

Abstract
Background:
To assess the prevalence of food insecurity and associated factors among rural households in north-east of Iran.
Methods:
In this cross-sectional study, a total of 4647 rural households (18,061 persons) were studied in Neyshabur, a city in north-east of Iran. The Iranian version of the Six-Item Short questionnaire of Household Food Security Scale was used to measure food insecurity. Logistic regression model was used to estimate odds ratios (OR) and 95% confidence intervals (CI).
Results:
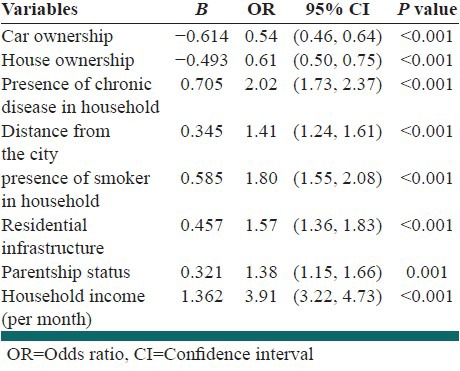
Total prevalence of food insecurity in this study was 40.9% (95% CI 39.49-42.31). Backward Multivariate Logistic Regression model showed that OR of food insecurity increased with: The presence of chronic disease in household in comparison the absence (OR = 2.02), the rural distance >30 km from the city in comparison the distance ≤30 km (OR = 1.41), the presence of smoker in household in comparison the absence (OR = 1.8), the residential infrastructure of household ≤50 m2 in comparison the >50 m2 (OR = 1.57), the presence of single parent in comparison the presence of both parents at home (OR = 1.38) and the household income (per month) <4,000,000 Rial in comparison the ≥4,000,000 Rial (OR = 3.91). But OR of food insecurity decreased with having a car in family in comparison not having (OR = 0.54) and the family having a house in comparison not having (OR = 0.61).
Conclusions:
According to results of this study, food insecurity is prevalent among rural households of Neyshabur, so it is an important public health problem in this region.
Keywords: Food insecurity, Iran, prevalence, rural households
INTRODUCTION
Food security exists when in a society all people at all times have enough food for an active, healthy life.[1] In contrast, food insecurity exists when food is not easily accessible and households have difficulty securing adequate food.[2] Food insecurity has emerged as a global crisis following the global economic meltdown.[3] Over the past two decades, food insecurity has increasingly been recognized as a serious public health problem in the developed world.[4] In USA, an estimated 17.4 million households, or 14.7% of all households, experienced food insecurity in 2009[5] and according to the 2012 report of the Food and Agriculture Organization (FAO) on the state of food insecurity in the world, about 870 million people are estimated to have been undernourished (in terms of dietary energy supply) in the period 2010-12.[2] Some surveys have found variation in the prevalence of food insecurity across Iran. For example, in Sharafkhani, Dastgiri, Hakim, and Karam Soltani studies, prevalence rates were 59.6%, 36.3%, 37.6%, and 30.5%.[6,7,8,9] However, there is little published data that provides insights regarding the extent and severity of food insecurity among the rural households in Iran. Some studies have shown that there is an association between household food insecurity and some factors. In Sharafkhani’ study was observed that distance from the city, number of centers that provides food, residential infrastructure, family size, and the presence of both parents are important factors on household's food insecurity status.[10] In Furness’ study that conducted in Los Angeles observed that income, having children in the household, and past homelessness were influential factors on food insecurity.[11] The objective of this study was to assess the prevalence of food insecurity and associated factors among rural households in north-east of Iran (Neyshabur).
METHODS
Participants
In this cross-sectional study, a total of 5000 rural households were selected in Neyshabur (a city in north-east of Iran) using simple random sampling. 353 households were excluded from the study, because of disagreement to contribute in study. Therefore, 4647 questionnaires were analyzed (response rate = 92.94%). The data were collected between April and June 2011, in the villages of Neyshabur. All participating households provided informed consent after being acquainted with the purpose of study. The approval of this research was obtained from the research committee of the Neyshabur University of Medical Sciences.
Procedure and study instrument
In this study, questionnaires have been filled via a face-to-face interview with responsible for household nutrition by trained persons (rural health volunteers), and for enhance accuracy; all participating households were informed that their responses would remain confidential. The Iranian version of the Six-Item Short questionnaire of Household Food Security Scale was used to measure food insecurity. This questionnaire was validated in Iran by Dastgiri.[12] This questionnaire contains six-items from the food security: (1) In the last 12 months, did you or any other in your household ever have to cut the size of your meals or skip meals entirely because there was not enough money for food? (2) If yes, how often did this happen? (3) In the last 12 months, did you ever eat less than you felt you should because there was not enough money to buy food? (4) In the last 12 months, were you ever hungry, but did not eat because you could not afford enough food? (5) The food that I/we bought just did not last, and I/we did not have money to get more. Was this often, sometimes, or never true for you or the other members of your household in the last 12 months? (6) I/we could not afford to eat balanced meals. Was this often, sometimes, or never true for you or the other members of your household in the last 12 months? Households were classified as “food-insecure” if the respondent answered affirmatively to two or more of the six household food security questions. “Almost every” and “some months” were considered affirmative responses to Question 2. “Often” and “sometimes” were considered affirmative responses to Questions 5 and 6.[13]
Dependent and independent variables
Food insecurity was considered as dependent variable. The other data collected, included, family size (≤3 vs. >3 persons), education years of household supervisor (<12 year vs. ≥12 year), age of household supervisor (≤50 year vs. >50 year), presence of children at home (no vs. yes), car ownership (no vs. yes), house ownership (tenant vs. private house), presence of chronic disease in household (no vs. yes), presence of smoker in household (no vs. yes), distance from the city (≤30 km vs. >30 km), number of places that provides food (≥1 vs. 0), residential infrastructure (≤50 km vs. >50 km), parentship status (two parents vs. single parent), and household income per month (≥4,000,000 Rial vs. <4,000,000 Rial) as independent variables.
Statistical analyses
The information collected was analyzed with the SPSS16.0 (SPSS Inc, Chicago, IL) software. Descriptive analyses performed including, frequencies, percentages, ranges, means, and standard deviations (SD). One-way analysis of variance (ANOVA) test was used in order to compare different status of food security (High or marginal Food Security (HFS), Low Food Security (LFS), and Very Low Food Security (VLFS)) according to household income (per month) and Tukey's Post-Hoc test was used in order to compare HFS, LFS, and VLFS two by two. Logistic regression model was used to investigate the relation between food insecurity and other variables. In this study, the Hosmer and Lemeshow goodness-of-fit test was used to test the model fit. We reported odds ratio (OR) with 95% confidence interval (CI). Various factors tested to have an association with food insecurity with P < 0.05.
RESULTS
The characteristics of study households are shown in Table 1. The family size of 55.7% households was more than three persons (range 1-15). The mean age of household supervisors was 47.2 ± 16.74 year (range 16-100 year). Total prevalence of food insecurity in the study population was 40.9% (95% CI 39.49-42.31). Of 4647 households, 704 (15.15%) households had VLFS, 1196 (25.74%) households had LFS, and 2747 (59.1%) households had HFS. One-way ANOVA test showed that average per month income according to household food security status (HFS, LFS, and VLFS) was significantly different (P < 0.05). However, after use of Tukey's Post-Hoc test observed average per month income was not significantly different between LFS and VLFS. In this study, after the use of Univariate logistic regression model observed that there was significant relation between independent variables such as education level of household supervisor, age of household supervisor, car ownership, house ownership, presence of chronic disease in household, presence of smoker in household, distance from the city, residential infrastructure, parentship status, and household income (per month). While variables such as family size, presence of children at home, and number of places that provide food had did not have a significant relation with food insecurity status [Table 2]. Table 3 illustrates the results of Backward Multivariate Logistic Regression model, it is apparent that OR of food insecurity increased with: The presence of chronic disease in household in comparison the absence, the rural distance upper than 30 km from the city in comparison the distance ≤30 km, the presence of smoker in household in comparison the absence, the residential infrastructure of household ≤50 m2 in comparison the >50 m2, the presence of single parent in comparison the presence of both parents at home and the household income (per month) lower than 4,000,000 Rial in comparison the ≥4,000,000 Rial. But, OR of food insecurity decreased with having a car in family in comparison not having and the family having a house in comparison not having.
Table 1.
Characteristics of study households (n=4647)
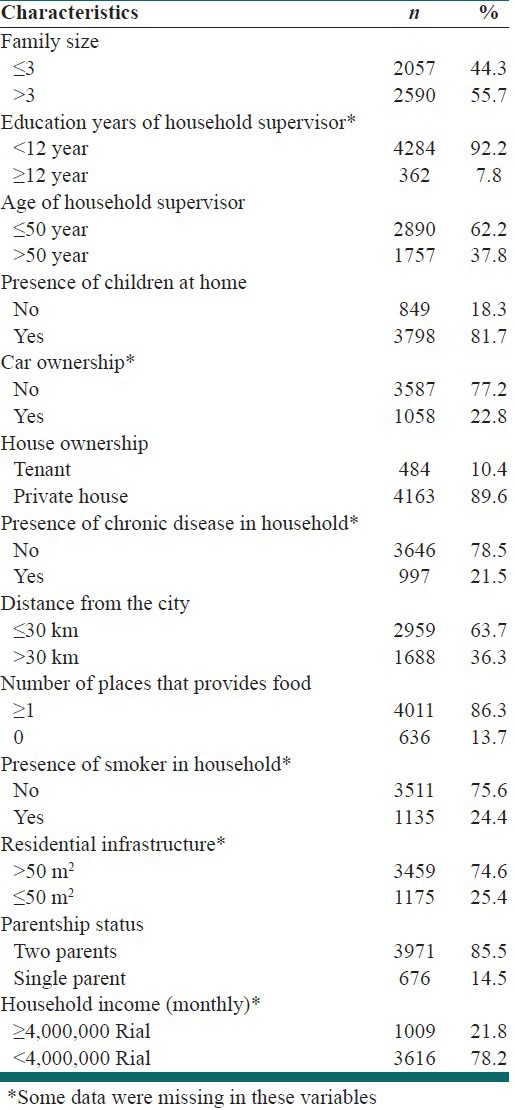
Table 2.
Odds ratio estimates of household food insecurity based on the univariate logistic regression model
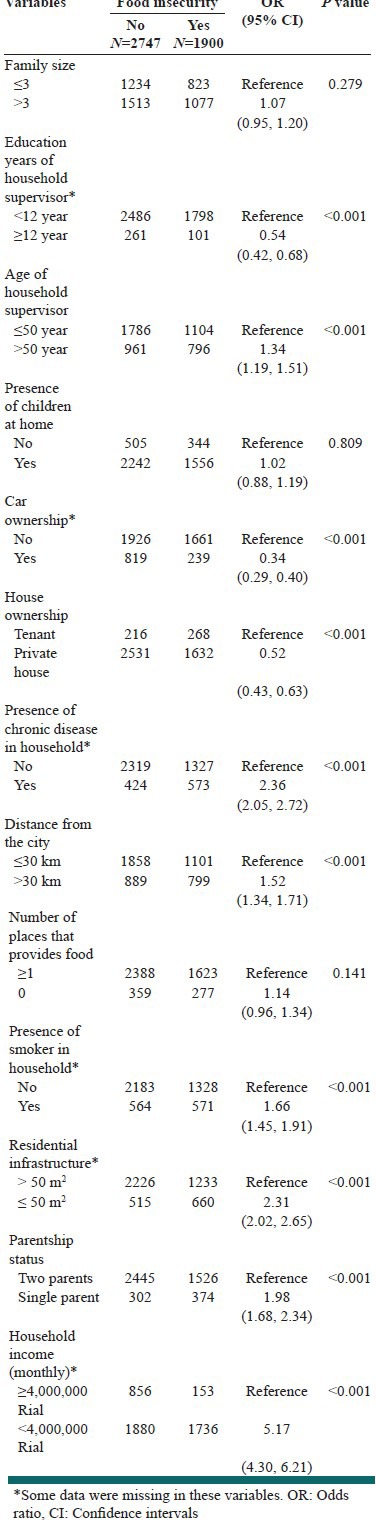
Table 3.
Odds ratio estimates of household food insecurity based on the multivariate logistic regression model
DISCUSSION
This investigation was a cross-sectional study designed to assess the prevalence of food insecurity and associated factors among rural households in Neyshabur. The findings indicated that household food insecurity was prevalent among rural households of Neyshabur (40.9%). In Dastgiri's study used Iranian version of the Six-Item Short questionnaire of Household Food Security Scale in order to assess prevalence food insecurity in the northwest region of Iran observed that 59.3% of households experienced food insecurity.[14] In Ramesh’ study, the results showed that the prevalence of food insecurity without hunger was 27.8% and food insecurity with hunger was 16.2%.[15] The study conducted by Furness, in Los Angeles, showed that 24.4% of households experienced food insecurity.[11] In Piaseu's study conducted on 199 households in Thailand, it was observed that 39.2% of households experienced food insecurity without hunger and 30.1% of households had food insecurity with hunger.[16]
In this study, after the use of multivariate logistic regression model [Table 3] observed that car ownership, house ownership, presence of chronic disease in household, distance from the city, presence of smoker in household, residential infrastructure, parentship status, and household income (per month) are influential factors that affect household food insecurity of study population. In Sharafkhani's study was conducted on 2500 households selected from Qaresoo region in the north-west of Iran and used of the Six-Item Short questionnaire of Household Food Security Scale, the influential factors affecting household food insecurity were: Distance from the city, number of centers that provides food, family size, presence of both parents, and residential infrastructure.[10] In Dastgiri's study used of the Six-Item Short questionnaire of Household Food Security Scale, the influential factors affecting household food insecurity were: Children at home, elderly people at home, education (head of family), car ownership, house ownership, monthly income, and parentship status.[14] In Furness's study conducted among households in Los Angeles County and used of the Six-Item Short questionnaire of Household Food Security Scale, the influential factors were: Income, children in household, past homelessness.[11] In study conducted by Mohammadzadeh, food insecurity was positively associated with number of members in the household and negatively associated with parental education level, job status and household economic status.[17] As observed in this study and other mentioned studies, socio-economic status had a remarkable role on the high prevalence of food insecurity in the surveyed regions. Data such as these can be used to specify high-risk areas with food insecurity and use of it to implement interventional programs in there. Some studies were carried out in order to assess quality of diet in Iranian people and they evaluated some indices such as dietary energy density, dietary diversity score, and so on.[18,19,20] Food insecurity is likely related to quality of diet. So with attention to result of this study and other similar studies and furthermore, the importance of diet quality, we suggest that future studies assess the relation between food insecurity and the diet quality indices beside prevalence of food insecurity assessment in different rural regions of Iran.
Strengths and limitations
The most notable strengths of this study include: Use of large sample size, use of logistic regression model, and response rate greater than 92%. Furthermore, this study has some limitations: First, causality between the compared variables could not be concluded due to the cross-sectional design of the study. Second, 353 households were excluded from the study because of refusal to participate in the study.
CONCLUSIONS
The findings from this study showed that food insecurity is prevalent among rural households of Neyshabur and also observed that some variables had a relation to food insecurity especially household income per month. This indicates that there is an urgent need to identify and implement interventional programs by Neyshabur leaderships to improve the undesirably high level of food insecurity in rural households.
ACKNOWLEDGMENTS
The authors gratefully acknowledge households that participated in this study.
Footnotes
Source of Support: This research was funded by Neyshabur University of Medical Sciences
Conflict of Interest: None declared
REFERENCES
- 1.Washington: USDA; 2011. [Last accessed 2011 Sep 16]. United States Department of Agriculture. Economic Research Service [Internet]. Food Security in the United States: Definitions of Hunger and Food Security. Available from: http://www.ers.usda.gov/Briefing/Food Security/labels.htm . [Google Scholar]
- 2.Rome: Food and Agriculture Organization of the United Nations; 2012. [Last accessed 2012]. The State of Food Insecurity in the World 2012: Economic growth is necessary but not sufficient to accelerate reduction of hunger and malnutrition. Available from: http://www.fao.org/docrep/016/i3027e/i3027e.pdf . [Google Scholar]
- 3.New York: United States Agency for International Development, Bureau for Democracy, Conflict, and Humanitarian Assistance, Office of US Foreign Disaster Assistance; 2009. [Last accessed 2011 Sep 16]. Global Food Insecurity and Price Increase (Situation Report # 1, Fiscal Year 2009) Available from: http://www.usaid.gov/our_work/humanitarian_assistance/foodcrisis/documents/052209_ foodcrisis_sr1.pdf . [Google Scholar]
- 4.Tarasuk V. A critical examination of community-based responses to household food insecurity in Canada. Health Educ Behav. 2001;28:487–99. doi: 10.1177/109019810102800408. [DOI] [PubMed] [Google Scholar]
- 5.Nord M, Coleman-Jensen A, Andrews M, Carlson S. ERR- 108, U.S. Dept. of Agriculture, Econ. Res. Serv; 2010. Nov, Household Food Security in the United States, 2009; p. 4. [Google Scholar]
- 6.Sharafkhani R, Dastgiri S, Gharaaghaji R, Ghavamzadeh S, Didarloo A. The role of household structure on the prevalence of food insecurity. Eur J Gen Med. 2010;7:385–8. [Google Scholar]
- 7.Dastgiri S, Soltanali M, Totonchi H, Ostadrahimi AR. Determinants of food insecurity: A cross-sectional study in Tabriz. J Ardabil Univ Med Sci. 2006;6:233–9. [Google Scholar]
- 8.Hakim S, Dorosty AR, Eshraghian MR. Association of food insecurity and household socio-economic status with the body mass index among urban women in Dezful. J Sch Public Health Inst Public Health Res. 2010;8:55–66. [Google Scholar]
- 9.Karam Soltani Z, Dorosty Motlagh A, Eshraghian MR, Siassi F, Djazayeri A. Obesity and food security in Yazd primary school students. Tehran Univ Med J. 2007;65:68–76. [Google Scholar]
- 10.Sharafkhani R, Dastgiri S, Gharaaghaji Asl R, Ghavamzadeh S. Factors influencing household food security status. Food Nutr Sci. 2011;2:31–4. [Google Scholar]
- 11.Furness BW, Simon PA, Wold CM, Asarian-Anderson J. Prevalence and predictors of food insecurity among low-income households in Los Angeles County. Public Health Nutr. 2004;7:791–4. doi: 10.1079/phn2004608. [DOI] [PubMed] [Google Scholar]
- 12.Dastgiri S, Tutunchi H, Ostadrahimi A, Mahboob S. Sensitivity and specificity of a short questionnaire for food insecurity surveillance in Iran. Food Nutr Bull. 2007;28:55–8. doi: 10.1177/156482650702800106. [DOI] [PubMed] [Google Scholar]
- 13.Blumberg SJ, Bialostosky K, Hamilton WL, Briefel RR. The effectiveness of a short form of the Household Food Security Scale. Am J Public Health. 1999;89:1231–4. doi: 10.2105/ajph.89.8.1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Dastgiri S, Sharafkhani R, Gharaaghaji R, Ghavamzadeh S. Prevalence, influencing factors and control of food insecurity: A model in the northwest of Iran. Asia Pac J Clin Nutr. 2011;20:613–7. [PubMed] [Google Scholar]
- 15.Ramesh T, Motlagh AD, Abdollahi M. Prevalence of food insecurity on urban household in Shiraz city and its related socioeconomic factors. Iranian J Nutr Food Tech. 1388;4:53–64. [Google Scholar]
- 16.Piaseu N, Mitchell P. Household food insecurity among urban poor in Thailand. J Nurs Scholarsh. 2004;36:115–21. doi: 10.1111/j.1547-5069.2004.04023.x. [DOI] [PubMed] [Google Scholar]
- 17.Mohammadzadeh A, Dorosty A, Eshraghian M. Household food security status and associated factors among high-school students in Esfahan, Iran. Public Health Nutr. 2010;13:1609–13. doi: 10.1017/S1368980010000467. [DOI] [PubMed] [Google Scholar]
- 18.Azadbakhat L, Haghighatdoost F, Esmailzadeh A. Dietary energy density is inversely associated with the diet quality indices among Iranian young adults. J Nutr Sci Vitaminol (Tokyo) 2012;58:29–35. doi: 10.3177/jnsv.58.29. [DOI] [PubMed] [Google Scholar]
- 19.Azadbakht L, Mirmiran P, Hosseini F, Azizi F. Diet quality status of most Tehranian adults needs improvement. Asia Pac J Clin Nutr. 2005;14:163–8. [PubMed] [Google Scholar]
- 20.Rouhani MH, Mirseifinezhad M, Omrani N, Esmaillzadeh A, Azadbakht L. Fast food consumption, quality of diet, and obesity among Isfahanian adolescent girls. J Obes 2012. 2012:8. doi: 10.1155/2012/597924. [DOI] [PMC free article] [PubMed] [Google Scholar]