

Abstract
Background:
Diabetes Mellitus is a metabolic disorder characterized by abnormal lipid and glucose metabolism. Various modes of adjuvant therapy have been advocated to ameliorate insulin resistance.
Aim:
This study was intended to assess the effects of antioxidants; alpha lipoic acid (ALA), omega 3 fatty acid and vitamin E on parameters of insulin sensitivity (blood glucose and HbA1c) in patients of type 2 diabetes mellitus with documented insulin resistance.
Subjects and Methods:
It was a prospective, randomized, double blind, placebo controlled, single centered study. 104 patients with type 2 diabetes mellitus with insulin resistance were recruited. They were given ALA, omega 3 fatty acid, vitamin E or placebo. Fasting blood glucose and HbA1c were measured at first visit (V1) and after 90 days (V2). Statistical analysis was carried out by paired t-test by using SPSS software version 11 (SPSS, Chicago, USA).
Results:
Analysis of baseline (V1) vs. end of treatment period (V2) parameters, showed significant decrease in HbA1c in the three treatment group. We also observed decrease in fasting blood glucose in the three treatment group but it was not statistically significant (Gr. I = 0.51, Gr. II = 0.05, Gr. III = 0.22, Gr. IV = 0.88).
Conclusion:
ALA, Omega 3 fatty acid and vitamin E can be used as add on therapy in patients with type 2 diabetes mellitus to improve insulin sensitivity and lipid metabolism.
Keywords: Alpha lipoic acid, Insulin resistance, Omega 3 fatty acid, Vitamin E
Introduction
The worldwide prevalence of Diabetes Mellitus (DM) has risen dramatically over the past two decades, from an estimated 30 million cases in 1985 to 177 million in 2000. Based on current trends, more than 360 million individuals will have diabetes by the year 2030. Although the prevalence of both type 1 and type 2 DM is increasing worldwide, the prevalence of type 2 DM is rising much more rapidly because of increasing obesity and reduced physical activity.[1]
Presently, India has the largest number of people with diabetes in the world as stated in the findings of the International Diabetes Federation, 2007. India clearly leads this list with 40.9 million diabetics. In India, this figure is about to rise to 60.9 million by 2020.[2]
Impaired insulin secretion and insulin resistance are the basic pathophysiological mechanisms responsible for diabetes mellitus. There is well established association between oxidative stress and insulin resistance. The most probable mechanism proposed is when glucose and free fatty acid (FFA) increase in diabetes; they cause oxidative stress along with activation of stress-sensitive signalling pathways. Activation of these pathways, in turn, worsens both insulin action and secretion leading to overt type 2 DM.
Currently insulin and oral antidiabetic agents form the mainstay of treatment in addition to diet and exercise, but these agents are associated with major limitations like:
Hypoglycemic episodes
Inability to achieve normoglycemia by themselves. Even in properly selected patients, sulfonylureas may fail (primary failure: 5-28%) or become ineffective after few months or years (secondary failure: 5-10%) due to progression of insulin resistance or desensitization of receptors.[3]
Inability to prevent premature atherosclerosis due to hyperinsulinemia in case of insulin resistance.[3]
The major limitation in the current therapy of DM is the lack of alternatives to treat patients with insulin resistance.[4] These patients require very high doses of exogenous insulin and even this has limited effect in improving the quality of life. Various animal studies and clinical trials have favored the use of anti-oxidants in such patients. Anti-oxidants have been shown to improve not only HbA1c levels but also glucose uptake in the resistant tissue.[5]
Various clinical trials have been performed to assess the effects of antioxidants such as omega 3 fatty acid,[6] alfa lipoic acid and vitamin E on insulin sensitivity. However the above trials are limited by small sample size and none of the trials compared the effects of two or more antioxidants at the same time. Therefore the present study was planned to assess comparative effects of three different antioxidants, on insulin sensitivity reflected by parameters like blood glucose and HbA1c in patients of type 2 diabetes mellitus.
HbA1c expressed, as the percentage of adult hemoglobin that is glycated, is the most widely used measure to assess glycemic control over the past 90 days. Maintaining HbA1c levels in the normal range have been shown to reduce long-term complications of diabetes. HbA1c estimation is recommended to determine whether treatment is adequate and also to guide adjustment in drug doses.[7] The aim of the study is to assess and compare the effects of antioxidants, viz. vitamin E, omega 3 fatty acid and alpha lipoic acid on endogenous insulin sensitivity (reflected by parameters like blood glucose and HbA1c) in patients of type 2 Diabetes Mellitus.
Subjects and Methods
The randomized double-blind, placebo-controlled, prospective, single centre study was conducted in a tertiary care hospital where patients attending the medicine outpatient department/diabetes clinic were recruited for the study. A synopsis of the study protocol was submitted to the Institutional Ethics committee and approval was obtained. Written informed consent was taken from all the participants.
Inclusion criteria
Patients of either sex in the age group of 21-65 years, who are previously diagnosed cases of type 2 diabetes mellitus, were considered. Their fasting blood sugar values during screening were between 110-250 mg/dl. A diagnosis of insulin resistance was made on the basis of NCEP: ATPIII 2001 Criteria for the Metabolic Syndrome.
Exclusion criteria
Patient with type 2 diabetes mellitus with fasting blood glucose >250 mg/dl or patients who are currently on insulin therapy
Patients taking any long term medication except anti-diabetic
Patients with major illness
Patients received both Tab. Metformin and Tab. Glimepiride as oral hypoglycaemic therapy. They were receiving the same oral hypoglycemic medications for at least 6 months. Only vegetarian volunteers were included to avoid any bias.
The patients were categorized randomly into 4 groups.
Group I (n = 25) → alpha lipoic Acid group
Group II (n = 25) → omega 3 fatty acid group
Group III (n = 25) → Vitamin E group
Group IV (n = 25) → Placebo group
After patients’ randomization, they were given study medication (alpha lipoic acid, omega 3 fatty acid, Vitamin E or Placebo) for 90 days.
Study drugs and doses
Alpha- lipoic acid 300 mg soft gelatin capsules [Batch number-K117109; expiry date-Jun 2010].
Ecosapentaenoic acid 180 mg + Docosahexaenoic acid 120 mg soft gelatin capsules [Batch number-G0562808; expiry date-Nov 2010].
Vitamin E 400 mg soft gelatin capsules [Batch number-G0361908; expiry date-Oct 2010].
Placebo soft gelatin capsules [Batch number-DCW3701501; expiry date-Dec 2010].
Following parameters were recorded at each visit.
Visit 1 (Day 0)
General examination including height, weight (BMI), waist circumference and blood pressure.
Blood (Fasting) à Glucose, HbA1c
Visit 2 (Day 90)
General examination including height, weight (BMI), waist circumference and blood pressure.
Blood (Fasting) à Glucose, HbA1c
Adverse drug reaction monitoring
Serum Glucose (Fasting)
A fasting sample of blood was collected in a fluoride bulb at each visit for estimation of serum glucose. Blood was centrifuged to separate plasma. The measurement was done by the glucose-oxidase method.
Blood HbA1c
HbA1c was determined by using the cation-exchange resin method.[7]
Statistical analysis was carried out by paired t-test by using SPSS software version 11 (Chicago, USA).
Results
All the four groups were statistically comparable [Table 1]. Though there was decrease in blood glucose level in treatment group as compared to placebo group, the difference was not statistically significant [Table 2]. There was a statistically significant decrease in HbA1C levels in Group I (alpha lipoic Acid), Group II (omega 3 fatty acid) and Group III (vitamin E) (Gr. I = 0.02, Gr. II = 0.03, Gr. III = 0.09) at visit 2 compared to visit 1. Group IV (Placebo) (Gr. IV = 0.21) showed a decrease which was not statistically significant. Maximum decrease was found with omega 3 fatty acid. We also got decrease in placebo group but we believe that this may be because of oral hypoglycaemic drugs [Table 3].
Table 1.
Group wise demographic data mean (SD)
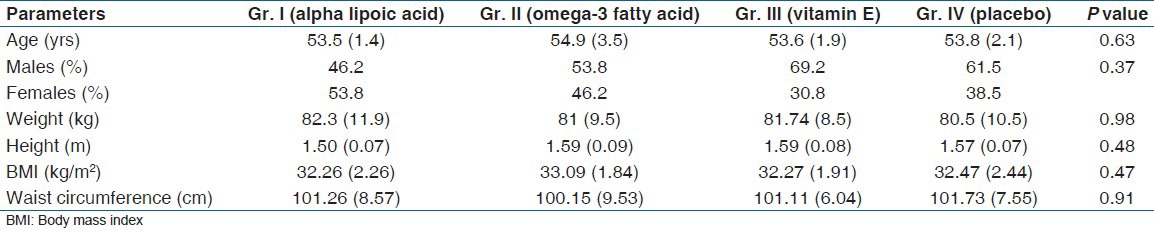
Table 2.
Change in blood glucose levels in mg/dl (fasting) within the groups from V1 to V2 mean (SD)

Table 3.
Change in serum HbA1c as percentage of the total Hb within the groups from V1 to V2 mean (SD)

Discussion
In the present study the effects of three different antioxidants viz. alpha lipoic acid, omega 3 fatty acid and vitamin E in patients with type 2 DM were evaluated. The present study was a randomized, double blind, placebo controlled trial. Parameters which either directly or indirectly measures endogenous insulin sensitivity were used such as, blood glucose and HbA1c.
Subjects were divided into 4 groups depending upon the medication given. Group I (alpha lipoic Acid), Group II (omega 3 fatty acid) and Group III (vitamin E) showed a reduction in fasting blood glucose levels but this was not statistically significant. Group IV (Placebo) showed an increase in mean values of fasting blood glucose [Table 2].
There was a statistically significant decrease in HbA1C levels in Group I (alpha lipoic Acid), Group II (omega 3 fatty acid) and Group III (vitamin E) at visit 2 compared to visit 1. Group IV (Placebo) also showed a decrease but it was not statistically significant [Table 3]. Though the reduction in blood glucose levels and HbA1C was statistically significant in all the groups, the maximum reduction was found with omega 3 fatty acid. Thus it was the best antioxidant which showed the maximum improvement in type II diabetes mellitus.
Similar results were obtained by Pooya SH and colleagues who studied the effect of omega-3 fatty acids on the concentration of fasting glucose and HbA1C in diabetic patients. They conducted a randomized double-blind, placebo-controlled clinical trial on 81 patients with type 2 DM. Each subject received three capsules of omega-3 fatty acids or a placebo every day for a period of 2 months. They found that due to omega-3 fatty acid supplementation, HbA1C decreased by 0.75% in the treatment group and increased by 0.26% in the control group. However, the changes in fasting blood sugar levels were not significant.
In order to find outcome of vitamin E supplementation, G Paolisso, investigated the potential metabolic benefits deriving from daily vitamin E administration in type II diabetic patients. They found that long term vitamin E administration reduced plasma glucose, triglycerides, FFAs, total cholesterol, low-density lipoprotein cholesterol, and apoprotein B levels but did not affect beta-cell response to glucose. HbA1c levels were also significantly lowered.
Role of antioxidants
It has long been suspected, but only recently demonstrated, that the consumption of fruits and vegetables rich in vitamin and other antioxidants can increase overall antioxidant status.[8] In studies of humans and rodents, dietary supplementation with antioxidants is associated with decreased risk of type 2 DM and induces changes that could be beneficial in reducing insulin resistance and protecting vascular endothelium.[9] Primary among these are vitamin E (alpha-tocopherol), Alpha lipoic acid (thioctic acid) and omega 3 fatty acid.[10]
In the GK rat, a model for type 2 DM, vitamin E supplementation significantly improved glycemic control, possibly by minimizing free radical damage to the pancreatic β-cells.[11,12] Another study using the obese Zucker rat, an animal that exhibits many of the features of type 2 DM showed improvements in glucose metabolism and insulin action by addition of vitamin E that was mediated by a reduction in oxidative stress. They found that glucose-stimulated hyper-insulinemia and lipid peroxidation in the obese Zucker rat could be significantly reduced with dietary vitamin E.[13]
Alpha lipoic acid, an essential cofactor of alpha-oxoacid dehydrogenase complexes, is also a potent lipophilic free radical scavenger. Alpha lipoic acid was found to increase glucose transport in muscle cells in culture by stimulating translocation of GLUT4 from internal pools to the plasma membrane.[14] In cultured adipocytes, treatment with ALA protected the insulin receptor from oxidative damage, maintaining its functional integrity. Konrad, et al.,[14] used cell cultures consisting of different isoforms of p38 MAPK (p38 mitogen-activated protein kinase) in L6 GLUT4 myc myotubes. They demonstrated that Alpha lipoic acid was able to increase the plasma membrane content of GLUT4 and stimulate glucose uptake in L6 GLUT4 myc myotubes to a similar extent as insulin. They further suggested that alpha lipoic acid stimulates glucose uptake by translocating and regulating the intrinsic activity of GLUT4. They concluded that alpha lipoic acid enhanced glucose uptake and GLUT4 translocation in L6 myotubes, mimicking insulin action.
Ingestion of PUFA-rich diets, particularly enriched in omega 3 fatty acid, has been shown to have anti-obesity effects[15] and to facilitate insulin action[16] through a number of metabolic effects. Ingestion of both omega 6 and omega 3 fatty acid has been demonstrated to suppress hepatic lipogenesis,[17] reduce the hepatic output of triglycerides, enhance ketogenesis,[18] and induce fatty acid oxidation in both the liver and the skeletal muscle.[19] Insulin sensitivity may improve as a result of the effects of fatty acid intake on membrane fluidity.[20] The improvement in glucose uptake after membrane enrichment with PUFA is apparently related to an increase in the residency time of GLUT4 in the plasma membrane, which leads to an expansion of the intracellular pool of glucose-6-phosphate[20] and to increased skeletal muscle glycogen synthesis.
The results of this study demonstrate that antioxidants alpha lipoic acid, omega 3 fatty acid and vitamin E showed encouraging decrease in blood glucose and HbA1c with no adverse effect and these antioxidants may be used in patients with type 2 diabetes mellitus. Depending upon the cost benefit analysis we found vitamin E to be the most cost effective even though the maximum improvement in blood glucose and HbA1c was with omega 3 fatty acid.
Summary and Conclusions
Currently many drugs are used to treat type 2 diabetes mellitus. Most of these drugs either improve the insulin secretion by the pancreas or decrease the secretion of glucose by the liver. However the basic pathology of insulin resistance goes unanswered. Antioxidants by their unique mechanisms of action can be used to tackle this problem in addition to anti-diabetic drugs in any of the groups.
The results of this study demonstrate that antioxidants alpha lipoic acid, omega 3 fatty acid and vitamin E showed encouraging decrease in blood glucose and HbA1c with no adverse effect and these antioxidants may be used in patients with type 2 diabetes mellitus. However further study with larger sample size and longer duration of treatment is required to definitely establish the role of anti-oxidants in patients with type 2 diabetes mellitus. Depending upon the cost benefit analysis we found vitamin E to be the most cost effective even though the maximum improvement in blood glucose and HbA1c was with omega 3 fatty acid. But most importantly, since the antioxidants differed in their effects on parameters of insulin sensitivity, combining these drugs might prove as an attractive option in patients with type 2 diabetes mellitus.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Alvin C. Powers, Kasper D. L, Brounwal E, Fauci AS. 16th ed. New York: Mc Graw Hill Publishers; 2005. Harrisons Principle of Internal Medicine; pp. 2152–79. [Google Scholar]
- 2.Park K. 18th ed. Jabalpur: Bhanot Publishers; 2006. Text. Book of Preventive and Social Medicine; pp. 341–45. [Google Scholar]
- 3.Jacob S, Ruus P, Hermann R, Tritschler J, Maerker E, Renn W, et al. Oral administration of RAC-Alpha lipoic Acid modulates insulin sensitivity in patients with type 2 diabetes mellitus: A placebo control pilot trial. Free Radic Bio Med. 1999;27:309–41. doi: 10.1016/s0891-5849(99)00089-1. [DOI] [PubMed] [Google Scholar]
- 4.Lovejoy JC. The influence of dietary fat on insulin resistance. Curr Diab Rep. 2002;2:435–40. doi: 10.1007/s11892-002-0098-y. [DOI] [PubMed] [Google Scholar]
- 5.Montonen J, Knekt P, Järvinen R, Reunanen A. Dietary antioxidants intake and risk of type II diabetes. Diabetes Care. 2004;27:362–6. doi: 10.2337/diacare.27.2.362. [DOI] [PubMed] [Google Scholar]
- 6.Shidfar F, Keshavarz A, Hosseyni S, Ameri A, Yarahmadi S. Effects of omega-3 fatty acid supplements on serum lipids, apolipoproteins and malondialdehyde in type 2 diabetes patients. East Mediterr Health J. 2008;14:305–13. [PubMed] [Google Scholar]
- 7.Nathan DM, Singer DE, Hurxthal K, Goodson JD. The clinical information value of the glycosylated haemoglobin assay. N Eng J Med. 1984;310:341–6. doi: 10.1056/NEJM198402093100602. [DOI] [PubMed] [Google Scholar]
- 8.Cao G, Booth SL, Sadowski JA, Prior RL. Increase in human plasma antioxidant capacity after consumption of controlled diets high in fruits and vegetables. Am J Clin Nutr. 1998;68:1081–7. doi: 10.1093/ajcn/68.5.1081. [DOI] [PubMed] [Google Scholar]
- 9.Paolisso G, Esposito R, D’Alessio MA, Barbieri M. Primary and secondary prevention of atherosclerosis: Is there a role for antioxidants? Diabetes Metab. 1999;25:298–306. [PubMed] [Google Scholar]
- 10.Ruhe RC, McDonald RB. Use of antioxidant nutrients in the prevention and treatment of type 2 diabetes. J Am Coll Nutr. 2001;20:363S–369S. doi: 10.1080/07315724.2001.10719169. discussion 381S-3S. [DOI] [PubMed] [Google Scholar]
- 11.Ihara Y, Toyokuni S, Uchida K, Odaka H, Tanaka T, Ikeda H, et al. Hyperglycemia causes oxidative stress in pancreatic β cells of GK rats, a model of type 2 diabetes. Diabetes. 1999;48:927–32. doi: 10.2337/diabetes.48.4.927. [DOI] [PubMed] [Google Scholar]
- 12.Ihara Y, Yamada Y, Toyokuni S, Miyawaki K, Ban N, Adachi T, et al. Antioxidant alpha tocopherol ameliorates glycemic control of GK rats, a model of type 2 diabetes. FEBS Lett. 2000;473:24–6. doi: 10.1016/s0014-5793(00)01489-7. [DOI] [PubMed] [Google Scholar]
- 13.Laight DW, Desai KM, Gopaul NK, Anggård EE, Carrier MJ. F2-isoprostane evidence of oxidative stress in the insulin resistant, obese Zucker rat: Effects of vitamin E. Eur J Pharmacol. 1999;377:89–92. doi: 10.1016/s0014-2999(99)00407-0. [DOI] [PubMed] [Google Scholar]
- 14.Konrad D, Somwar R, Sweeney G, Yaworsky K, Hayashi M, Ramlal T, et al. The antihyperglycemic drug alpha lipoic Acid stimulates glucose uptake via both GLUT4 translocation and GLUT4 activation: Potential role of p38 mitogen activated protein kinase in GLUT4 activation. Diabetes. 2001;50:1464–71. doi: 10.2337/diabetes.50.6.1464. [DOI] [PubMed] [Google Scholar]
- 15.Mori TA, Vandongen R, Masarei JR, Rouse IL, Dunbar D. Comparison of diets supplemented with fish oil or olive oil on plasma lipoproteins in insulin dependent diabetics. Metabolism. 1991;40:241–6. doi: 10.1016/0026-0495(91)90104-5. [DOI] [PubMed] [Google Scholar]
- 16.Jump DB, Clarke SD. Regulation of gene expression by dietary fat. Annu Rev Nutr. 1999;19:63–90. doi: 10.1146/annurev.nutr.19.1.63. [DOI] [PubMed] [Google Scholar]
- 17.Berge RK, Madsen L, Vaagenes H. Hypolipidemic 3-thia fatty acid: Fatty acid oxidation and ketogenesis in rat liver under proliferation of mitochondria and peroxisomes. Adv Exp Med Biol. 1999;466:125–32. [PubMed] [Google Scholar]
- 18.Thomassen MS, Christiansen EN, Norum KR. Characterization of the stimulatory effect of high fat diets on peroxisomal beta oxidation in rat liver. Biochem J. 1982;206:195–202. doi: 10.1042/bj2060195. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Podolin DA, Gayles EC, Wei Y, Thresher JS, Pagliassotti MJ. Menhaden. Oil prevents but does not reverse sucrose induced insulin resistance in rats. Am J Physiol. 1998;274:840–8. doi: 10.1152/ajpregu.1998.274.3.R840. [DOI] [PubMed] [Google Scholar]
- 20.Evans JL, Goldfine ID, Maddux BA, Grodsky GM. Are oxidative stress-activated signaling pathways mediators of insulin resistance and beta-cell dysfunction? Diabetes. 2003;52:1–8. doi: 10.2337/diabetes.52.1.1. [DOI] [PubMed] [Google Scholar]