims of relational victimization reported more emotional problems and feelings of loneliness than non-victims, whereas students who experienced physical victimization did not differ from non-victims. Based on this research, we hypothesize that relational victimization will be more strongly associated with changes in depressive cognitions than physical victimization.
We focus on gender as a possible moderator of the TPV-cognition relation; however, the direction of this effect is unclear. Theory and evidence proceed in two directions. On the one hand, we know that the social worlds of boys and girls become increasingly differentiated during middle childhood. Girls become more invested in their social networks than do boys; conversely, boys become less likely to seek social support when stressed (Frydenberg & Lewis, 1993; Rose & Rudolph, 2006). Supporting this idea, Prinstein, Boergers, and Vernberg (2001) found that physical victimization was significantly associated with depressive symptoms for adolescent boys but not for adolescent girls. These differences might lead one to expect that boys will have more difficulty coping with TPV than will girls. On the other hand, studies also reveal that girls are more likely to internalize peers’ negative acts directed at them than boys are, resulting in increased loneliness and anxiety symptoms (Grills & Ollendick, 2002). These differences suggest that TPV might have greater impact on girls than boys. That said, still other evidence is inconclusive. For example, Cole et al. (2010) found that the relations between both types of victimization, self-cognitions, and depressive symptoms were the same for girls and boys. In the current study, we test gender as a moderator of the longitudinal relation of positive and negative cognitions to both types of TPV without clear a priori expectations about the direction of these effects.
Research regarding mean gender differences for TPV has also generated complex results. Although studies have established that boys are more likely to experience physical victimization than are girls, gender differences in the experience of relational victimization have been inconsistent (e.g., Crick & Grotpeter, 1995; Galen & Underwood, 1997; French, Janse, & Pidada, 2002). Smith, Rose, and Schwartz-Mette (2010) suggested that the inconsistent findings regarding relational victimization may be due to the fact that both types of TPV are highly correlated and some researchers have not controlled for overlap with physical victimization when testing the effect of gender on relational victimization. When Smith et al. (2010) controlled for statistical overlap with physical TPV, they found that girls were more likely to experience relational victimization than boys. Other studies have found similar results (e.g., Cole et al., 2010). Therefore in the current study, we hypothesize that boys will experience more physical TPV than girls do and girls will experience more relational TPV than boys do, after statistically controlling for the other type of TPV.
We focused this research on middle childhood and early adolescence for three reasons. First, rates of peer victimization are higher during these years than at any other period of human development (Pelligreni & Long, 2002). Second, during these years, a major developmental task is the construction of self-concept and self-perceived competence (Weiss & Garber, 2003; Harter, 1990). Some children negotiate this task well, developing positive self-cognitions and an optimistic world view, resilience factors that can protect against depression (Masten, Hubbard, & Scott, 1999; Cole, Martin, Powers, & Truglio, 1996). Other children have difficulty with this task, developing a strong negative cognitive style that can predispose depression (Cole, Martin, & Powers, 1997; Burt, Obradovic, Long, & Masten, 2008). Peer victimization represents a clear and undeniable source of negative, self-relevant information that has the potential to affect a child’s capacity to complete this developmental task successfully. Third, individual differences in several kinds of depressive cognitions become increasingly stable at this age (Cole et al., 2008; LaGrange et al., 2008; Hankin, 2008).
In the current study, we had three major goals. First was to test the hypotheses that TPV would predict increases in negative self-cognitions and decreases in positive self-cognitions over time. We predicted that evidence of a relation between relational TPV and depressive cognitions would be stronger than evidence of a relation between physical TPV and such cognitions. Second was to test the hypotheses that boys would experience more physical victimization than do girls, and that girls would experience more relational victimization than do boys, after controlling for the overlap between these two types of TPV. Our third goal was to test for gender differences in the strength of the relations of relational and physical TPV to positive and negative cognitions. We addressed these goals in a two-wave longitudinal study of the effects of both physical and relational TPV on various types of positive and negative self-relevant cognitions. Noting that Hawker and Boulton (2000) reported evidence of mono-method bias when TPV and the outcome variable were assessed by similar methods (e.g., self-report), we assessed TPV using two relatively dissimilar methods: peer nomination and self-report.
Method
Participants
We recruited participants from two suburban elementary schools and one middle school in central Tennessee. At Time 1, consent forms for parents and letters describing the project were distributed to 626 students in third, fourth, fifth, and sixth grades. We received permission for 421 students, 404 (96%) of whom were present on the day of data collection and gave their assent to participate. At Time 2 (one year later), 656 consent forms were sent to parents of fourth, fifth, sixth and seventh students, and 470 parents gave permission for their children to participate, of whom 414 (88%) were present on the day of data collection and gave their assent to participate. Comparisons of participants to nonparticipants on ethnicity, sex, and grade level revealed only small, nonsignificant results (ps > .20) at both time points. The total N of 478 contained two patterns of missing data: those who participated at Time 1 but not Time 2 (dropouts, 15%) and those who participated in Time 2 but not Time 1 (joiners, 13%). The primary reason for dropping out (moving out of the school district) was essentially the same as the primary reason for joining the study (moving into the school district). Comparison of these two subgroups to participants with no missing data revealed no significant differences on any variable on which the subgroups were not missing (all ps > .05). Therefore, to avoid unnecessary sampling bias and to enhance the fidelity of parameter estimation, we included all participants in the data analysis and used full information maximum likelihood statistical methods for all parameter estimations (Widaman, 2006).
At the beginning of the study, participants were evenly distributed across grades 3 through 6, and ages ranged from 8 to 14 (M = 10.9, SD = 1.2). Overall, the sample had approximately equal numbers of males and females (49.6% and 50.4%, respectively). The sample consisted of 91.0% Caucasian, 1.7% African American, 3.6% Hispanic, and 3.7% other. These rates were proportional to the ethnic distribution of the county. Family size (i.e., the number of children living at home) ranged from 1 to 9 (Mdn = 2.8). In this sample, 31% of students were on a completely free lunch program and an additional 12% were on a partially free lunch program, reflecting the fact that the school district served families that were of predominantly low to middle socio-economic status.
Measures
Peer victimization
We assessed peer victimization using both self-report and peer nomination methods. Utilization of multiple informants is crucial insofar as every informational source has its own strengths and weaknesses (De Los Reyes & Prinstein, 2004). Our self-report was a 6-item questionnaire designed to assess covert/relational and overt/physical victimization (RV-SR and PV-SR, respectively) we had used and validated in an earlier study (Cole et al., 2010). The measure expands on the items used by Kochenderfer-Ladd and Ladd (2001) to reflect a broader range of victimization experiences. Items were also reworded for somewhat older children. The question stem was “Does anyone in your class ever….” The three relational items were: (1) Tell others to stop being your friend, (2) Say you can’t play with them, and (3) Say mean things to others kids about you. The three physical items were (4) Kick you, (5) Hit you, and (6) Push you. Each item was rated on a 4-point scale (1 = never, 2 = rarely, 3 = sometimes, 4 = a lot). Despite the relatively small number of items, both subscales had acceptable internal consistency in the current study (Cronbach’s alphas were 0.86 and 0.77 for relational and physical victimization, respectively). Principle axis factor analysis with oblimin rotation revealed a 2-factor structure with primary factor loadings above 0.57 on the appropriate factors, and no cross loadings greater than 0.25. The two factors correlated 0.44 and 0.51 for Time 1 and Time 2, respectively.
Our peer nomination measure followed a format similar to that used in studies of children’s social status (e.g., Coie, Dodge, & Coppotelli, 1982). Each participant received a list of 20 names of student participants, in an order randomized for each participant. Names were primarily from the respondent’s homeroom. If there were not 20 consented participants from that roster, names were added from adjacent classrooms. Every student’s name appeared on 20 other students’ peer nomination forms. Separate forms were used to obtain peer nominations of relational and physical victimization. For example, the physical victimization item was: “Some kids get picked on or hurt by other kids at school. They might get pushed around. They might get bullied by others. They might even get beaten up. Who gets treated like this? Who gets pushed around or bullied by others?” The relational victimization item was: “Some kids get picked on by other kids at school in different ways. They might get ignored, talked about or made fun of. Other kid may say or do mean things behind their backs. They may even be left out or kicked out of groups.” Instructions ask respondents to mark all the names of classmates who fit a particular question. Scores for each student were the proportion of participant nominators who indicated that the student was either physically or relationally victimized.
Cognitve measures
Harter’s (1985) Self-Perception Profile for Children (SPPC) is a self-report inventory with 36 items reflecting developmentally appropriate specific domains (i.e., scholastic competence, social acceptance, behavioral conduct, physical attractiveness, and sports competence) plus a global self-worth scale, which we did not use. For each item, children select one of two statements to indicate whether they are more like a child who is good or a child who is not so good at a particular activity. Then they select statements indicating whether the selected statement is “sort of true” or “really true” about themselves. Responses are converted to 4-point rating scales with high scores reflecting better self-perceptions. The SPPC has a highly interpretable factor structure and all subscales have good internal consistency (Harter, 1982, 1985). In our sample, Cronbach’s alpha for the SPPC scales ranged from 0.86 to 0.89.
The Cognitive Triad Inventory for Children (CTI-C; Kaslow, Stark, Printz, Livingston, & Tsai, 1992) is a 36-item self-report questionnaire assessing children’s views of themselves (e.g., “I am a failure”), their world (e.g. “The world is a very mean place”), and their future (e.g., “Nothing is likely to work out for me”). Children indicate whether or not they have had specific thoughts using a yes/maybe/no response format, scored on 3-point scales. Scores range from 0 to 72 with higher scores indicating more negative views. Despite the word “triad” in the title, recent factor analysis of the measure reveals that a two-factor solution emerges over the course of middle childhood (LaGrange et al., 2008). One is a positive cognition factor; the other is a negative cognition factor. The measure has high internal consistency and good construct validity, correlating with measures of self-perception, self-worth, self-control, perceived contingency, and attributional style (Kaslow et al., 1992; LaGrange et al., 2008). Cronbach’s alphas for the positive and negative CTI-C scales were from 0.90 and 0.91, respectively.
The Children’s Automatic Thoughts Scale (CATS; Schniering & Rapee, 2002) is a self-report questionnaire assessing negative cognitions in young people. The questionnaire asks children to rate the frequency with which they have had 56 different negative thoughts in the previous week. Ratings are made on 5-point scales, ranging from 1=not at all to 5=all the time. The CATS yields scores on four subscales: Physical Threat (e.g. “I’m going to get hurt”), Social Threat (e.g., “I’m afraid I will make a fool of myself”), Personal Failure (e.g., “It’s my fault that things have gone wrong”), and Hostility (e.g., “I won’t let anyone get away with picking on me”). Test-retest reliability is 0.79 at 1 month and 0.76 at 3 months (Schniering & Rapee, 2002). In the current sample, Cronbach’s alphas were 0.86 to 0.94 at Time 1 and Time 2, respectively.
Procedures
Prior to data collection, informed-consent statements were distributed to all children in each participating classroom. We offered a $100 donation to each classroom if 90% of children returned consent forms signed by a parent or guardian, either granting or denying permission for their child’s participation. During regular school hours, psychology graduate students gathered consented students into small groups and administered the questionnaires, reading the questionnaires aloud but allowing participant to answer the questions on their own forms. Research assistants circulated among students to answer questions before, during, and after questionnaire administration. At the end of the survey, students were given snacks and a decorated pencil for their participation. The entire procedure was repeated one year later.
Results
Preliminary Analyses
Table 1 contains descriptive statistics and correlations for all study variables. Means and standard deviations were similar to those reported in other studies of non-referred school-based samples (LaGrange et al., 2008; Muris et al., 2003; Schniering & Rapee, 2002).i In general, within-time and within-measure correlations tended to be larger than their cross-time counterparts, although many cross-wave correlations were both significant and large. Before proceeding with the primary analyses, we note that sex is coded male = 0 and female = 1. Therefore positive correlations with sex imply that being male is associated with greater likelihood of being victimized physically (according to self-reports and peer nominations) and that being female is associated with greater likelihood of being victimized relationally (according to self-reports).
Table 1.
Correlations, Means, and Standard Deviations
| Measure | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | 13. | 14. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Physical TPV (SR) | 1.00 | |||||||||||||
| 2. Relational TPV (SR) | 0.37 | 1.00 | ||||||||||||
| 3. Physical TPV (PN) | 0.29 | 0.26 | 1.00 | |||||||||||
| 4. Relational TPV (PN) | 0.26 | 0.31 | 0.59 | 1.00 | ||||||||||
| 5. Sex (female) | -0.17 | 0.22 | -0.09 | 0.04 | 1.00 | |||||||||
| 6. CATS Physical T1 | 0.38 | 0.60 | 0.26 | 0.30 | 0.18 | 1.00 | ||||||||
| 7. CATS Social T1 | 0.40 | 0.67 | 0.26 | 0.31 | 0.21 | 0.79 | 1.00 | |||||||
| 8. CATS Hostility T1 | 0.38 | 0.48 | 0.24 | 0.22 | -0.06 | 0.61 | 0.61 | 1.00 | ||||||
| 9. CATS Personal Failure T1 | 0.36 | 0.57 | 0.28 | 0.28 | 0.13 | 0.82 | 0.81 | 0.61 | 1.00 | |||||
| 10. CTI Positive T1 | 0.29 | 0.50 | 0.32 | 0.26 | 0.12 | 0.56 | 0.61 | 0.45 | 0.68 | 1.00 | ||||
| 11. CTI Negative T1 | 0.34 | 0.53 | 0.32 | 0.31 | 0.06 | 0.65 | 0.68 | 0.52 | 0.76 | 0.74 | 1.00 | |||
| 12. SPPC Academic T1 | -0.18 | -0.33 | -0.18 | -0.17 | -0.08 | -0.49 | -0.49 | -0.38 | -0.49 | -0.55 | -0.55 | 1.00 | ||
| 13. SPPC Appearance T1 | -0.21 | -0.32 | -0.19 | -0.18 | -0.07 | -0.43 | -0.54 | -0.29 | -0.51 | -0.50 | -0.47 | 0.49 | 1.00 | |
| 14. SPPC Behavior T1 | -0.35 | -0.33 | -0.20 | -0.27 | 0.09 | -0.44 | -0.37 | -0.47 | -0.43 | -0.47 | -0.41 | 0.49 | 0.36 | 1.00 |
| 15. SPPC Social T1 | -0.23 | -0.43 | -0.30 | -0.29 | -0.08 | -0.45 | -0.60 | -0.30 | -0.53 | -0.56 | -0.58 | 0.51 | 0.56 | 0.33 |
| 16. SPPC Sport T1 | -0.13 | -0.26 | -0.14 | -0.14 | -0.22 | -0.31 | -0.40 | -0.17 | -0.35 | -0.38 | -0.34 | 0.39 | 0.49 | 0.13 |
| 17. CATS Physical T2 | 0.21 | 0.27 | 0.22 | 0.30 | 0.09 | 0.51 | 0.42 | 0.24 | 0.47 | 0.29 | 0.39 | -0.31 | -0.34 | -0.31 |
| 18. CATS Social T2 | 0.16 | 0.35 | 0.26 | 0.31 | 0.09 | 0.29 | 0.42 | 0.17 | 0.31 | 0.27 | 0.29 | -0.22 | -0.29 | -0.21 |
| 19. CATS Hostility T2 | 0.13 | 0.16 | 0.16 | 0.20 | -0.14 | 0.17 | 0.19 | 0.39 | 0.18 | 0.17 | 0.19 | -0.20 | -0.20 | -0.25 |
| 20. CATS Personal Failure T2 | 0.12 | 0.27 | 0.21 | 0.25 | 0.10 | 0.38 | 0.33 | 0.18 | 0.42 | 0.29 | 0.32 | -0.25 | -0.30 | -0.25 |
| 21. CTI Positive T2 | 0.15 | 0.26 | 0.14 | 0.22 | 0.04 | 0.40 | 0.34 | 0.25 | 0.44 | 0.31 | 0.45 | -0.35 | -0.30 | -0.27 |
| 22. CTI Negative T2 | 0.15 | 0.28 | 0.19 | 0.18 | 0.04 | 0.37 | 0.37 | 0.31 | 0.43 | 0.44 | 0.46 | -0.37 | -0.28 | -0.33 |
| 23. SPPC Academic T2 | -0.11 | -0.19 | -0.17 | -0.17 | -0.03 | -0.34 | -0.34 | -0.31 | -0.35 | -0.31 | -0.33 | 0.57 | 0.34 | 0.39 |
| 24. SPPC Appearance T2 | 0.01 | -0.19 | -0.12 | -0.15 | -0.13 | -0.33 | -0.37 | -0.15 | -0.36 | -0.31 | -0.41 | 0.37 | 0.62 | 0.31 |
| 25. SPPC Behavior T2 | -0.12 | -0.19 | -0.22 | -0.14 | 0.13 | -0.25 | -0.20 | -0.29 | -0.27 | -0.28 | -0.38 | 0.32 | 0.19 | 0.54 |
| 26. SPPC Social T2 | -0.15 | -0.26 | -0.19 | -0.26 | -0.01 | -0.29 | -0.32 | -0.12 | -0.30 | -0.33 | -0.36 | 0.23 | 0.38 | 0.17 |
| 27. SPPC Sport T2 | -0.01 | -0.11 | -0.14 | -0.11 | -0.13 | -0.19 | -0.25 | -0.12 | -0.23 | -0.23 | -0.28 | 0.21 | 0.42 | 0.13 |
| Mean | 4.63 | 5.91 | 0.06 | 0.06 | 0.51 | 16.92 | 11.77 | 21.60 | 15.16 | 26.53 | 25.36 | 11.99 | 12.26 | 13.85 |
| SD | 2.19 | 2.54 | 0.13 | 0.12 | 0.50 | 8.17 | 6.13 | 8.47 | 8.34 | 6.90 | 6.037 | 4.66 | 5.15 | 4.10 |
| Measures | 15. | 16. | 17. | 18. | 19. | 20. | 21. | 22. | 23. | 24. | 25. | 26. | 27. |
|
| |||||||||||||
| 15. SPPC Social T1 | 1.00 | ||||||||||||
| 16. SPPC Sport T1 | 0.48 | 1.00 | |||||||||||
| 17. CATS Physical T2 | -0.34 | -0.30 | 1.00 | ||||||||||
| 18. CATS Social T2 | -0.47 | -0.37 | 0.70 | 1.00 | |||||||||
| 19. CATS Hostility T2 | -0.23 | -0.20 | 0.58 | 0.59 | 1.00 | ||||||||
| 20. CATS Personal Failure T2 | -0.37 | -0.30 | 0.79 | 0.80 | 0.55 | 1.00 | |||||||
| 21. CTI Positive T2 | -0.40 | -0.30 | 0.63 | 0.66 | 0.53 | 0.77 | 1.00 | ||||||
| 22. CTI Negative T2 | -0.39 | -0.35 | 0.48 | 0.59 | 0.42 | 0.66 | 0.74 | 1.00 | |||||
| 23. SPPC Academic T2 | 0.33 | 0.29 | -0.37 | -0.41 | -0.37 | -0.42 | -0.52 | -0.58 | 1.00 | ||||
| 24. SPPC Appearance T2 | 0.42 | 0.42 | -0.39 | -0.51 | -0.31 | -0.48 | -0.53 | -0.58 | 0.45 | 1.00 | |||
| 25. SPPC Behavior T2 | 0.27 | 0.16 | -0.28 | -0.26 | -0.38 | -0.31 | -0.45 | -0.49 | 0.54 | 0.34 | 1.00 | ||
| 26. SPPC Social T2 | 0.57 | 0.47 | -0.44 | -0.60 | -0.34 | -0.55 | -0.58 | -0.61 | 0.45 | 0.52 | 0.30 | 1.00 | |
| 27. SPPC Sport T2 | 0.36 | 0.66 | -0.32 | -0.39 | -0.23 | -0.38 | -0.42 | -0.51 | 0.50 | 0.47 | 0.33 | 0.54 | 1.00 |
| Mean | 11.77 | 11.70 | 15.10 | 17.65 | 21.79 | 15.00 | 25.00 | 26.00 | 11.77 | 11.47 | 13.43 | 12.25 | 11.55 |
| SD | 5.13 | 4.75 | 6.88 | 9.41 | 9.18 | 8.43 | 6.63 | 7.29 | 4.900 | 5.78 | 4.59 | 5.24 | 5.21 |
Note. SR = Self-report; PN = Peer-nominated, CATS = Children’s Automatic Thoughts Scale; CTI = Cognitive Triad Inventory for Children; SPPC= Self-perception Profile for Children; p < .05; p < .01. The SPPC is scaled in the opposite direction of the CATS and CTI. For r > .08, p < .05; when r > .11, p < .01; when r > .14, p < .001.
Data Analysis Overview
We addressed 2 of our goals (goals 1 and 3) with a series of multiple regression analyses in which one of 11 cognitive subscales served as the dependent variable (i.e., 4 CATS subscales, 2 CTI subscales, and 5 SPPC subscales). All 11 variables contributed statistically significant support to at least one of these goals. We addressed the remaining goal (goal 2) with a series of regressions in which one of 4 measures of victimization served as the dependent variable. All 4 dependent variables contributed significantly to this goal.ii
Goal 1
The first half of goal 1 was to test the hypothesis that TPV predicts increases in negative cognitions and decreases in positive cognitions over time. To test this hypothesis, we ran a family of multiple regression models. Each cognitive variable at Time 2 was regressed onto the Time 1 measure of the dependent variable, gender, and Time 1 measures of physical and relational victimization. Nine of these analyses yielded significant results (see Table 2). Either self-reported or peer-nominated Relational TPV at Time 1 predicted increases in Time 2 negative cognitions as assessed by all four subscales of the CATS and the negative cognitions subscale of the CTI, and predicted decreases in positive cognitions as assessed by the physical appearance and social acceptance subscales of the SPPC. Peer-nominated Physical TPV at Time 1 predicted increases in Time 2 scores on the negative cognitions subscale of the CTI and decreases in scores on the behavioral conduct subscale of the SPPC.
Table 2.
Relations between TPV and Negative and Positive Self-Cognitions
| Predictor | Unst. B | SE(B) | b | t(474) | p |
|---|---|---|---|---|---|
| DV = CATS Physical: Feeling Physically Threatened Time 2 | |||||
| CATS Physical Time 1 | 0.423 | 0.046 | 0.51 | 9.126 | < .001 |
| Sex | -0.219 | 0.809 | -0.016 | -0.271 | 0.787 |
| Physical TPV (PN) | -0.316 | 0.424 | -0.046 | -0.745 | 0.456 |
| Relational TPV (PN) | 1.243 | 0.411 | 0.18 | 3.023 | 0.003 |
|
| |||||
| DV = CATS Social: Feeling Socially Threatened Time 2 | |||||
| CATS Social Time 1 | 0.344 | 0.085 | 0.335 | 4.041 | < .001 |
| Sex | -1.095 | 1.221 | -0.058 | -0.897 | 0.37 |
| Physical TPV (SR) | 0.026 | 0.299 | 0.006 | 0.086 | 0.932 |
| Relational TPV (SR) | 0.607 | 0.307 | 0.165 | 1.976 | 0.048 |
|
| |||||
| DV = CATS Social: Feeling Socially Threatened Time 2 | |||||
| CATS Social Time 1 | 0.383 | 0.063 | 0.376 | 6.054 | < .001 |
| Sex | 0.367 | 1.176 | 0.02 | 0.312 | 0.755 |
| Physical TPV (PN) | 0.827 | 0.591 | 0.088 | 1.4 | 0.162 |
| Relational TPV (PN) | 1.32 | 0.585 | 0.14 | 2.258 | 0.024 |
|
| |||||
| DV = CATS Hostility: Feeling Hostility Toward Others Time 2 | |||||
| CATS Hostility Time 1 | 0.384 | 0.064 | 0.358 | 5.976 | < .001 |
| Sex | -3.715 | 1.111 | -0.206 | -3.344 | < .001 |
| Physical TPV (PN) | -0.716 | 0.586 | -0.078 | -1.221 | 0.222 |
| Relational TPV (PN) | 1.725 | 0.571 | 0.188 | 3.023 | 0.003 |
|
| |||||
| DV = CATS Personal Failure: Self-perceptions of Failure Time 2 | |||||
| CATS Personal Failure Time 1 | 0.412 | 0.06 | 0.418 | 6.9 | < .001 |
| Sex | 0.558 | 1.039 | 0.033 | 0.537 | 0.591 |
| Physical TPV (PN) | 0.06 | 0.542 | 0.007 | 0.111 | 0.911 |
| Relational TPV (PN) | 1.169 | 0.517 | 0.139 | 2.262 | 0.024 |
|
| |||||
| DV = CTI Negative: Negative View of Self, World, and Future Time 2 | |||||
| CTI Negative Time 1 | 0.502 | 0.061 | 0.481 | 8.19 | < .001 |
| Sex | -0.261 | 0.883 | -0.018 | -0.295 | 0.768 |
| Physical TPV (PN) | -0.946 | 0.468 | -0.129 | -2.019 | 0.043 |
| Relational TPV (PN) | 1.142 | 0.451 | 0.156 | 2.534 | 0.011 |
|
| |||||
| DV = SPPC Appearance: Self-perceived Physical Attractiveness Time 2 | |||||
| SPPC Appearance Time 1 | 0.709 | 0.056 | 0.637 | 12.689 | < .001 |
| Sex | -0.416 | 0.646 | -0.036 | -0.644 | 0.52 |
| Physical TPV (SR) | -0.049 | 0.14 | -0.021 | -0.349 | 0.727 |
| Relational TPV (SR) | 0.319 | 0.156 | 0.121 | 2.047 | 0.041 |
|
| |||||
| DV = SPPC Behavior: Self-perceived Behavioral Competence Time 2 | |||||
| SPPC Behavior Time 1 | 0.595 | 0.058 | 0.538 | 10.284 | < .001 |
| Sex | 0.492 | 0.523 | 0.054 | 0.941 | 0.347 |
| Physical TPV (PN) | -0.821 | 0.276 | -0.178 | -2.97 | 0.003 |
| Relational TPV (PN) | 0.37 | 0.278 | 0.08 | 1.334 | 0.182 |
|
| |||||
| DV = SPPC Social: Self-perceived Social Competence Time 2 | |||||
| SPPC Social Time 1 | 0.561 | 0.054 | 0.553 | 10.359 | < .001 |
| Sex | -0.123 | 0.596 | -0.012 | -0.206 | 0.837 |
| Physical TPV (PN) | 0.255 | 0.321 | 0.049 | 0.795 | 0.427 |
| Relational TPV (PN) | -0.62 | 0.312 | -0.118 | -1.991 | 0.047 |
The second half of goal 1 was to test the hypothesis that Relational TPV will predict depressive cognitions even after controlling for Physical TPV, but Physical TPV will not predict such cognitions over-and-above Relational TPV. This hypothesis was partially supported. Out of the nine significant regressions described above and reported in Table 2, seven showed that Relational TPV was significant and Physical TPV was not, one showed that Physical TPV was significant and Relational TPV was not, and one showed that both Relational and Physical TPV were significant predictors.
Goal 2
Our second goal was to test the hypotheses that girls experience more relational victimization than do boys and that boys experience more physical victimization than do girls. To test these hypotheses, we ran a series of regression models. Each measure of Physical TPV was regressed onto gender and a comparable measure of Relational TPV. Likewise, each measure of Relational TPV was regressed onto gender and a comparable measure of Physical TPV. Gender was coded as 0 for boys and 1 for girls, meaning that positive beta weights for gender indicate that girls experienced more TPV than boys. Results indicated that (a) when self-reported Physical TPV was statistically controlled, girls reported more Relational TPV than did boys did (β = 0.29, p < .001), (b) when peer-nominated Physical TPV was controlled, girls had higher Relational TPV scores than did boys (β = 0.11, p = .001), (c) when self-reported Relational TPV was controlled, boys reported more physical TPV than did girls (β = -0.26, p < .001), and (d) when peer-reported Relational TPV was controlled, boys had higher physical victimization scores than did girls (β = -0.13, p < .001). As depicted in Figure 1, these adjusted mean differences supported our hypotheses.
Figure 1.
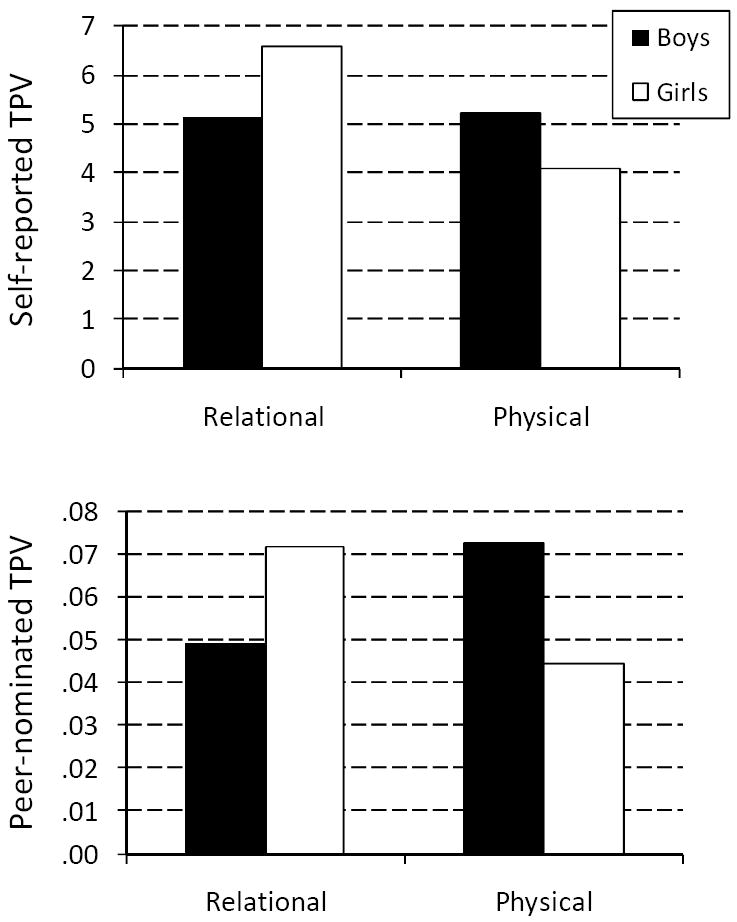
Adjusted means for relational and physical victimization broken down by gender.
Goal 3
Our third goal was to test for gender differences in the relations of TPV to positive and negative cognitions. Toward this goal, we conducted a series of multiple regression analyses. In each analysis, a cognition measure at Time 2 was regressed onto that measure at Time 1, Gender, a measure of TPV, and the TPV × Gender interaction. When the TPV × Gender interaction was significant, we conducted simple slope analyses to determine if the relation between TPV and cognitions was significant for each gender. As shown in Table 3, 14 significant interactions emerged, all with highly consistent interpretations.
Table 3.
Gender Differences in the Relations between TPV and Self-Cognitions
| Predictor | Unst. B | SE(B) | b | t(474) | p |
|---|---|---|---|---|---|
| DV = CATS Physical: Feeling Physically Threatened Time 2 | |||||
| CATS Physical Time 1 | 0.44 | 0.50 | 0.52 | 8.79 | < .001 |
| Sex | -0.01 | 0.68 | 0.00 | -0.01 | 0.989 |
| Physical TPV (SR) | 1.25 | 0.53 | 0.17 | 2.33 | 0.020 |
| Sex × Physical TPV (SR) | -1.74 | 0.79 | -0.15 | -2.20 | 0.028 |
|
| |||||
| DV = CATS Physical: Feeling Physically Threatened Time 2 | |||||
| CATS Physical Time 1 | 0.46 | 0.06 | 0.49 | 8.18 | < .001 |
| Sex | -2.21 | 2.80 | -0.04 | -0.79 | 0.431 |
| Physical TPV (PN) | 7.10 | 1.89 | 0.24 | 3.76 | < .001 |
| Sex × Physical TPV (PN) | -11.18 | 3.14 | -0.23 | -3.56 | < .001 |
|
| |||||
| DV = CATS Physical: Feeling Physically Threatened Time 2 | |||||
| CATS Physical Time 1 | 0.45 | 0.05 | 0.54 | 9.93 | < .001 |
| Sex | -0.23 | 0.63 | -0.02 | -0.37 | 0.715 |
| Relational TPV (PN) | 1.71 | 0.48 | 0.25 | 3.59 | < .001 |
| Sex × Relational TPV (PN) | -1.64 | 0.68 | -0.17 | -2.40 | 0.016 |
|
| |||||
| DV = CATS Social: Feeling Socially Threatened Time 2 | |||||
| CATS Social Time 1 | 0.44 | 0.06 | 0.44 | 7.30 | < .001 |
| Sex | -0.10 | 0.91 | -0.01 | -0.11 | 0.915 |
| Physical TPV (PN) | 2.72 | 0.60 | 0.29 | 4.52 | < .001 |
| Sex × Physical TPV (PN) | -3.24 | 0.98 | -0.21 | -3.30 | < .001 |
|
| |||||
| DV = CATS Social: Feeling Socially Threatened Time 2 | |||||
| CATS Social Time 1 | 0.37 | 0.08 | 0.35 | 4.49 | < .001 |
| Sex | -0.99 | 0.92 | -0.05 | -1.08 | 0.282 |
| Relational TPV (SR) | 3.69 | 1.07 | 0.37 | 3.46 | < .001 |
| Sex × Relational TPV (SR) | -3.35 | 1.18 | -0.26 | -2.85 | 0.004 |
|
| |||||
| DV = CATS Hostility: Feeling Hostility Toward Others Time 2 | |||||
| CATS Hostility Time 1 | 0.44 | 0.06 | 0.41 | 6.83 | < .001 |
| Sex | -2.13 | 0.86 | -0.12 | -2.46 | 0.014 |
| Physical TPV (PN) | 1.38 | 0.60 | 0.15 | 2.30 | 0.022 |
| Sex × Physical TPV (PN) | -2.16 | 0.99 | -0.14 | -2.18 | 0.029 |
|
| |||||
| DV = CATS Hostility: Feeling Hostility Toward Others Time 2 | |||||
| CATS Hostility Time 1 | 0.39 | 0.08 | 0.35 | 5.21 | < .001 |
| Sex | -2.62 | 0.94 | -0.14 | -2.80 | 0.005 |
| Relational TPV (SR) | 2.13 | 1.05 | 0.22 | 2.04 | 0.041 |
| Sex × Relational TPV (SR) | -2.33 | 1.19 | -0.18 | -1.96 | 0.05 |
|
| |||||
| DV = CATS Hostility: Feeling Hostility Toward Others Time 2 | |||||
| CATS Hostility Time 1 | 0.43 | 0.06 | 0.40 | 6.76 | < .001 |
| Sex | -2.12 | 0.86 | -0.12 | -2.48 | 0.013 |
| Relational TPV (PN) | 2.07 | 0.67 | 0.23 | 3.11 | 0.002 |
| Sex × Relational TPV (PN) | -1.94 | 0.96 | -0.15 | -2.03 | 0.042 |
|
| |||||
| DV = CATS Personal Failure: Self-perceptions of Failure Time 2 | |||||
| CATS Personal Failure Time 1 | 0.45 | 0.06 | 0.47 | 7.58 | < .001 |
| Sex | 0.40 | 0.81 | 0.02 | 0.49 | 0.624 |
| Physical TPV (PN) | 1.44 | 0.55 | 0.17 | 2.65 | 0.008 |
| Sex × Physical TPV (PN) | -2.27 | 0.91 | -0.16 | -2.50 | 0.013 |
|
| |||||
| DV = CATS Personal Failure: Self-perceptions of Failure Time 2 | |||||
| CATS Personal Failure Time 1 | 0.41 | 0.07 | 0.40 | 5.71 | < .001 |
| Sex | 0.03 | 0.83 | 0.00 | 0.04 | 0.972 |
| Relational TPV (SR) | 2.58 | 0.93 | 0.29 | 2.77 | 0.006 |
| Sex × Relational TPV (SR) | -3.06 | 1.06 | -0.26 | -2.88 | 0.004 |
|
| |||||
| DV = SPPC Academic: Self-perceived Academic Competence Time 2 | |||||
| SPPC Academic Time 1 | 0.61 | 0.05 | 0.59 | 11.91 | < .001 |
| Sex | 0.10 | 0.44 | 0.01 | 0.23 | 0.822 |
| Physical TPV (PN) | -0.84 | 0.30 | -0.17 | -2.78 | 0.005 |
| Sex × Physical TPV (PN) | 1.41 | 0.49 | 0.17 | 2.89 | 0.004 |
|
| |||||
| DV = SPPC Social: Self-perceived Social Competence Time 2 | |||||
| SPPC Social Time 1 | 0.58 | 0.05 | 0.57 | 11.20 | < .001 |
| Sex | 0.10 | 0.49 | 0.01 | 0.21 | 0.831 |
| Physical TPV (SR) | -0.90 | 0.39 | -0.16 | -2.34 | 0.019 |
| Sex × Physical TPV (SR) | 1.47 | 0.58 | 0.16 | 2.52 | 0.012 |
|
| |||||
| DV = SPPC Social: Self-perceived Social Competence Time 2 | |||||
| SPPC Social Time 1 | 0.60 | 0.06 | 0.58 | 10.52 | <.001 |
| Sex | 0.26 | 0.49 | 0.03 | 0.53 | 0.600 |
| Relational TPV (SR) | -0.96 | 0.52 | -0.17 | -1.84 | 0.066 |
| TPV × Sex | 1.51 | 0.61 | 0.21 | 2.46 | 0.014 |
|
| |||||
| DV = SPPC Sports: Self-perceived Athletic Competence Time 2 | |||||
| SPPC Sport Time 1 | 0.73 | 0.05 | 0.68 | 14.62 | < .001 |
| Sex | 0.19 | 0.46 | 0.02 | 0.40 | 0.688 |
| Physical TPV (PN) | -0.41 | 0.31 | -0.08 | -1.35 | 0.178 |
| Sex × Physical TPV (PN) | 1.12 | 0.50 | 0.13 | 2.27 | 0.023 |
Eight of these involved an interaction between Gender and Physical TPV. Depicted in Figure 2, Physical TPV was more strongly (and positively) related to negative cognitions for boys than for girls, on all subscales of the CATS. No significant Gender by Physical TPV interactions emerged for the CTI subscales. Also depicted in Figure 2, Physical TPV was more strongly (and negatively) related to positive cognitions for boys than for girls on the social acceptance, academic competence, and sports competence subscales of the SPPC. Simple slope analyses revealed that the relation was much more likely to be significant for boys than for girls (see the p-values associated with each of the Figure 2 regression lines).
Figure 2.
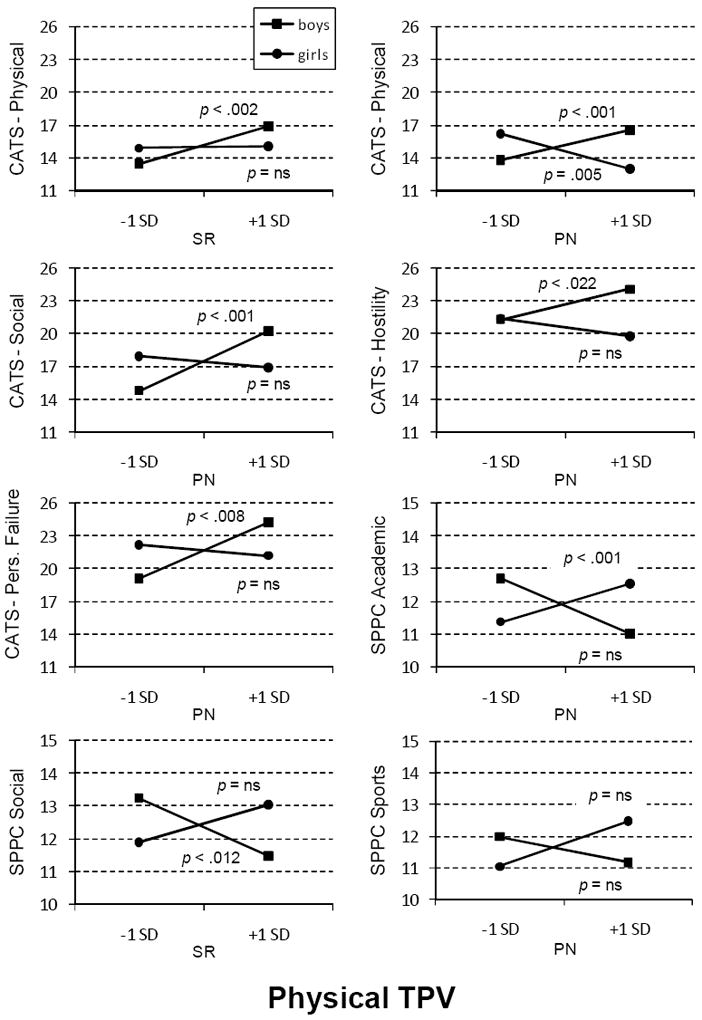
Gender differences in the relation between physical TPV and multiple measures of self-cognition (Note: PN = peer nomination; SR = self-report).
The other six significant tests involved interactions between Gender and Relational TPV. Depicted in Figure 3, Relational TPV was more strongly (and positively) related to negative cognitions for boys than for girls on all subscales of the CATS. No significant Gender by Relational TPV interactions emerged for the CTI subscales. Also depicted in Figure 3, Relational TPV was more strongly (and negatively) related to scores on the social acceptance subscale of the SPPC for boys than for girls. Simple slope analyses revealed that the relation was typically significant for boys but not for girls (see the p-values associated with each of the Figure 3 regression lines).
Figure 3.
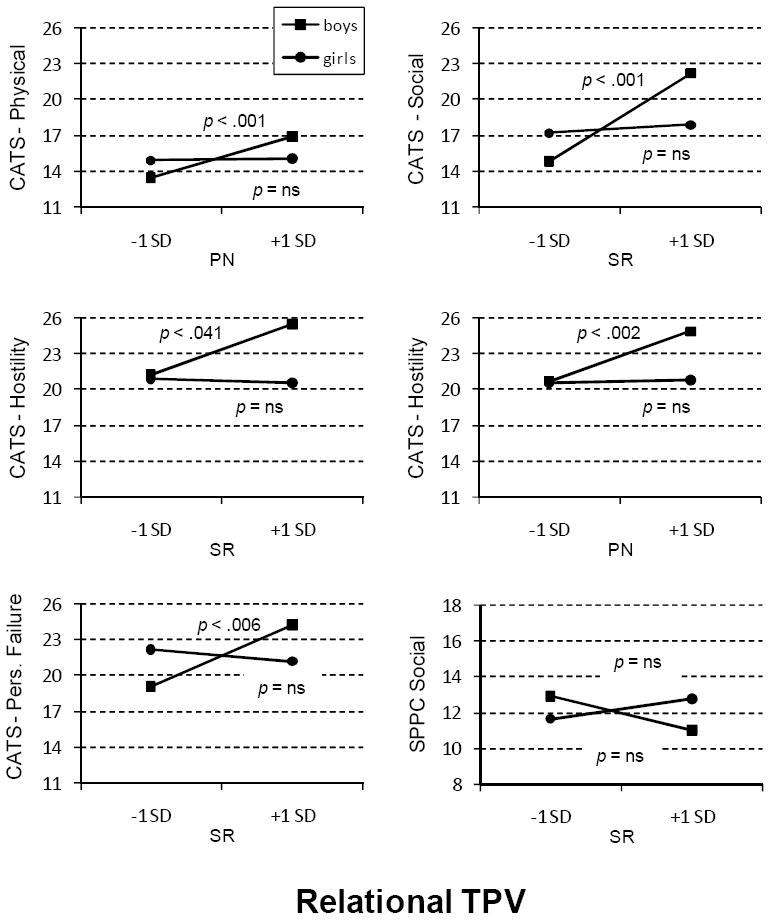
Gender differences in the relation between relational TPV and self-cognitions (Note: PN = peer nomination; SR = self-report).
Discussion
Four major findings emerged from the current study. First, in a sample of children and adolescents, TPV predicted increases in negative cognitions and decreases in positive cognitions over a one-year time interval. Second, after controlling for the overlap between relational and physical TPV, evidence supporting the prospective relation of relational TPV to negative cognitions was stronger than evidence supporting the predictive utility of physical TPV. Third, the prospective relation between TPV and depressive cognitions was stronger for boys than for girls. Fourth, when the overlap between relational and physical TPV was statistically controlled, girls experienced more relational TPV than did boys, and boys experienced more physical TPV than did girls. Each of these results is elaborated below.
First, the data supported our hypothesis that TPV would predict increases in negative cognitions and decreases in positive cognitions during middle childhood and early adolescence over the course of one calendar year. Pooling across analyses of both self-report and peer-nomination measures of victimization, a wide variety of cognitions were affected, including participants’ perceptions of themselves as a failure, physically unattractive, socially incompetent, and angry. TPV also affected perceptions of the world as a physically and socially threatening place. Compared to non-victimized children, children who experienced TPV generally developed more negative views of themselves, their worlds, and their futures over time. Although both positive and negative cognitions were affected by TPV, results were more often significant for negative than for positive self-cognitions.
These findings provide support for several theoretical positions. Symbolic interactionism and the “looking glass” model suggest self-perceptions derive at least in part from our perceptions of others’ views of us (Cooley, 1902; Mead, 1913). Support for such models has tended to be stronger among children and adolescents than adults (Cole, 1991a; Shrauger & Schoeneman, 1979), a finding commensurate with the idea that a major developmental task of middle childhood is the development of self-concept and self-perceived competence (Cole, Jacquez, & Maschman, 2001; Cole, Maxwell, & Martin, 1997; Garber, 1984; Harter, 2003). The key to the viability of such models is identifying key mechanisms whereby children become aware of others’ perceptions of themselves. The current study supports the idea that peer victimization experiences represent one such mechanism. The current study also provides an initial stage of support for our speculation that increases in negative cognitions and decreases in positive cognitions constitute vehicles through which peer victimization can lead to depression in children and adolescents (Cole et al., 2010). We hasten to add, however, that mediation is a causal chain. The current study supports the first link of this chain, connecting TPV to depressive cognitions. Other studies support the second link, connecting such cognitions to depression in children (Berg & Klinger, 2009; Uhrlass, Schofield, Coles, & Gibb, 2009; Cole, 1990). An important avenue for future research will be longitudinal meditational analyses assessing the degree to which changes in positive and negative cognitions explain the longitudinal connection between TPV and depression in children and adolescents.
In a closely related vein, our second finding was that relational TPV was more often associated with these negative cognitive outcomes than was physical TPV, even after controlling for the common co-occurrence of these two forms of victimization. This result expands upon our previous cross-sectional findings (Cole et al., 2010), suggesting that relational TPV is the more harmful form of victimization at least insofar as children’s cognitive and emotional well-being are concerned. The current findings also complement and expand upon the work of John Abela. Gibb and Abela (2008) examined the impact of emotional abuse from caregivers and relational TPV on inferential styles in middle childhood. Emotional abuse can be viewed as relational victimization at the hands of parents. Therefore, Gibb and Abela’s findings indicate that relational victimization from either parents or peers has a significant impact on depressogenic cognitions. The current study assessed both physical and relational peer victimization, providing additional support for the harmful impact of relational victimization while also indicating that relational victimization has a stronger connection to depressive cognitions than does physical. Several explanations for this finding are possible: (a) Relational victimization may convey negative information of a more personalized nature than does physical victimization; (b) Relational TPV may be harder to counteract, as reputational bias is difficult to reverse; (c) Relational TPV is often more difficult to defend against, as the victim may not even be aware of the perpetrator’s identity (Mynard & Joseph, 2000). Understanding the reasons why relational victimization appears to be more toxic than physical victimization is an important area for future research.
Third, we found that the prospective relation of TPV to positive and negative cognitions was stronger for boys than for girls. Indeed, many of our analyses suggested that the detrimental effect of TPV on several types of cognition was significant for boys and not for girls. Our findings are commensurate with Prinstein et al.’s (2001) results suggesting that victimization was more strongly associated with depressive symptoms for boys than for girls. Although the current study did not include measures of variables that might account for this effect, we hypothesize that the difference may be due to developmental differences in the social worlds of boys and girls. As boys enter into middle childhood, they become less likely than girls to turn to peers, teachers, or parents for social support (e.g., Frydenberg & Lewis, 1993), making TPV particularly damaging at this time. Boys who seek help for such problems may even be perceived as weak (by both peers and adults), potentially exacerbating the effect of victimization on self-perceptions. We want to note, however, that large individual differences exist within (as well as between) the genders, paving the way for the examination of social support as a possible mediator.
Fourth, we found differences in the relative degree to which boys and girls were targeted by peers for relational versus physical victimization. As we predicted, self-report and peer nomination measures revealed that girls experience more relational victimization than do boys, and that boys experience more physical victimization than do girls, at least when the overlap between these types of victimization is statistically controlled. Gender differences in the perpetration of relational and physical aggression have been well documented (Crick & Grotpeter, 1995), but gender differences in the receipt of victimization have been less consistent. Following the recommendation of Smith et al. (2010) and controlling for one type of TPV while testing for gender differences in the other helped to clarify the issue. Combining this result with the previous finding leads to the interesting conclusion that although girls experience more relational TPV than do boys, boys are more adversely affected by relational TPV than are girls.
Implications for Research, Policy, and Practice
Results of the current study have several important clinical implications. First, finding that relational TPV increases the strength of negative cognitions, coupled with the knowledge that negative cognitions increase risk for depression, suggests that victims of relational TPV are at increased risk for depression. Teachers, school officials, and parents should not just focus on aggressors, but also realize that for every instance of peer victimization, there is a victim who warrants intervention as well. Victims of physical victimization reported more misbehavior (i.e., lower levels of behavioral competence), suggesting that they might retaliate against aggressors or be involved in physical altercations. Clearly, victims may need support from adults in order to prevent maladaptive responses to victimization.
Second, our results suggest that negative cognitions may be more easily affected by peer victimization than are positive cognitions. This finding suggests a point of entry for cognitive behavioral therapists working with victimized youths. More specifically, victimized youths may retain some domains of positive cognition that can be called upon during intervention efforts to prevent the emergence of depressive symptoms. Therapists for victimized youth could adapt current evidenced-based treatments, such as cognitive-behavioral therapy, that have been shown to help depressed children and adolescents (e.g., Weersing & Brent, 2010). For example, therapists could reinforce the content of retained positive cognitions and help youths find pleasurable activities in their domains of competency. In addition, therapists should target negative cognitions that result from victimization experiences and help youths develop coping strategies and problem solving skills that could help prevent or mitigate future instances of TPV.
Third, the fact that relational victimization appears to be more damaging than physical victimization is surprising, given that the very idea of relational aggression emerged only 16 years ago (Crick, 1995). Policy implications clearly emerge. Although many schools have anti-bullying programs, most of these focus on physical victimization. These programs are an important step in the right direction; however, they should be expanded to include relational victimization as well. School-based social skills training programs, such as the Social Skills Group Intervention (DeRosier, 2002), the Steps to Respect Program (Frey, Hirschstein, Edstrom, & Snell, 2009), and the Olweus Bullying Prevention Program (Olweus et al., 2007), appear to have positive effects on both perpetrators and victims. Physical victimization prevention programs focus on nonviolent conflict resolution and adaptive social skills, goals that are not as applicable to relational victimization. Newer programs targeting relational victimization, such as the Creating a Safe School (CASS) Intervention, are currently being studied (Nixon & Werner, 2010). CASS focuses on raising awareness and increasing knowledge about relational victimization, building empathy, and challenging normative beliefs about relational aggression.
A comprehensive program addressing both physical and relational victimization can combine the most successful aspects of these separate programs to address the two major forms of victimization simultaneously. Such a program should strive to create an environment where victims of physical and relational aggression receive support, and perpetrators receive disapproval for their actions as well as guidance for changing their behaviors. Effective interventions that address both relational and physical victimization would likely be well received by school administrators.
Future Directions
Shortcomings of the study suggest avenues for future research. One concern is the fact that we did not obtain information about the aggressors. Victims who are also perpetrators may be very different from youth who are victims only. Distinguishing between subtypes of victims may lead to even cleaner findings and facilitate better matching of individuals to specific interventions. Second, although the current study was longitudinal, it was not experimental. Without random assignment to treatment and control conditions, strong causal inferences about the relation of victimization to depressive cognitions are not possible. Carefully controlled prevention studies could significantly enhance our understanding of cause-effect relations in this domain. Third, the current findings have led us to speculate about the role of enhanced negative cognitions as a mediator of the relation between victimization and depression. Such conclusions, however, await multi-wave longitudinal investigations in which victimization, cognition, and depression are all tracked over time. Fourth, although our sample was socio-economically diverse, it was relatively homogenous from an ethnographic point of view. Additional research with ethnically diverse samples is needed to support the generalizability of these findings. Finally, the current study focused only on the effects of victimization by peers in the school setting. Although a large proportion of children’s social interactions occur with classmates, children can be victimized by peers in other social settings as well. Children may also be victimized by adults. Children who experience victimization in multiple contexts have even fewer social contexts to foster the development of healthy cognitions. The possibility that this puts such youths at even greater risk for depression is another important area for future research (e.g., Gibb & Abela, 2008).
Acknowledgments
This research was supported by a gift from Patricia and Rodes Hart, by support from the Warren Family Foundation, by NICHD grant 1R01HD059891) to David A. Cole. We thank Judy Bell, Mickey Dyce, and Dawn Young for their support at various stages of this project. We also thank the children, teachers, and parents who participated in the study.
Footnotes
Score distributions on our peer nomination measures of physical and relational victimization were positively skewed (skewness was 2.1 for relational victimization and 2.4 for physical victimization), virtually an inevitable finding when measures are proportions reflecting characteristics with base rates less than 50 percent. Our analytic strategy, however, treated these measures as independent variables (for which distributional assumptions of normality are not critical).
For two reasons, we have elected to report all significant results using an alpha of .05. One reason is that our various significant results reflect only subtle variations in what is virtually the same underlying pattern. This constitutes more of a replication across various cognitive measures than the emergence of qualitatively new and different results. Second, the results of peer victimization can be quite serious. Over the years, far more attention has been paid to perpetrators than to the victims of bullying. We prefer to run the risk of erring in the other direction. That said, we report exact p-values so that the reader can easily implement family-wise alpha corrections and standardized beta weights as indices of effect size.
Contributor Information
Keneisha R. Sinclair, Email: keneisha.r.sinclair@vanderbilt.edu.
Tammy Dukewich, Email: tdukewich@tntech.edu.
Julia Felton, Email: julia.w.felton@vanderbilt.edu.
Amy S. Weitlauf, Email: amy.s.weitlauf@vanderbilt.edu.
Melissa M. Maxwell, Email: Melissa.Maxwell@vanderbilt.edu.
Carlos Tilghman-Osborne, Email: carlos.e.osborne@vanderbilt.edu.
Amy Jacky, Email: amy.jacky@vanderbilt.edu.
References
- Abela JRZ. The hopelessness theory of depression: A test of the diathesis-stress and causal mediation components in third and seventh grade children. Journal of Abnormal Child Psychology. 2001;29(3):241–254. doi: 10.1023/a:1010333815728. [DOI] [PubMed] [Google Scholar]
- Abela JRZ, Hankin BL. Cognitive vulnerability to depression in children and adolescents: A developmental psychopathology perspective. New York: Guilford Press; 2008. [Google Scholar]
- Abela JRZ, Hankin BL. Cognitive vulnerability to depression in adolescents: A developmental psychopathology perspective. In: Nolen-Hoeksema S, Hilt LM, editors. Handbook of depression in adolescents. New York: Routledge/Taylor & Francis Group; 2009. pp. 335–376. [Google Scholar]
- Barchia K, Bussey K. The psychological impact of peer victimization: Exploring self-cognitive mediators of depression. Journal of Adolescence. 2010;33:615–623. doi: 10.1016/j.adolescence.2009.12.002. [DOI] [PubMed] [Google Scholar]
- Berg DH, Klinger DA. Gender differences in the relationship between academic self-concept and self-reported depressed mood in children. Sex Roles. 2009;61(7-8):501–509. [Google Scholar]
- Boivin M, Hymel S, Bukowski WM. The roles of social withdrawal, peer rejection, and victimization by peers in predicting loneliness and depressed mood in childhood. Development and Psychopathology. 1995;7:765–685. [Google Scholar]
- Boulton MJ, Smith PK. Bully-victim problems in middle-school children: Stability, self-perceived competence, peer perceptions and peer acceptance. British Journal of Developmental Psychology. 1994;12:315–329. [Google Scholar]
- Burt KB, Obradovic J, Long JD, Masten AS. The interplay of social competence and psychopathology over 20 years: Testing transactional and cascade models. Child Development. 2008;79(2):359–374. doi: 10.1111/j.1467-8624.2007.01130.x. [DOI] [PubMed] [Google Scholar]
- Callaghan S, Joseph S. Self-concept and peer victimization among school children. Personality and Individual Differences. 1995;18:161–163. [Google Scholar]
- Coie JD, Dodge KA, Coppotelli H. Dimensions and types of social status: A cross-age perspective. Developmental Psychology. 1982;18:557–570. [Google Scholar]
- Cole DA. Relation of social and academic competence to depressive symptoms in childhood. Journal of Abnormal Psychology. 1990;99:422–429. doi: 10.1037//0021-843x.99.4.422. [DOI] [PubMed] [Google Scholar]
- Cole DA. Change in self-perceived competence as a function of peer and teacher evaluation. Developmental Psychology. 1991;27:682–688. [Google Scholar]
- Cole DA, Ciesla JA, Dallaire DH, Jacquez FM, Pineda AQ, LaGrange B, Truss AE, Folmer AS, Tilghman-Osborne C, Felton JW. Emergence of attributional style and its relation to depressive symptoms. Journal of Abnormal Psychology. 2008;117(1):16–31. doi: 10.1037/0021-843X.117.1.16. [DOI] [PubMed] [Google Scholar]
- Cole DA, Jacquez F, Maschman TL. Social origins of depressive congitions: A longitudinal study of self-perceived competence in children. Cognitive Therapy & Research. 2001;25:377–395. [Google Scholar]
- Cole DA, Martin JM, Powers B. A competency-based model of child depression: A longitudinal study of peer, teacher, and self-evaluations. Journal of Child Psychology and Psychiatry. 1997;38(5):505–514. doi: 10.1111/j.1469-7610.1997.tb01537.x. [DOI] [PubMed] [Google Scholar]
- Cole DA, Maxwell SE. Statistical methods for risk-outcome research: Being sensitive to longitudinal structure. Annual Review of Clinical Psychology. 2009;5:71–96. doi: 10.1146/annurev-clinpsy-060508-130357. [DOI] [PubMed] [Google Scholar]
- Cole DA, Martin JM, Powers B, Truglio R. Modeling causal relations between academic and social competence and depression: A multi-trait multi-method longitudinal study of children. Journal of Abnormal Psychology. 1996;105(2):258–270. doi: 10.1037//0021-843x.105.2.258. [DOI] [PubMed] [Google Scholar]
- Cole DA, Maxwell MA, Dukewich TL, Yosick R. Targeted peer victimization and the construction of positive and negative self-cognitions: Connections to depressive symptoms in children. Journal of Clinical Child and Adolescent Psychology. 2010;39(3):421–445. doi: 10.1080/15374411003691776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole DA, Maxwell SE, Martin JM. Reflected self-appraisals: Strength and structure of the relation of teacher, peer, and parent ratings to children’s self-perceived competencies. Journal of Educational Psychology. 1997;89(1):55–70. [Google Scholar]
- Cooley CH. Human nature and the social order. New York: Scribner’s; 1902. [Google Scholar]
- Crick NR, Bigbee MA. Relational and overt forms of peer victimization: A multi-informant approach. Journal of Consulting and Clinical Psychology. 1998;66:337–347. doi: 10.1037//0022-006x.66.2.337. [DOI] [PubMed] [Google Scholar]
- Crick NR, Grotpeter JK. Relational aggression, gender, and social-psychological adjustment. Child Development. 1995;66(3):710–722. doi: 10.1111/j.1467-8624.1995.tb00900.x. [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Prinstein MJ. Applying depression-distortion hypotheses to the assessment of peer victimization in adolescents. Journal of Clinical Child and Adolescent Psychology. 2004;33:325–335. doi: 10.1207/s15374424jccp3302_14. [DOI] [PubMed] [Google Scholar]
- DeRosier ME. Group interventions and exercises for enhancing children’s communication, cooperation, and confidence. Sarasota, FL: Professional Resource Press; 2002. [Google Scholar]
- Dill EJ, Vernberg EM, Fonagy P, Twemlow SW, Gamm BK. Negative affect in victimized children: The roles of social withdrawal, peer rejection, and attitudes toward bullying. Journal of Abnormal Child Psychology. 2004;32(2):159–173. doi: 10.1023/b:jacp.0000019768.31348.81. [DOI] [PubMed] [Google Scholar]
- French DC, Jansen EA, Pidada S. United States and Indonesian children’s and adolescents’ reports of relational aggression by disliked peers. Child Development. 2002;73(4):1143–1150. doi: 10.1111/1467-8624.00463. [DOI] [PubMed] [Google Scholar]
- Frey KS, Hirschstein MK, Edstrom LV, Snell JL. Observed reductions in school bullying, nonbullying aggression, and destructive bystander behavior: A longitudinal evaluation. Journal of Educational Psychology. 2009;101:466–481. [Google Scholar]
- Frydenberg E, Lewis R. Boys play sport and girls to others: Age, gender, and ethnicity as determinants of coping. Journal of Adolescence. 1993;16:253–266. doi: 10.1006/jado.1993.1024. [DOI] [PubMed] [Google Scholar]
- Galen BR, Underwood MK. A developmental investigation of social aggression in children. Developmental Psychology. 1997;33(4):589–600. doi: 10.1037//0012-1649.33.4.589. [DOI] [PubMed] [Google Scholar]
- Garber J. Classification of childhood psychopathology: A developmental perspective. Child Development. 1984;55:30–48. [PubMed] [Google Scholar]
- Gibb BE, Abela JRZ. Emotional abuse, verbal victimization, and the development of children’s negative inferential styles and depressive symptoms. Cognitive Therapy and Research. 2008;32(2):161–176. [Google Scholar]
- Gibb BE, Abramson LY, Alloy LB. Emotional maltreatment from parents, verbal peer victimization, and cognitive vulnerability to depression. Cognitive Therapy and Research. 2004;28:1–21. [Google Scholar]
- Grills AE, Ollendick TH. Peer victimization, global self-worth, and anxiety in middle school children. Journal of Clinical Child and Adolescent Psychology. 2002;31(1):59–68. doi: 10.1207/S15374424JCCP3101_08. [DOI] [PubMed] [Google Scholar]
- Grotpeter JK, Crick NR. Relational aggression, overt aggression, and friendship. Child Development. 1996;67:2328–2338. [PubMed] [Google Scholar]
- Hankin BL. Stability of cognitive vulnerabilities to depression: A short-term prospective multiwave study. Journal of Abnormal Psychology. 2008;117:324–333. doi: 10.1037/0021-843X.117.2.324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hankin BL, Abramson LY. Development of gender differences in depression: An elaborated cognitive vulnerability-transactional stress theory. Psychological Bulletin. 2001;127(6):773–796. doi: 10.1037/0033-2909.127.6.773. [DOI] [PubMed] [Google Scholar]
- Harter S. The perceived competence scale for children. Child Development. 1982;53:87–97. [PubMed] [Google Scholar]
- Harter S. Manual for the self-perception profile for children. Denver, CO: University of Denver; 1985. [Google Scholar]
- Harter S. Developmental differences in the nature of self-representations: Implications for the understanding, assessment, and treatment of maladaptive behavior. Cognitive Therapy and Research. 1990;14:113–142. [Google Scholar]
- Harter S. The development of self-representations during childhood and adolescence. In: Leary RR, Tangney JP, editors. Handbook of self and identity. New York: Guilford; 2003. pp. 610–642. [Google Scholar]
- Hawker DSJ, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry. 2000;41:441–455. [PubMed] [Google Scholar]
- Hunter SC, Boyle JME. Perceptions of control in the victims of school bullying: The importance of early intervention. Educational Research. 2002;44:323–336. [Google Scholar]
- Juvonen J, Graham S, editors. Peer harassment in school: The plight of the vulnerable and victimized. New York: Guilford; 2001. [Google Scholar]
- Kaslow NJ, Stark KD, Printz B, Livingston R, Tsai SL. Cognitive Triad Inventory for Children: Development and relation to depression and anxiety. Journal of Clinical Child Psychology. 1992;21:339–347. [Google Scholar]
- Kercher A, Rapee RM. A test of a cognitive diathesis-Stress generation pathway in early adolescent depression. Journal of Abnormal Child Psychology. 2009;37(6):845–855. doi: 10.1007/s10802-009-9315-3. [DOI] [PubMed] [Google Scholar]
- Kochenderfer-Ladd B, Ladd GW. Variations in peer victimization: Relations to children’s maladjustment. In: Juvonen J, Graham S, editors. Peer harassment in school: The plight of the vulnerable and victimized. New York: Guilford; 2001. pp. 25–48. [Google Scholar]
- LaGrange B, Cole DA, Dallaire DH, Ciesla JA, Pineda AQ, Truss AE, Folmer A. Developmental changes in depressive cognitions: A longitudinal evaluation of the Cognitive Triad Inventory for Children. Psychological Assessment. 2008;20:217–226. doi: 10.1037/1040-3590.20.3.217. [DOI] [PubMed] [Google Scholar]
- Masten AS, Hubbard JJ, Scott GD. Competence in the context of adversity: Pathways to resilience and maladpation from childhood to late adolescence. Development and Psychopathology. 1999;11:143–149. doi: 10.1017/s0954579499001996. [DOI] [PubMed] [Google Scholar]
- Mead GH. The social self. Journal of Philosophy, Psychology, and Scientific Methods. 1913;10:374–380. [Google Scholar]
- Muris P, Meesters C, Fijen P. The self-perception profile for children: Further evidence for its factor structure, reliability, and validity. Personality and Individual Differences. 2003;35:1791–1802. [Google Scholar]
- Mynard H, Joseph S. Development of the Multidimensional Peer-Victimization Scale. Aggressive Behavior. 2000;26:169–178. [Google Scholar]
- Nixon CL, Werner NE. Reducing adolescents’ involvement with relational aggression: Evaluating the effectiveness of the Creating a Safe School (CASS) Intervention. Psychology in the Schools. 2010;47(6):606–620. [Google Scholar]
- Nolen-Hoeksema S, Girgus JS, Seligman MEP. Predictors and consequences of childhood depressive symptoms: A 5-Year Longitudinal Study. Journal of Abnormal Psychology. 1992;101(3):405–422. doi: 10.1037//0021-843x.101.3.405. [DOI] [PubMed] [Google Scholar]
- Olweus D. Bullying or peer abuse at school: Facts and interventions. Current Directions in Psychological Science. 1995;4(6):196–200. [Google Scholar]
- Olweus D, Limber SP, Flerx VC, Mullin N, Riese J, Snyder M. Olweus Bullying Prevention Program: Schoolwide guide. Center City, MN: Hazelden; 2007. [Google Scholar]
- Pellegrini AD, Long JD. Longitudinal study of bullying, dominance, and victimization during the transition from primary through secondary school. British Journal of Developmental Psychology. 2002;20:259–280. [Google Scholar]
- Pepler D, Craig W, Yuile A, Connolly J. Girls who bully: A developmental and relational perspective. In: Putallaz MB, editor. Aggression, antisocial behavior, and violence among girls: A developmental perspective. New York: Guildford; 2004. pp. 90–109. [Google Scholar]
- Prinstein MJ, Boegers J, Vernberg EM. Overt and relational aggression in adolescents: Social-psychological adjustments of aggressors and victims. Journal of Clinical Child Psychology. 2001;30(4):479–491. doi: 10.1207/S15374424JCCP3004_05. [DOI] [PubMed] [Google Scholar]
- Rose AJ, Rudolph KD. A review of sex differences in peer relationship processes: Potential trade-offs for the emotional and behavioral development of girls and boys. Psychological Bulletin. 2006;132(1):98–131. doi: 10.1037/0033-2909.132.1.98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schniering CA, Rapee RM. Development and validation of a measure of children’s automatic thoughts: The children’s automatic thoughts scale. Behaviour Research and Therapy. 2002;40:1091–1109. doi: 10.1016/s0005-7967(02)00022-0. [DOI] [PubMed] [Google Scholar]
- Shrauger JS, Schoeneman TJ. Symbolic interactionist view of self-concept: Through the looking-glass darkly. Psychological Bulletin. 1979;86(3):549–573. [Google Scholar]
- Smith RL, Rose AJ, Schwartz-Mette RA. Relational and overt aggression in childhood and adolescence: Clarifying mean-level gender differences and associations with peer acceptance. Social Development. 2010;19(2):243–268. doi: 10.1111/j.1467-9507.2009.00541.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Urhlass DJ, Schofield CA, Coles ME, Gibb BE. Self-perceived competence and prospective changes in symptoms of depression and social anxiety. Journal of Behavior Therapy and Experimental Psychiatry. 2009;40(2):329–337. doi: 10.1016/j.jbtep.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weersing VR, Brent DA. Treating depression in adolescents using cognitive-behavioral therapy. In: Weisz JR, Kazdin AE, editors. Evidence-based psychotherapies for children and adolescents. New York: Guilford; 2010. pp. 126–139. [Google Scholar]
- Weiss B, Garber J. Developmental differences in the phenomenology of depression. Development and Psychopathology. 2003;15:403–430. doi: 10.1017/s0954579403000221. [DOI] [PubMed] [Google Scholar]
- Widaman KF. Best practices in quantitative methods for developmentalists: III. missing data: What to do with or without them. Monographs of the Society for Research in Child Development. 2006;71(3):42–64. doi: 10.1111/j.1540-5834.2006.07103001.x. [DOI] [PubMed] [Google Scholar]
- Woods S, Done J, Kalsi H. Peer victimization and internalizing difficulties: The moderating role of friendship quality. Journal of Adolescence. 2009;32:293–308. doi: 10.1016/j.adolescence.2008.03.005. [DOI] [PubMed] [Google Scholar]