

Abstract
Objective
Quantification of chiropractic high-velocity, low-amplitude spinal manipulation (HVLA-SM) may require biomechanical equipment capable of sampling data at high rates. However, there are few studies reported in the literature regarding the minimal sampling rate required to record the HVLA-SM force-time profile data accurately and precisely. The purpose of this study was to investigate the effect of different sampling rates on the quantification of forces, durations, and rates of loading of simulated side posture lumbar spine HVLA-SM delivered by doctors of chiropractic.
Methods
Five doctors of chiropractic (DCs) and 5 asymptomatic participants were recruited for this study. Force-time profiles were recorded during (i) 52 simulated HVLA-SM thrusts to a force transducer placed on a force plate by 2 DCs and (ii) 12 lumbar side posture HVLA-SM on 5 participants by 3 DCs. Data sampling rate of the force plate remained the same at 1000 Hz, whereas the sampling rate of the force transducer varied at 50, 100, 200, and 500 Hz. The data were reduced using custom-written MATLAB (Mathworks, Inc, Natick, MA) and MathCad (version 15; Parametric Technologies, Natick, MA) programs and analyzed descriptively.
Results
The average differences in the computed durations and rates of loading are smaller than 5% between 50 and 1000 Hz sampling rates. The differences in the computed preloads and peak loads are smaller than 3%.
Conclusions
The small differences observed in the characteristics of force-time profiles of simulated manual HVLA-SM thrusts measured using various sampling rates suggest that a sampling rate as low as 50 to 100 Hz may be sufficient. The results are applicable to the manipulation performed in this study: manual side posture lumbar spine HVLA-SM.
Key Indexing Terms: Biomechanics, Manipulation, Spinal, Chiropractic, Manual Therapy
High-velocity, low-amplitude spinal manipulation (HVLA-SM) is a commonly used procedure in chiropractic practice (eg, also known as side-lying diversified or Gonstead style lumbar, lumbosacral, or sacroiliac joint chiropractic manipulation/adjustment). Participants are placed in a lateral recumbent or side-lying position, with the superior or free hip and knee flexed and adducted across the midline. The lumbar spine and pelvis remained in a neutral position, approximately perpendicular to the adjusting table surface. A quick, short controlled movement of the clinician’s shoulder, arm, and hand combined with a slight body drop provide the single impulse load or thrust to the contact point. Because spinal manipulation is a form of mechanical stimulus, quantification of the associated force-time characteristics is important.1–3
Forces applied by doctors to patients can be measured directly using a force transducer at the doctor/patient interface (eg, hand to spine).4–12 The forces measured are referred to as applied or contact forces. Van Zoest et al13,14 described a measurement method to quantify the 3-dimensional forces at the doctor/patient interface using 3-dimensional force transducers and found, in addition to normal forces, shear forces occurred during thoracic and lumbar manipulations. The forces transmitted to patients can also be measured with force plates placed underneath the patients.15–20 These forces are referred to as transmitted forces or loads. Triano and Schultz15 reported on the transmitted loads to the lumbar spine using a force plate embedded in the chiropractic table and estimating the loads in the lumbar spine using inverse dynamics approach and reported large shear loads and moment loads. Furthermore, a flexible pressure mat has been used to measure contact forces at the doctor/patient interface in the thoracic, cervical, and lumbosacral regions. Herzog et al,4,12 Forand et al,6 Hessell et al,8 Suter et al,9 Kawchuk and Herzog,11 and Kirstukas and Backman10 measured doctor/patient contact forces during thoracic HVLA-SM using a pressure resistance film and reported very large normal forces with high rate of loading. Only the normal component of the contact force can be obtained when using pressure pads or pressure resistance film-type devices. These reported investigations help advance our understanding of the magnitude of force during preload phase and thrusting phase, duration of the manipulation, rate of loading, and contact area in thoracic and lumbar spinal manipulation.
High-velocity, low-amplitude spinal manipulation is a dynamic event that involves delivery of forces at a high speed in a short duration in the order of 100 to 500 milliseconds. Some investigators have measured the force-time profiles at the contact hand at a relatively low sampling frequency of 50 to 100 Hz,7–10 whereas others21,22 have measured at a higher sampling rate of 300 to 1000 Hz19,21,22 or 2500 to 5000 Hz.23,24 However, to the best of our knowledge, there is little information available regarding the effect of sampling rate on capturing the force-time characteristics of HVLA-SM. A study reported by Hori et al25 on the measurement of peak force, power, and velocity during jumping concluded that up to 100 Hz sampling rates the differences are small, whereas sampling rates of 50 and 25 Hz could lead to differences of up to 13%. Because the HVLA-SM delivering speed is similar to the speed in jumping, it is possible that the sampling rate may also affect the accuracy of capturing HVLA-SM force-time characteristics.
The objectives of this study were to determine the minimal sampling rate required to accurately quantify the force-time characteristics of HVLA-SM, including preload and peak forces, duration of loading, duration of unloading, total duration, and rates of loading and unloading and to quantify the differences in those characteristics when data were collected at different sampling rates, whereas HVLA-SM–type thrusts were repeatedly delivered to a force transducer by experienced doctors of chiropractic (DCs).
Methods
Experienced chiropractic clinicians were recruited to deliver the simulated high-velocity, low-amplitude (HVLA) thrusts. This study was approved by the Palmer College of Chiropractic Institutional Review Board. All participants provided signed informed consent documents.
Instrumentation
Experiment 1
Force-time profiles were recorded when 2 clinicians (1 male DC with 23 years of experience and 1 female DC with 31 years of experience) delivered simulated HVLA thrusts to a miniature force transducer (Model no. mini45; ATI Industrial Automation, Apex, NC) placed on the top of a force plate (Model no. 4060-NC; Bertec, Inc, Columbus, OH). The transducer has a diameter of 45 mm, a thickness of 15.7 mm, and a contact surface of 15.9 cm2. Both the force plate and the force transducer are capable of measuring 3-dimensional forces and moments. Figure 1 depicts a doctor performing a thrust on the force transducer, which was placed directly on the force plate. Data recordings were made using Motion Monitor software with a 16-bit analog-to-digital data acquisition system (Innovative Sports Training, Inc, Chicago, IL). To investigate the effect of sampling rate on force-time characteristics, the sampling rate of the force plate remained same at 1000 Hz, whereas the sampling rate of the force transducer was varied at 50, 100, 200, and 500 Hz. Data collected from both force plate and force transducer were exported to ASCII formatted text files for further data reduction and analysis.
Fig. 1.
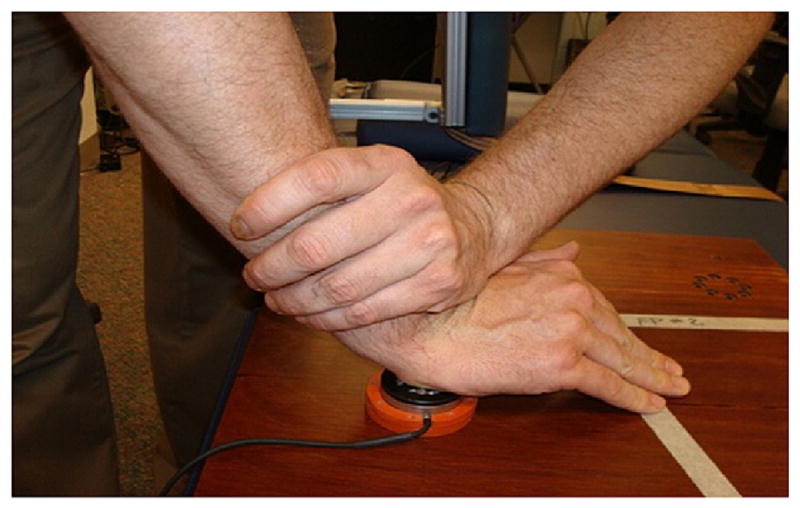
A photograph showing the force transducer, force plate, and the doctor’s hand position for delivering simulated HVLA thrusts. (Color version of figure is available online.)
Experiment 2
Three male DCs with an average of 14 (range 12–15) years of experience and 5 asymptomatic participants (4 male and 1 female, with age ranging from 26–51 years old) were recruited for this study. Upon physical examination, the participants were excluded if the clinician felt that there was a contraindication to spinal manipulation. Participants were included if examination indicated the need for spinal manipulation. Each DC performed side posture HVLA-SM on all participants on different days. There were at least 7 days in between for each participant to receive spinal manipulations. During this experiment, the 3-dimensional force transducer was placed between the doctor’s hand and the participant’s back. Standard side posture treatment table was used for this study. Force-time profile data were collected during 12 HVLA-SM, with a sampling rate of 1000 Hz. From these data, we used the resampling function in MathCad (version 15; Parametric Technologies, Natick, MA) to recreate force-time profiles at frequencies of 50, 100, 200, and 500 Hz to mimic data collection at lower sampling rates.
Data Reduction
For the first experiment, the doctors delivered a total of 52 simulated HVLA thrusts. Exported data were processed using custom-developed programs in MATLAB (Mathworks, Inc, Natick, MA). Force-time profile plots were generated from the raw data. For the second experiment, we obtained 60 force-time profiles (12 from data collection and 48 from resampling at 50, 100, 200, and 500 Hz). From those plots, the examiners identified the preload phase and the beginning and end of the thrust using visual inspection. Preload and peak load amplitude, durations of loading and unloading, and rate of loading and unloading as well as power spectrum density were computed using MATLAB and MathCAD programs. These parameters are defined in a manner similar to what has been described by Herzog et al,4 Triano et al,18,20 and Cohen et al.17 The magnitude of preload, magnitude of peak load, time to peak load, average rate of loading, and average rate of unloading were then calculated.
Data Analysis
We performed descriptive analyses on the preload, peak load, duration of thrust loading, duration of unloading, rate of loading, and rate of unloading. The differences in these values as computed using data collected at 50, 100, 200, and 500 Hz by the force transducer against the data collected at 1000 Hz by the force plate. The percentages of those differences were also calculated.
Results
Figure 2 shows a typical graph of force-time profile collected at 50 and 1000 Hz sampling rates. The descriptive statistics (mean ± SD) for the force-time profiles from the first experiment of 52 simulated spinal manipulations are preload force at 94.4 ± 71.7 N, peak normal force at 432.5 ± 122.8 N, duration of loading at 154 ± 70 milliseconds, rate of loading at 2692 ± 1633 N/s, duration of unload at 420 ± 257 milliseconds, rate of unloading at 1567 ± 1334 N/s, and duration of thrust at 574 ± 260 milliseconds, respectively. The descriptive statistics for the force-time profiles based on the second experiment of 12 HVLA-SM on asymptomatic participants are preload force 106.3 ± 55.5 N, peak force at 327.6 ± 90.7 N, duration of loading at 261 ± 163 milliseconds, rate of loading at 1077.6 ± 571.9.2 N/s, duration of unload at 509 ± 143 milliseconds, rate of unloading at 683.3 ± 259.4 N/s, and total duration of thrust at 770 ± 212 milliseconds, respectively.
Fig. 2.
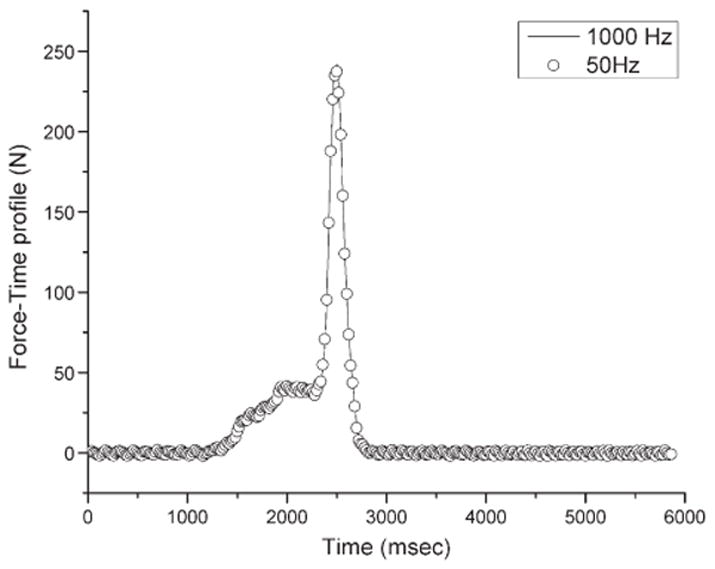
A graph of typical force-time profile for data sampled at 50 and 1000 Hz.
Figure 3 shows a typical power spectral graph of a force-time data during HVLA-SM. The maximum meaningful frequency was defined as the highest frequency with power density above the background white noise, for example, the relative flat region higher than 50 Hz as illustrated in Figure 3.
Fig. 3.
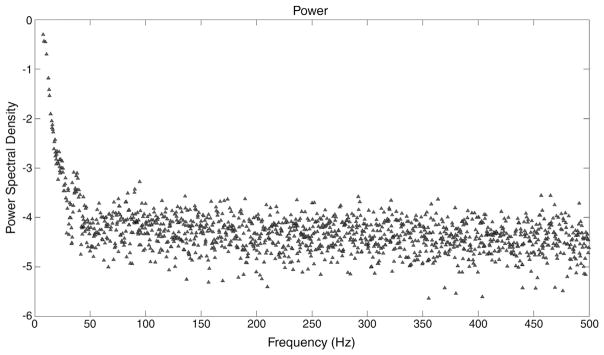
Power spectrum density of a representative dataset collected at 1000 Hz with power in logarithm scale.
Based on the power spectral density information for the 52 manipulations, the maximum power occurred at a mean frequency of 3.34 Hz (minimum, 1 Hz; maximum, 12 Hz) and the frequency where the power has reached a plateau had a mean value of 26 Hz (minimum, 16 Hz; maximum, 41 Hz).
Tables 1 and 2 summarizes the differences in preload, peak load, durations of loading and unloading, total duration, and rates of loading and unloading when normalized to these characteristics determined at 1000 Hz.
Table 1.
Percentage differences of measured force-time profile characteristics using the force plate at 1000 Hz and those using the force transducers at 50, 100, 200, and 500 Hz
| 50 Hz (n = 20)
|
100 Hz (n = 12)
|
200 Hz (n = 10)
|
500 Hz (n = 10)
|
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Preload | 1.37 | 22.74 | −0.54 | 6.14 | 3.43 | 9.64 | −1.05 | 1.31 |
| Peak load | −3.05 | 3.31 | −0.91 | 0.44 | −0.80 | 0.17 | −0.53 | 0.32 |
| Duration of load | −4.75 | 12.31 | 5.94 | 11.38 | 0.51 | 15.40 | 2.94 | 3.52 |
| Duration of unload | 1.84 | 7.71 | 3.24 | 9.24 | −1.15 | 4.09 | −4.39 | 5.77 |
| Total duration | −0.74 | 3.01 | 3.58 | 5.87 | −0.20 | 6.45 | −1.52 | 3.88 |
| Rate of load | 3.01 | 13.80 | −5.62 | 8.18 | −2.42 | 10.50 | −3.27 | 3.09 |
| Rate of unload | −4.30 | 7.79 | −3.39 | 7.74 | 0.51 | 4.30 | 4.40 | 6.66 |
Table 2.
Percentage differences of side posture, HVLA lumbar spine manipulation characteristics measured at 1000 Hz and those resampled at lower frequencies
| 50 Hz (n = 12)
|
100 Hz (n = 12)
|
200 Hz (n = 12)
|
500 Hz (n = 12)
|
|||||
|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Preload | 0.07 | 1.77 | 0.52 | 1.51 | −0.32 | 0.92 | 0.20 | 0.30 |
| Peak load | 0.39 | 0.52 | 0.18 | 0.43 | 0.06 | 0.39 | 0.00 | 0.46 |
| Duration of load | 3.24 | 7.16 | 4.14 | 6.01 | 3.71 | 7.09 | 0.27 | 6.65 |
| Duration of unload | −2.11 | 4.40 | −2.07 | 2.78 | −1.90 | 2.48 | 0.45 | 2.65 |
| Total duration | −0.19 | 1.22 | −0.08 | 0.48 | −0.11 | 0.24 | 0.04 | 0.07 |
| Rate of load | −3.06 | 7.49 | −4.65 | 6.98 | −4.41 | 9.95 | 1.25 | 8.18 |
| Rate of unload | 0.71 | 6.71 | 1.01 | 5.98 | 2.49 | 4.63 | 0.33 | 3.34 |
Discussion
The thrusts that were quantified in experiment 1 of the present study were simulations of HVLA-SM delivered by pressing on a force transducer. The simulations are reasonable as their force-time profile characteristics including preload and peak forces, durations, and rates of loading values are in the range reported in the literature for the thoracic, lumbar, and sacroiliac HVLA-SM4,15,21,6,26,14,22 and experiment 2 of the present study.
Biomechanics researchers are aware that the recommended sampling rates are at least twice the Nyquist frequency.27 If sampled at a rate that is too low, it is possible to miss important information. For example, the characteristics of the thrust will not be able to be determined accurately. If over sampling the data, one has to deal with a large quantity of data occupying excessive storage and requiring more cumbersome data processing and reduction. Therefore, recommended sampling frequencies for walking are 50 to 100 Hz for motion capture, running and sprinting at 100 to 200 Hz, javelin throw at 200 to 300 Hz, 1000 Hz for ground reaction force data collection.27 The recommendation for electromyographic data sampling frequencies are 1000 Hz or higher.27 The power spectral density analysis on HVLA-SM data of present study revealed that the power reaches a plateau at an average frequency of 26 Hz, indicating that, in theory, a sampling rate of 52 or above may provide adequate information about the HVLA-SM force-time characteristics.
From the data we obtained in sampling at different frequencies, the mean differences are smaller than 5% in durations and rates of loading for all lower frequencies compared with those at 1000 Hz. The differences in the magnitudes of the loads are smaller than 3%. This suggests that data acquisition at the lower frequencies examined in the present work does not substantially reduce the accuracy of measurement. However, we observed larger SDs at lower frequencies, indicating that the accuracy of results may degrade if sample size is too small.
This study provides information that was not previously available as to how sampling frequency influences the measurement of force-time profile characteristics of manual therapy techniques such as HVLA-SM. For example, some equipment such as thin film sensors allows sampling rates in the order of only 50 to 100 Hz. Based on the findings of this study, this equipment may be used without loss of accuracy. This will allow researchers the confidence to apply these sensors with lower sampling rate in their studies, while taking advantage of the pliable nature of these devices that make them more suitable for measurement between doctor’s hand and the participant’s spine. Other equipment such as force sensors and force plates has the capacity to sample at much higher frequencies. Higher frequencies may be needed for some applications. However, in some applications such as monitoring force-time profiles of HVLA-SM, sampling at higher frequencies may not provide better accuracy and yet would produce excessive volume of data and consequently increase the data processing time and cost.
The results from this study are useful for researchers and clinicians and to understand the force-time profile characteristics collected at various sampling rates during manual HVLA side posture spinal manipulations. Knowledge that smaller sampling frequencies give reasonably accurate results can be useful to select the equipment for measuring forces and design future studies. This implies that training of students and clinicians can be done using low sampling rate force-measuring equipment that is more pliable and, therefore, causes less interference with their normal delivery of the thrust.
Limitations
The findings in this study relate to the specific techniques used by the 3 DCs and, therefore, cannot be extrapolated to other manipulation techniques or other practitioners. As well, the patients were not symptomatic, and therefore, force applied in the treatment setting may be different. These experiments are based on the doctor’s delivering on force transducers as well as side posture lumbar HVLA-SM on asymptomatic participants. This study was not intended to characterize treatment techniques delivered through impulse adjusting instruments28,29 that deliver much quicker thrusts than manually delivered thrusts. Chiropractic techniques using treatment tables with drop mechanism may also have different characteristics requiring a higher sampling rate.
In addition, different regions of spine may have different compliance characteristics; thus, forces from this study (eg, to the lumbar spine) may not be similar to other areas of the body (eg, cervical/thoracic spine, upper/lower extremities). The current study only mimicked the lumbar HVLA-SM. Caution is needed when attempting to generalize the findings of this study to manual treatment on other body regions. Furthermore, this study only evaluated the normal component of the force-time profile characteristics, whereas shear components were not. Therefore, further studies are needed to address these limitations.
Conclusions
Small differences were observed in the characteristics of force-time profiles of simulated and actual side posture, HVLA lumbar spine manipulation thrusts measured using various sampling rates. This suggests that a sampling rate as low as 50 to 100 Hz may be adequate to describe these thrusts accurately.
Practical Application.
This study demonstrates that sampling rates of 50 to 100 Hz for measurement of HVLA-SMs performed by DCs. The differences in force-time characteristics are smaller than 5% of 1000 Hz sampling rates.
Acknowledgments
Funding Sources
This investigation was conducted in a facility constructed with support from Research Facilities Improvement Program Grant number C06 RR15433-01 from the National Center for Research Resources, National Institutes of Health.
Footnotes
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike License, which permits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
Potential Conflicts of Interest
No conflicts of interest were reported for this study.
References
- 1.Cramer G, Budgell B, Henderson C, Khalsa P, Pickar J. Basic science research related to chiropractic spinal adjusting: the state of the art and recommendations revisited. J Manipulative Physiol Ther. 2006;29:726–61. doi: 10.1016/j.jmpt.2006.09.003. [DOI] [PubMed] [Google Scholar]
- 2.Brennan PC, Cramer GD, Kirstukas SJ, Cullum ME. Basic science research in chiropractic: the state of the art and recommendations for a research agenda. J Manipulative Physiol Ther. 1997;20:150–68. [PubMed] [Google Scholar]
- 3.Herzog W. The mechanical, neuromuscular, and physiologic effects produced by spinal manipulation. In: Herzog W, editor. Clinical Biomechanics of Spinal Manipulation. Philadelphia: Churchill Livingston; 2000. pp. 191–207. [Google Scholar]
- 4.Herzog W, Conway PJ, Kawchuk GN, Zhang Y, Hasler EM. Forces exerted during spinal manipulative therapy. Spine (Phila Pa 1976) 1993;18:1206–12. doi: 10.1097/00007632-199307000-00014. [DOI] [PubMed] [Google Scholar]
- 5.Herzog W, Kats M, Symons B. The effective forces transmitted by high-speed, low-amplitude thoracic manipulation. Spine (Phila Pa 1976) 2001;26:2105–10. doi: 10.1097/00007632-200110010-00012. [DOI] [PubMed] [Google Scholar]
- 6.Forand D, Drover J, Suleman Z, Symons B, Herzog W. The forces applied by female and male chiropractors during thoracic spinal manipulation. J Manipulative Physiol Ther. 2004;27:49–56. doi: 10.1016/j.jmpt.2003.11.006. [DOI] [PubMed] [Google Scholar]
- 7.Herzog W, Scheele D, Conway PJ. Electromyographic responses of back and limb muscles associated with spinal manipulative therapy. Spine (Phila Pa 1976) 1999;24:146–52. doi: 10.1097/00007632-199901150-00012. [DOI] [PubMed] [Google Scholar]
- 8.Hessell BW, Herzog W, Conway PJ, McEwen MC. Experimental measurement of the force exerted during spinal manipulation using the Thompson technique. J Manipulative Physiol Ther. 1990;13:448–53. [PubMed] [Google Scholar]
- 9.Suter E, Herzog W, Conway PJ, Zhang YT. Reflex response associated with manipulative treatment of the thoracic spine. J Neuromusculoskelet Syst. 2011;2:124–30. [Google Scholar]
- 10.Kirstukas SJ, Backman JA. Physician-applied contact pressure and table force response during unilateral thoracic manipulation. J Manipulative Physiol Ther. 1999;22:269–79. doi: 10.1016/s0161-4754(99)70059-x. [DOI] [PubMed] [Google Scholar]
- 11.Kawchuk GN, Herzog W. Biomechanical characterization (fingerprinting) of five novel methods of cervical spine manipulation. J Manipulative Physiol Ther. 1993;16:573–7. [PubMed] [Google Scholar]
- 12.Herzog W, Zhang YT, Conway PJ, Kawchuk GN. Cavitation sounds during spinal manipulative treatments. J Manipulative Physiol Ther. 1993;16:523–6. [PubMed] [Google Scholar]
- 13.van Zoest GG, van den Berg HT, Holtkamp FC. Three-dimensionality of contact forces during clinical manual examination and treatment: a new measuring system. Clin Biomech (Bristol, Avon) 2002;17:719–22. doi: 10.1016/s0268-0033(02)00132-8. [DOI] [PubMed] [Google Scholar]
- 14.van Zoest GG, Gosselin G. Three-dimensionality of direct contact forces in chiropractic spinal manipulative therapy. J Manipulative Physiol Ther. 2003;26:549–56. doi: 10.1016/j.jmpt.2003.08.001. [DOI] [PubMed] [Google Scholar]
- 15.Triano J, Schultz AB. Loads transmitted during lumbosacral spinal manipulative therapy. Spine (Phila Pa 1976) 1997;22:1955–64. doi: 10.1097/00007632-199709010-00003. [DOI] [PubMed] [Google Scholar]
- 16.Chiradejnant A, Latimer J, Maher CG. Forces applied during manual therapy to patients with low back pain. J Manipulative Physiol Ther. 2002;25:362–9. doi: 10.1067/mmt.2002.126131. [DOI] [PubMed] [Google Scholar]
- 17.Cohen E, Triano JJ, McGregor M, Papakyriakou M. Biomechanical performance of spinal manipulation therapy by newly trained vs. practicing providers: does experience transfer to unfamiliar procedures? J Manipulative Physiol Ther. 1995;18:347–52. [PubMed] [Google Scholar]
- 18.Triano JJ, Rogers CM, Combs S, Potts D, Sorrels K. Quantitative feedback versus standard training for cervical and thoracic manipulation. J Manipulative Physiol Ther. 2003;26:131–8. doi: 10.1016/S0161-4754(02)54105-1. [DOI] [PubMed] [Google Scholar]
- 19.Triano JJ, Scaringe J, Bougie J, Rogers C. Effects of visual feedback on manipulation performance and patient ratings. J Manipulative Physiol Ther. 2006;29:378–85. doi: 10.1016/j.jmpt.2006.04.014. [DOI] [PubMed] [Google Scholar]
- 20.Triano JJ, Rogers CM, Combs S, Potts D, Sorrels K. Developing skilled performance of lumbar spine manipulation. J Manipulative Physiol Ther. 2002;25:353–61. doi: 10.1067/mmt.2002.126132. [DOI] [PubMed] [Google Scholar]
- 21.Descarreaux M, Dugas C, Lalanne K, Vincelette M, Normand MC. Learning spinal manipulation: the importance of augmented feedback relating to various kinetic parameters. Spine J. 2006;6:138–45. doi: 10.1016/j.spinee.2005.07.001. [DOI] [PubMed] [Google Scholar]
- 22.Descarreaux M, Dugas C. Learning spinal manipulation skills: assessment of biomechanical parameters in a 5-year longitudinal study. J Manipulative Physiol Ther. 2010;33:226–30. doi: 10.1016/j.jmpt.2010.01.011. [DOI] [PubMed] [Google Scholar]
- 23.Colloca CJ, Gunzburg R, Freeman BJ, Szpalski M, Afifi M, Moore RJ. Biomechanical quantification of pathologic manipulable spinal lesions: an in vivo ovine model of spondylolysis and intervertebral disc degeneration. J Manipulative Physiol Ther. 2012;35:354–66. doi: 10.1016/j.jmpt.2012.04.018. [DOI] [PubMed] [Google Scholar]
- 24.Colloca CJ, Cunliffe C, Pinnock MH, Kim YK, Hinrichs RN. Force-time profile characterization of the McTimoney toggle-torque-recoil technique. J Manipulative Physiol Ther. 2009;32:372–8. doi: 10.1016/j.jmpt.2009.04.005. [DOI] [PubMed] [Google Scholar]
- 25.Hori N, Newton RU, Kawamori N, McGuigan MR, Kraemer WJ, Nosaka K. Reliability of performance measurements derived from ground reaction force data during countermovement jump and the influence of sampling frequency. J Strength Cond Res. 2009;23:874–82. doi: 10.1519/JSC.0b013e3181a00ca2. [DOI] [PubMed] [Google Scholar]
- 26.Conway PJ, Herzog W, Zhang Y, Hasler EM, Ladly K. Forces required to cause cavitation during spinal manipulation of the thoracic spine. Clin Biomech. 1993 Jul;8:210–4. doi: 10.1016/0268-0033(93)90016-B. [DOI] [PubMed] [Google Scholar]
- 27.Power Giakas G. Analysis Spectrum. Power spectrum analysis and filtering. In: Stergiou N, editor. Innovative Analysis of Human Movement. Champaign, Illinois: Human Kinetics; 2004. [Google Scholar]
- 28.Keller TS, Colloca CJ, Fuhr AW. Validation of the force and frequency characteristics of the activator adjusting instrument: effectiveness as a mechanical impedance measurement tool. J Manipulative Physiol Ther. 1999;22:75–86. doi: 10.1016/s0161-4754(99)70111-9. [DOI] [PubMed] [Google Scholar]
- 29.Colloca CJ, Keller TS, Black P, Normand MC, Harrison DE, Harrison DD. Comparison of mechanical force of manually assisted chiropractic adjusting instruments. J Manipulative Physiol Ther. 2005;28:414–22. doi: 10.1016/j.jmpt.2005.06.004. [DOI] [PubMed] [Google Scholar]