

Abstract
Background:
Obesity has been associated with several co-morbidities such as diabetes and increased mortality. In general, the use of medication promotes only a modest weight loss in the range of 2 to 10 kg, usually most effective during the first 6 months of therapy; however, studies have shown positive effects on other risk factors such as blood pressure and serum glucose levels, but there are fewer studies in patients with diabetes. The aim of this study was to assess the effect of topiramate on weight reduction patients with type 2 diabetes.
Materials and Methods:
This was a 32-week randomized clinical trial study of 69 subjects during 2008-2010. Patients, in two treatment groups were given topiramate (39 patients) and Placebo (30 patients) and were subjected to participation in a non-pharmacologic lifestyle intervention program; which were randomly allocated in our two groups. The percentage change in body weight and Body Mass Index (BMI) at the end of the study was the primary efficacy endpoint and secondary indicators were changes in blood pressure (BP), proportion of subjects who achieved 5% or 10% weight loss, changes in lipid profile (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides); and changes in glycosylated hemoglobin (HgA1c). Paired samples and independent samples t-test was used for statistical analysis. (RCT code: IRCT201112036027N2).
Results:
All results were extracted on base of 69 (Intended to treat) ITT patients. Mean BMI changes was significantly higher in patients treated with topiramate (-1.08 1.90 vs. +0.086 ± 1.05 kg/m², P = 0.006). Mean weight loss percentage was significantly different between active and placebo groups (-3.02 ± 5.78% vs. +0.32 ± 3.54%, P = 0.005) and systolic blood pressure and HgA1C significantly decreased in patients treated with topiramate (P = 0.021 and P = 0.047, respectively).
Conclusion:
Topiramate induced weight loss and improved glycemic control in obese, diabetic patients.
Keywords: Obesity, topiramate, type 2 diabetes
INTRODUCTION
The global prevalnce of Obesity as the sixth most important risk factor for common health is increasing; however, type 2 diabetes is the most devestating chronic complication of obesity; a condition along with obesity thaht is becomming more common.[1,2]
Some studies show that in western countries more than 80% of individuals with type 2 diabetes also suffer from obesity.[1] Other life threatening risks related to obesity are hypertension, dyslipidemia, coronary artery disease, cerebral vascular accident (CVA) and gall bladder disorders. It is recommended that moderate weight loss in obese diabetic patients can lower serum glucose and lessen the amount of insulin needed.[3] 5-10% weight loss in obese patients can reduce blood pressure in all individuals and can lessen the need for hypertension drugs in mild to moderate hypertensive patients.[4]
Although a life style change consisting of physical activity and dietary regime is the basic way to control and treat obesity, the result is often disappointing. Pharmacotherapy is usually reserved for patients with a BMI greater than 30 kg/m2 without complications or a BMI greater than 27 to 30 kg/m2 with concomitant weight-related complications. Pharmacotherapy is typically initiated if the patient has been unsuccessful in attaining their weight loss target after 6 months of lifestyle modification, but it must be used in conjunction with a program that includes dietary changes and physical activity.[5] Therefore, there is a demand for new weight reducing drugs to help diabetic patients lose weight.[6]
Topiramate is a highly controversial medication that has already been used to reduce weight.[7,8,9] topiramate, discovered in 1979 by Bruce E. Maryanoff and Joseph F. Gardoki, first prescribed as an anticonvulsant drug.[10] This drug can block voltage mediated sodium gates in the central nervous system and prevents repeated stimulation of neurons with an 80% oral bioavailability and a 20-30 h half life, most of the topiramate consumed is excreted by the body, unchanged in the urine.[9] This drug has also been investigated for use to treat alcoholism,[11] post-traumatic stress disorder (PTSD),[12] periventricular leukomalacia[13] and Binge eating disorder[14]
There have been several studies showing the weight reducing effect of topiramate.[10] The studies on humans demonstrated that amounts of weight loss from topiramate were related to the dose and duration of administration.[6,7,15,16,17] However, there is a need for more accurate and precise research on its effect on different ethnic groups and medical conditions.
The determination of an effective weight reducing medication would be helpful to combat the high prevalence of obesity and its complications. topiramate offers an effective possibility, but research is needed to gain information with a more global perspective. The aim of this study was to evaluate the effect of topiramate on weight loss in Iranian patients with type 2 diabetes.
MATERIALS AND METHODS
Study design and subjects
The subjects for this randomized, double-blind, placebo-controlled, parallel group study were recruited from the Institute of Endocrinology and Metabolism, Firouzgar Hospital, Tehran, Iran. The trial was from October 2008 to February 2010 (RCT code: IRCT201112036027N2) and was planned for 32 weeks, consisting of a 1-week run-off placebo phase, a 3-week titration phase, a 26-week maintenance phase, and a 2-week taper phase (See flow chart).
FLOW CHART.
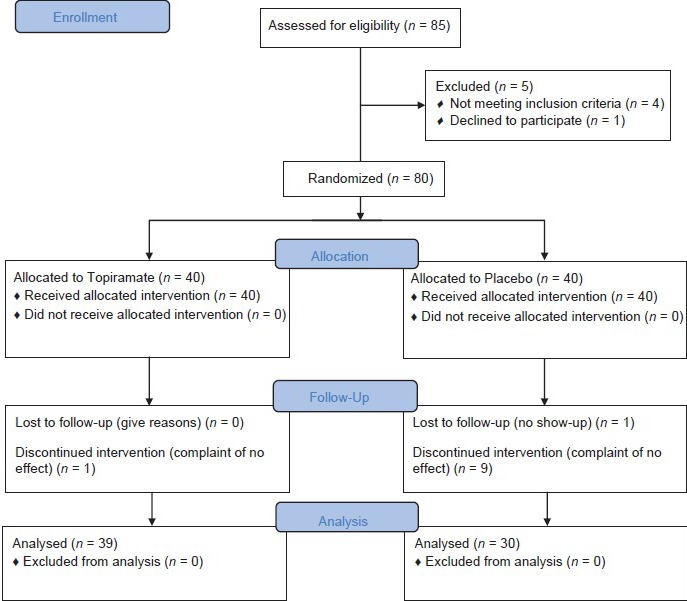
Consort flow diagram for the effect of topiramate on weight loss in Iranian patients with type two 2 diabetes
The sampling was made by stratified randomization (by age and gender) on patients who fulfilled our inclusion criteria. All individuals were referred to a single endocrinologist (blinded to drug administration) and the study was fully introduced to the participants (Also blinded to drug administration). Both topiramate and placebo were similar in size, shape and color and administered randomly by a pharmacist in the hospital which the study was taken place and the results were stored by their insurance code. The sample size was calculated at least 30 individuals in each group by “estimation of mean difference between two groups” formula according to of Rosenstock et al.[17] study on Base of BMI changes (α = 0.05, β = 0.8, μ1 = 0.8 ± 1.1 and μ2 = 2.1 ± 1.8). In our study, 85 individuals were included; however after starting the protocol, only 69 patients (21 male and 48 female) were assessed as intention to treat (ITT) population.
The criteria for participation in the study were considered as followed: Age 18-75 years; body mass index (BMI) between 27 and 50 kg/m2; a documented history of type 2 diabetes mellitus; glycosylated hemoglobin (HbA1c) less than 11%; fasting plasma glucose between 126 and 240 mg/dl; blood pressure (BP) less than 160/105 mmHg and a constant weight for at least 3 months (±3 kg).[17] The dose of hyper-lipidemic medication that had been stable for at least 3 months (the dose was to be maintained for the duration of the study). Female subjects of childbearing age were required to use an approved method of birth control.[17] Subjects with a history of central nervous system (CNS) related or psychiatric disorders, significant renal, hepatic, and thyroid diseases were excluded from the study any time after participation. All subjects participated in a non-pharmacologic lifestyle intervention program, designed and performed by the nutrition counselors of the Institute during the study. The emphasis of the program was a diet composed of low-salt (1,500 mg/day) with a maximum of 30% fat and an energy content that was 300 kcal less than the patient's daily energy. The goal population was stratified into different life-style and medication, then the samples were randomly selected split into two groups; one to receive the placebo and the other topiramate at a doses of 150 mg/day,[17,18] 100 mg each morning and 50 mg every evening. The 3-week titration phase began with administration of 25 mg topiramate once every morning to subjects assigned to that group. In the second week, topiramate was administered at 25 mg twice daily (50 mg/day). The dose was thereafter increased to 100 mg/day (50 mg in the morning and 50 mg in the evening). The maintenance phase begun in the 4th week with the dose of 150 mg/day. During the maintenance phase, the dose remained constant (placebo and 150 mg/day, divided in to twice daily doses as stated above). Finally the dose was tapered to75 mg/day in the first week and 25 mg/day in the second week up to either completion of or early withdrawal from the study. A follow-up evaluation was performed 2 weeks after the treatment was stopped.
Ethics
Before including any individual in our study, all subjects signed a consent form stating that they willing to participate in our study. All subjects could exit the trial whenever they want and no charges were defined for the participant. None of the information will be released individually and all participants were included as anonymous. Our study was approved by ethics committee of Hemmat Campus of Tehran University of Medical Sciences (formerly: Iran University of Medial Sciences) before initiating the research (Ethics code 501, date of approval: August 20, 2008)
Efficacy end points
The primary efficacy end point was the percent change in BMI at the end of the study. The secondary end points were changes in sitting systolic and diastolic BP; the proportion of subjects who achieved 5% or 10% weight loss (5% and 10% weight responders); the proportion of subjects who achieved a decrease of 5 or 10 mmHg in diastolic BP (5 and 10 mmHg diastolic BP responders) or systolic BP (5 and 10 mmHg systolic BP responders); changes in lipid profile (total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglycerides); and changes in glycosylated hemoglobin (HgA1c).
However, all patients had been warned about the drugs side effects (Parasthesia, lack of concentration, pruritus, insomnia and dizziness) and been advised to inform the endocrinologist. The participants would be excluded from the study if desired or the side effects was disabling.
Assesments
Weight, height and blood pressure measurements for each patient were taken according to the appropriate scales (Richter Inc., Germany). All the biochemical assays were carried out at the Institute of Endocrine and Metabolism laboratory (Firoozgar Hospital, Tehran, Iran). Total cholesterol, HDL and triglycerides were measured by photometric assay with intra- and inter-assay coefficients of variation less than 2% (Pars Azmoon Company; Iran).
Statistical analyses
All data were analyzed by SPSS for Windows version 16 (SPSS Inc., Illinois, USA) using statistical tests; Paired samples t-test (for within group analyses), Independent samples t-test (for between groups analysis) and Chi-square fisher exact test. Efficacy data were assessed in the intent-to-treat (ITT) population, defined as all subjects who were randomized, received at least one dose of study medication, and completed at least one efficacy measurement while on the treatment.
RESULT
Baseline characteristics
At the end of the study, 69 patients (21 male and 48 female) were assessed as intention to treat (ITT) population; 39 in the topiramate group and 30 in the placebo group. The mean age was 52.45 ± 8.57 years an d the mean weight at the time of the trial was 82.59 ± 13.40 kg.
Weight and BMI changes
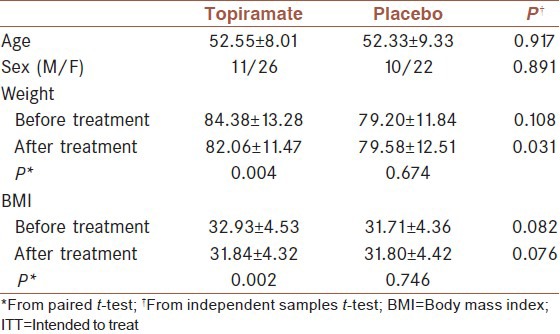
As seen in Table 1, mean weight and mean BMI reduced significantly in the topiramate group after treatment. Furthermore, mean weight of topiramate group was significantly lower than the placebo group after treatment.
Table 1.
Weight and BMI in ITT subjects, a comparison between drug and placebo groups; bolded P values are significant
Further analysis showed that the mean Δ weight (calculated from Δ W= weight after treatment – weight before treatment) was not significantly different between placebo and topiramate groups (5.18 ± 0.99 vs. 1.83 ± 0.50 kg, P = 0.523). Mean weight loss percentage (ΔW/weight before treatment) was also without significant difference (5.55 ± 1.06% vs. 3.40 ± 0.61%, P = 0.492). ΔBMI (calculated from: ΔBMI = BMI before treatment – BMI after treatment) was significantly higher in patients treated with topiramate (-1.08 ± 1.90 vs. +0.086 ± 1.05 kg/m², P = 0. 006). Also mean BMI loss percentage (calculated from: (ΔBMI/BMI before treatment) ×100) was significantly different between the active and placebo groups (-3.02 ± 5.78% vs. +0.32 ± 3.54%, P = 0.005); more information demonstrated in Figures 1 and 2.
Figure 1.
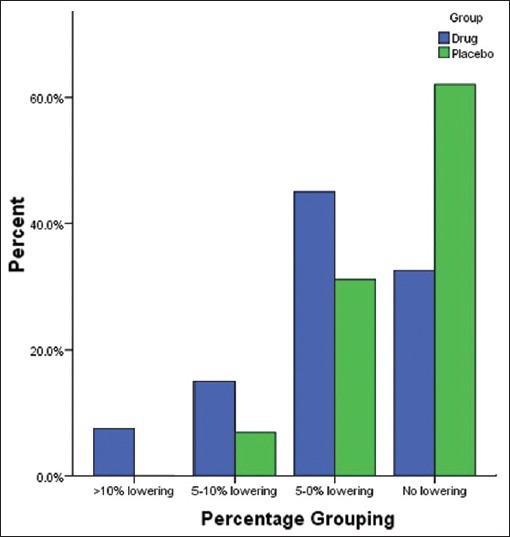
Proportion of patients achieving 0-5%, 5-10% and more than 10% weight loss by topiramate and placebo
Figure 2.
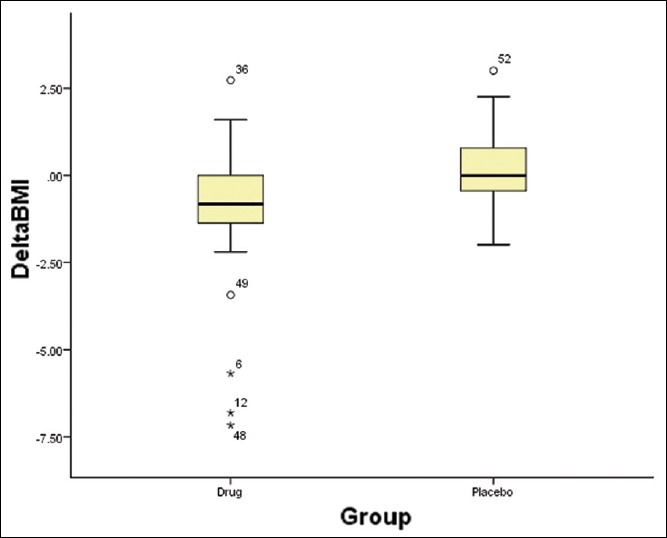
Box-plot of BMI reduction in topiramate and placebo groups; as stated, they have significant difference
Other diabetes markers
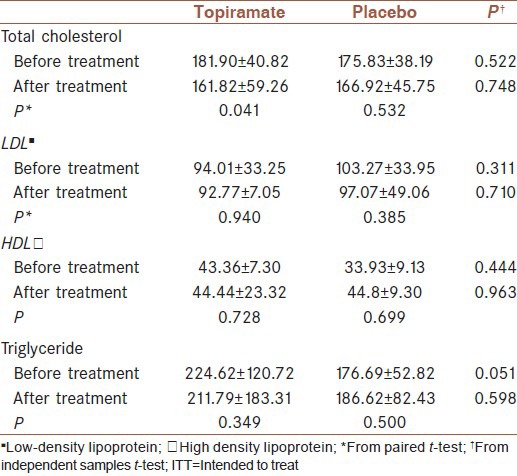
Systolic and diastolic blood pressure and hemoglobin A1C (HgA1C) levels were evaluated in all patients. Systolic blood pressure and HgA1C significantly decreased in patients treated with topiramate (P = 0.021 and P = 0.047, respectively). Other parameters did not differ significantly. Total cholesterol in the placebo group significantly decreased in the topiramate group after treatment (P = 0.048). Other data are classified in Tables 2 and 3 which demonstrates no significant difference in other parameters.
Table 2.
Blood pressure and hemoglobin A1C in ITT subjects, a comparison between drug and placebo groups; bolded P values are significant

Table 3.
Lipid profile in ITT subjects, a comparison between drug and placebo groups
Twenty-four patients in the topiramate group and nine cases in the placebo group had reported adverse effects. The most common of the side effects was paresthesia (12 cases in topiramate group and 3 in placebo group; P = 0.041) and followed by difficulty with concentration (8 in topiramate group and 2 in placebo group; P = 304). Other adverse effects were included pruritus, insomnia and dizziness (less than 2 cases). None of the patients were excluded from study due to these adverse effects.
DISCUSSION
Statistically, significant weight loss was achieved in obese type 2 diabetic subjects treated with topiramate in this study. This weight loss was accompanied by significant reduction in HbA1c. In different studies, it has been demonstrated that a modest reduction in body weight will considerably improve glycemic control in subjects with type 2 diabetes.[3] In our study, weight changes from baseline (>5%) were seen in 25% of subjects in the topiramate group compared with the placebo group (<5% of cases). This may account for improvement in HbA1c. All participants were matched for medication, diet and daily physical activity. Blood pressure and lipid profiles were predominantly normal at baseline. This may explain the relatively modest changes in these factors. Although the effect of topiramate on systolic blood pressure and cholesterol were statistically significant, triglyceride changes, that can be more dependent on body weight, did not differ significantly.
In the current study, the effect of topiramate was less compared with other studies that had used higher doses of topiramate for longer durations. Some studies suggest that topiramate can be more effective with longer treatment; hence, in subjects who did not show any persistent or adverse side effects, it could be used for longer periods.[16,19]
In a study conducted by Wilding et al., the mean decrease in body weight with topiramate 192 mg/day was 9.1% and 61% of these subjects lost at least 5% of their baseline body weight at week 60 of the treatment. Hence, there were no statistically significant differences in weight loss between the groups treated with doses of 256 and 192 mg/day.[16] Additional weight loss was observed in this study compared with our study; the difference could be attributed to the longer treatment duration, but the results are comparable at month 6 (near 5.5% weight loss). In another randomized placebo-controlled study, a total of 111 subjects were studied for 16 weeks, which demonstrated (2.5 vs. 6 kg, P < 0.001) weight loss and 0.4% vs. 0.7% lowering effect in HgA1C, concluding improvements in diabetic patients, however, the authors did not recommend it due to central nervous system and psychiatric adverse events.[17] Recently, combination of topiramate with phentermine has been evaluated in two big studies for weight loss which demonstrated near 10% weight loss and 0.3-0.7% reduction in HgA1C.[20,21]
Even more significantly, Eliasson et al. demonstrated a 6.6% weight loss with 9 months topiramate treatment in obese subjects with type 2 diabetes. Specifically, reduction in HbA1c in this study was comparable with the current study.[18]
The mechanisms underlying the effect of topiramate on lowering HbA1c and FBS of diabetic patients are not clear yet. Several studies have demonstrated whole-body insulin sensitivity following topiramate treatment although this would have been expected considering the over-all effect on glucose control. However, “a similar discrepancy between insulin-stimulated glucose uptake during a clamp and fasting glucose levels has also recently been shown in DM2 patients following 3% reduction in body weight”, shown in Eliasson et al. study.[18]
The most common adverse responses to topiramate were paresthesia and amnesia: Side effects that were realized early on in the study. Most of the patients stated that these effects are not much a problem and tried to comply with the study. These results were unique and have not been seen in any studies.[17,18,19]
The main limitations of this study were its short duration and the small sample size due to the non-co-operation state of some subjects. We recommend more studies with narrower inclusion criteria and larger sample size with different conditions with a long duration of follow-up in Iran and other middle to low income counties.
CONCLUSION
Treatment of obese diabetic patients with 150 mg/day topiramate can be suitable for near 5% weight loss. Topiramate may be effective in improving metabolic parameters associated with obesity and glycemic control in diabetes type two patients.
Footnotes
Source of Support: Iran University of Medical Science
Conflict of Interest: None declared.
REFERENCES
- 1.de Onis M, Blössner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257–64. doi: 10.3945/ajcn.2010.29786. [DOI] [PubMed] [Google Scholar]
- 2.Grandner MA, Patel NP, Perlis ML, Gehrman PR, Xie D, Sha D, et al. Obesity, diabetes, and exercise associated with sleep-related complaints in the American population. Z Gesundh Wiss. 2011;19:463–74. doi: 10.1007/s10389-011-0398-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Mangou A, Grammatikopoulou MG, Mirkopoulou D, Sailer N, Kotzamanidis C, Tsigga M. Associations between diet quality, health status and diabetic complications in patients with type 2 diabetes and comorbid obesity. Endocrinol Nutr. 2012;59:109–16. doi: 10.1016/j.endonu.2011.10.003. [DOI] [PubMed] [Google Scholar]
- 4.Tonstad S, Tykarski A, Weissgarten J, Ivleva A, Levy B, Kumar A, et al. Efficacy and safety of topiramate in the treatment of obese subjects with essential hypertension. Am J Cardiol. 2005;96:243–51. doi: 10.1016/j.amjcard.2005.03.053. [DOI] [PubMed] [Google Scholar]
- 5.Aronne LJ, Powell AG, Apovian CM. Emerging pharmacotherapy for obesity. Expert Opin Emerg Drugs. 2011;16:587–96. doi: 10.1517/14728214.2011.609168. [DOI] [PubMed] [Google Scholar]
- 6.Bray GA, Hollander P, Klein S, Kushner R, Levy B, Fitchet M, et al. A 6-month randomized, placebo-controlled, dose-ranging trial of topiramate for weight loss in obesity. Obes Res. 2003;11:722–33. doi: 10.1038/oby.2003.102. [DOI] [PubMed] [Google Scholar]
- 7.Richard D, Ferland J, Lalonde J, Samson P, Deshaies Y. Influence of topiramate in the regulation of energy balance. Nutrition. 2000;16:961–6. doi: 10.1016/s0899-9007(00)00452-4. [DOI] [PubMed] [Google Scholar]
- 8.Raskin P, Donofrio PD, Rosenthal NR, Hewitt DJ, Jordan DM, Xiang J, et al. CAPSS-141 Study Group. Topiramatevs placebo in painful diabetic neuropathy. Neurology. 2004;63:865–73. doi: 10.1212/01.wnl.0000137341.89781.14. [DOI] [PubMed] [Google Scholar]
- 9.Antel J, Hebebrand J. Weight-reducing side effects of the antiepileptic agents topiramate and zonisamide. HandbExpPharmacol. 2012;209:433–66. doi: 10.1007/978-3-642-24716-3_20. [DOI] [PubMed] [Google Scholar]
- 10.Maryanoff BE, Costanzo MJ, Nortey SO, Greco MN, Shank RP, Schupsky JJ, et al. Structure-activity studies on anticonvulsant sugar sulfamates related to topiramate. Enhanced potency with cyclic sulfate derivatives. J Med Chem. 1998;41:1315–43. doi: 10.1021/jm970790w. [DOI] [PubMed] [Google Scholar]
- 11.Flórez G, Saiz PA, García-Portilla P, Alvarez S, Nogueiras L, Bobes J. Topiramate for the treatment of alcohol dependence: Comparison with naltrexone. Eur Addict Res. 2011;17:29–36. doi: 10.1159/000320471. [DOI] [PubMed] [Google Scholar]
- 12.Berlant J, van Kammen DP. Open-label topiramate as primary or adjunctive therapy in chronic civilian posttraumatic stress disorder: A preliminary report. J Clin Psychiatry. 2002;63:15–20. doi: 10.4088/jcp.v63n0104. [DOI] [PubMed] [Google Scholar]
- 13.Follett PL, Deng W, Dai W, Talos DM, Massillon LJ, Rosenberg PA, et al. Glutamate receptor-mediated oligodendrocyte toxicity in periventricular leukomalacia: A protective role for topiramate. J Neurosci. 2004;24:4412–20. doi: 10.1523/JNEUROSCI.0477-04.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Claudino AM, de Oliveira IR, Appolinario JC, Cordás TA, Duchesne M, Sichieri R, et al. Double-blind, randomized, placebo-controlled trial of topiramate plus cognitive-behavior therapy in binge-eating disorder. J Clin Psychiatry. 2007;68:1324–32. doi: 10.4088/jcp.v68n0901. [DOI] [PubMed] [Google Scholar]
- 15.Verrotti A, Scaparrotta A, Agostinelli S, Di Pillo S, Chiarelli F, Grosso S. Topiramate-induced weight loss: A review. Epilepsy Res. 2011;95:189–99. doi: 10.1016/j.eplepsyres.2011.05.014. [DOI] [PubMed] [Google Scholar]
- 16.Wilding J, Van Gaal L, Rissanen A, Vercruysse F, Fitchet M OBES-002 Study Group. A randomized double-blind placebo-controlled study of the long-term efficacy and safety of topiramate in the treatment of obese subjects. Int J ObesRelatMetabDisord. 2004;28:1399–410. doi: 10.1038/sj.ijo.0802783. [DOI] [PubMed] [Google Scholar]
- 17.Rosenstock J, Hollander P, Gadde KM, Sun X, Strauss R, Leung A OBD-202 Study Group. A randomized, double-blind, placebo-controlled, multicenter study to assess the efficacy and safety of topiramate controlled release in the treatment of obese type 2 diabetic patients. Diabetes Care. 2007;30:1480–6. doi: 10.2337/dc06-2001. [DOI] [PubMed] [Google Scholar]
- 18.Ioannides-Demos LL, Piccenna L, McNeil JJ. Pharmacotherapies for obesity: Past, current, and future therapies. J Obes 2011. 2011 doi: 10.1155/2011/179674. 179674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Eliasson B, Gudbjörnsdottir S, Cederholm J, Liang Y, Vercruysse F, Smith U. Weight loss and metabolic effects of topiramate in overweight and obese type 2 diabetic patients: Randomized double-blind placebo-controlled trial. Int J Obes (Lond) 2007;31:1140–7. doi: 10.1038/sj.ijo.0803548. [DOI] [PubMed] [Google Scholar]
- 20.Garvey WT, Ryan DH, Look M, Gadde KM, Allison DB, Peterson CA, et al. Two-year sustained weight loss and metabolic benefits with controlled-release phentermine/topiramate in obese and overweight adults (SEQUEL): A randomized, placebo-controlled, phase 3 extension study. Am J ClinNutr. 2012;95:297–308. doi: 10.3945/ajcn.111.024927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Gadde KM, Allison DB, Ryan DH, Peterson CA, Troupin B, Schwiers ML, et al. Effects of low-dose, controlled-release, phentermine plus topiramate combination on weight and associated comorbidities in overweight and obese adults (CONQUER): Arandomised, placebo-controlled, phase 3 trial. Lancet. 2011;377:1341–52. doi: 10.1016/S0140-6736(11)60205-5. [DOI] [PubMed] [Google Scholar]