

Abstract
Since a very long time, a significant number of patients have been seeking treatment at Complementary and Alternative Medicine health facilities, but the disease burden at these facilities has never been assessed and documented. Present cross-sectional study was carried out at Ayurvedic tertiary care hospital to document and to assess the rationale of disease reporting at Ayurvedic institutions of the northern state of India from January 2011 to October 2011. Almost half of the patients’ morbidities were not classified at all into any of the disease categories. The common reported morbidities at study hospital were: Respiratory (10.5%), neuromuscular (9.5%), digestive (9.2%) and circulatory (9.1%) disorders. As the majority of diseases were unclassified, so mainstreaming of the effective disease surveillance would be required to understand the morbidity pattern and successful treatment practices at health facilities.
Keywords: Ayurveda, morbidity, surveillance
INTRODUCTION
The chronic diseases like cardiovascular diseases, diabetes and cancer contributes to almost half of the all-cause mortality in India.[1] Weighted prevalence of ischemic heart diseases was observed as 25.3/1000 population, and 118.0/1000 population for diabetes mellitus in an urban area of India.[2] It was observed due to common risk factors like physical inactivity, unhealthy diet, tobacco use and stress. Along with growth and development, they were observed to be increasing in developing and developed countries.[3] Reduction in common risk factors was considered to be one of the essential preventive and control strategies for chronic diseases.[4] Like modern medicine, the Complementary and Alternative Medicine (CAM) - Ayurveda (knowledge or science of life) - primarily concerned with the body. It had been mentioned in Ayurveda, about the three pillars for healthy and long life; proper diet (ahar), proper activities (vihar), and divine life-style and control of sexuality (brahmacharya).[5,6] Break in any of these principles had been considered as cause of disease. Improper and unbalanced diet like undigested, junk, and accumulated food was also considered toxic for the body.[5] Ayurveda had been oldest and most organized scientific discipline, which was providing health-care. Once upon a time, their classical text like Charak Samhita (100 AD) is an excellent source of information about the holistic health, herbs, diseases, and surgical treatment for the entire country and the world.[7] Like yoga, Ayurveda derived its origin to the hoary Vedas and considering one of the sub-Vedas (upa-Veda).[5] Therefore, its traditional holistic approach and principles observed to be have a potential in order to reduce the risk factors of chronic diseases in the community. It was already evident that CAM had been widely used in Africa (80.0%), Australia (49.0%), Indonesia (40.0%), France (75.0%), and even in United States (29.0-42.0%).[8] In India as well, people are using the CAM services through 2860 large hospitals across the country.[1] CAM has been integrated into primary health-care of the country under the National Rural Health Mission.[9] Pattern of reported diseases at the CAM facilities has not been shared with the modern medicine in India despite the provision of care to a significant group of the population.[1] Therefore, the present study was undertaken to describe the clinical profile of patients with chronic diseases at a tertiary care Ayurvedic hospital in North India.
METHODOLOGY
The study was a part of assignment for the fellows appeared for 3 months course on “Non-Communicable Disease and Health Promotion” at Department of Community Medicine, Dr. Rajendra Prasad Government Medical College, Kangra, Himachal Pradesh. Total 4 fellows appeared for the course and a 1 month field based assignment was allotted. During the course period fellows were assigned a mentor and a topic for study. Present study was hospital based record based descriptive study carried out at Department of Kayachikitsa, Rajiv Gandhi Post Graduate Ayurvedic College, Kangra, Himachal Pradesh. As per census 2011, the provisional population of the Himachal Pradesh was 68 56 509 (49.3% females) and 15 07 223 (50.3% females) of Kangra district of the state.[10] Complied monthly data were accessed from the outpatient department (OPD) records section from January 2011 to October 2011. A single person collected the number of patients with an available diagnosis for every month. The data were collected from structured data collection tool. In addition, 30 case records (patient file) of admitted patients of hypertension and Diabetes Mellitus were selected randomly - using a random number table - from the inpatient department (IPD). A total 30 case records were decided to study treatment practice at a tertiary care center. Small number was kept due to the logistics constraints. Data were entered and analyzed by Epiinfo 3.2 statistical software. Before the data collection, ethical clearance form institution ethics committee and consent from studied health institutions was obtained.
RESULTS
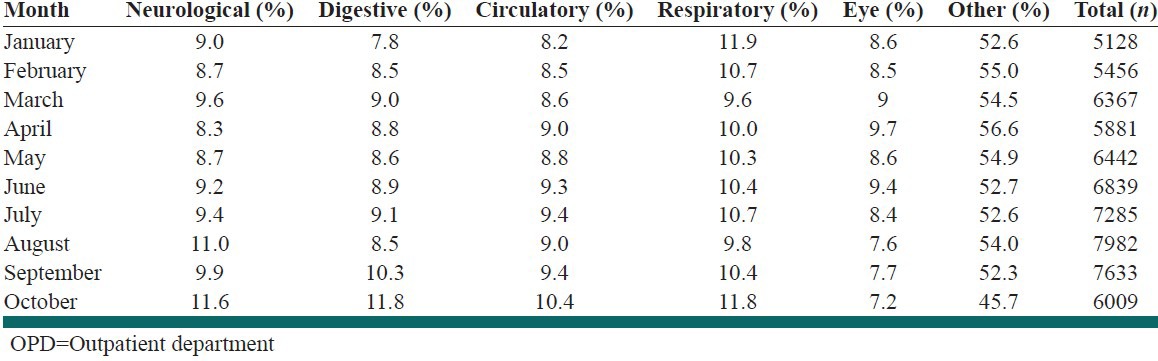
Total 65 022 patients attended the Ayurvedic OPD over 10 months. Significantly (P = 0.00) more males (51.1%) reported at OPD more than males. Total 10,276 (15.8%) children up to 5 years of age also sought treatment. Almost half (53.1%) of the patients were remained unclassified and kept under “other category.” Commonly reported morbidities were related to respiratory (10.5%), neuromuscular (9.5%), digestive (9.2%), circulatory (9.1%), and eye (8.4%) system. The trend remained the same in all the reported months [Table 1].
Table 1.
Monthly trend of reported patients in the OPD of Kayachikitsa at Rajiv Gandhi Post Graduate Ayurvedic College, Kangra, Himachal Pradesh, 2011
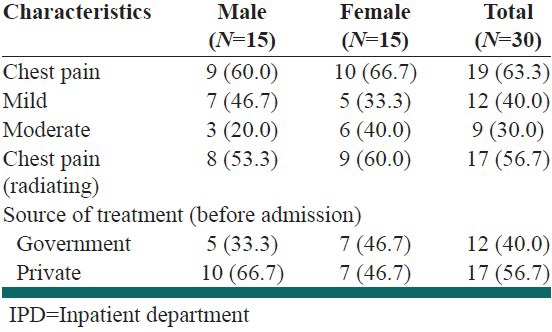
IPD records of 30 hypertensive patients at Ayurvedic tertiary hospital showed that the chest pain was the chief complaint (63.3%) with mild to moderate intensity (70.0%) and of radiating (56.7%) in nature. It was observed that more than half (56.7%) of the patients sought treatment from private practitioners before the admission [Table 2]. Admitted patients had a history of hypertension for average 9 months and were on regular treatment for 21.3% of disease duration. Diabetes Mellitus had long standing history of average 145 month among the admitted patients, and since diagnosis (90.3%) were on regular treatment. Majority of patients with hypertension were being managed with Aswaganda (66.0%) and Tagar powder (56.6%).
Table 2.
Symptomatic and management profile of patients in IPD of Kayachikitsa at Rajiv Gandhi Post Graduate Ayurvedic College, Kangra, Himachal Pradesh, 2011
DISCUSSION
Elevated blood pressure along with overweight and high cholesterol is a known risk factor for many chronic diseases. The chronic diseases are contributing about 46.0% of the all-cause mortality in India.[11] Evidence from India reported prevalence of chronic diseases up to 30.0% in the general population.[12] It had been found to be prevalent in urban (36.4%) along with slum (25.4%) and rural (24.0%) area.[13] Therefore, it cannot be considered a health condition of only urban area. The present study at rural tertiary care health institute of Ayurveda, showed that most of the patients were suffering from disorders related to respiratory, neuromuscular, and circulatory system, mostly suggestive of chronic diseases. Based upon the grouped OPD data it was observed to be difficult to further ascertain the causes of morbidity such as heart attack, brain attack, diabetes mellitus etc., Majority of patients were even not classified at all despite the complete diagnosis at the OPD. It hindered the information that could ascertain that whether these patients were affected with the exact cause of chronic or acute disease.
In the studied state, a total 27 Ayurvedic hospitals with 580 beds, 1105 dispensaries and 7326 registered practitioners exist at the time of study. In the country, a total of 254 graduate and 64 Post Graduate Ayurvedic colleges were producing 1197 under and 1110 Post Graduates every year. In addition, a total of 2458 hospitals with 44820 beds, 15353 dispensaries, 478750 registered practitioners.[14]
In Ayurveda, dietary factors like unhealthy diet considered as a known risk factor for chronic diseases like consumption of high glycemic index, junk and salted food.[4] However, food was being considered as medicine in Ayurveda like Barley/turmeric for obesity, Kulatha for Rheumatoid arthritis, Ashwagandha as a general tonic. Ayurveda had been playing a vial-role in the provision of treatment for common morbidities in India. Herbal Ayurvedic products considered being safe and effective in maintaining the healthy dietary practices. Ayurvedic products like jams, jellys, juices, biscuits, ice-cream, candies, chocolates, granules, flour, tea etc., were recommended as healthy food and to be promoted to the crowd out the junk food in the existing market.[6]
Therefore, with a vast human resource and the available Ayurvedic treatment potential in the country, the rising trend of chronic diseases due to non-healthy life-style and dietary behavior could be managed successfully. Furthermore, the actual burden and types of chronic disease in CAM discipline need to be studied and shared. In this respect, standard method of case reporting modified as per the discipline to Integrated Disease Surveillance Project (IDSP) at all levels and types of CAM health facilities would certainly help to capture exact disease burden. As, Government of India had already declared the mainstreaming of CAM in modern health-care delivery system as it had recommended by appointment of at least one CAM specialist at the community health center.[9] Ayurveda was being the oldest and the largest CAM discipline in India, so, the integration of information from the Ayurvedic health institution through IDSP would be required to help for formulation of healthy public policy.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Debas HT, Laxminaryan R, Straus S. Complementary and alternative medicine. In: Jamison DT, Breman JG, Measham AR, Alleyne G, Claeson M, Evans DB, et al., editors. Disease control priorities in developing countries. New York USA: Oxford University Press; 2006. pp. 1281–4. [PubMed] [Google Scholar]
- 2.Shah B, Kumar N, Menon GR, Khurana S, Kumar H. New Delhi: Indian Council of Medical Research; 2006. Assessment of Burden of Non Communicable Diseases. [Google Scholar]
- 3.Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet. 2007;370:1929–38. doi: 10.1016/S0140-6736(07)61696-1. [DOI] [PubMed] [Google Scholar]
- 4.Gaziano TA, Galea G, Reddy KS. Scaling up interventions for chronic disease prevention: The evidence. Lancet. 2007;370:1939–46. doi: 10.1016/S0140-6736(07)61697-3. [DOI] [PubMed] [Google Scholar]
- 5.Madanmohan . Presented at International Congress on Cardiology on internet; [Last accessed on 2012 May 12]. Role of Yoga and Ayurveda in Cardiovascular Diseases. Available from: http://www.fac.org.ar/qcvc/llave/c039i/madanmohan.php . [Google Scholar]
- 6.Kohli KR. Bridging ayurved and modern medicine with special reference to neutraceuiticals. [Last accessed on 2012 May 15]. Available from: http://www.nutraceuticalsummit.in/nutra./Prof_K_R_Kohli.pdf .
- 7.Jadavji T, editor. 2nd ed. Varanasi: Chaukhamba Sanskrit Sansthan; 1990. Charaka Samhita, Chikitsa Sthana, Grahani Chikitsa Adhyaya, 15/20; p. 225. [Google Scholar]
- 8.Geneva: World Health Organization, Department of Health Statistics and Informatics; 2002. [Last accessed on 2012 May 15]. World Health Statistics, 2002. Available from: http://www.who.int/medicines/organization/trm/factsheet271.doc . [Google Scholar]
- 9.National Rural Health Mission: Mission document. New Delhi: Ministry of Health and Family Welfare; [Last accessed on 2012 May 10]. Available from: http://www.mohfw.nic.in/NRHM/Documents/Mission_Document.pdf . [Google Scholar]
- 10.New Delhi: Ministry of Home Affairs; [Last accessed on 2012 Apr 5]. Registrar General of India and Census Commissioner, Government of India. Available from: http://censusindia.gov.in/2011.prov.results/data_files/himachal/Figure%20at%20 glance.%20Himachal%20Prad.pdf . [Google Scholar]
- 11.Jha P, Gajalakshmi V, Gupta PC, Kumar R, Mony P, Dhingra N, et al. Prospective study of one million deaths in India: Rationale, design, and validation results. PLoS Med. 2006;3:e18. doi: 10.1371/journal.pmed.0030018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Gupta R. Trends in hypertension epidemiology in India. J Hum Hypertens. 2004;18:73–8. doi: 10.1038/sj.jhh.1001633. [DOI] [PubMed] [Google Scholar]
- 13.Kar SS, Thakur JS, Virdi NK, Jain S, Kumar R. Risk factors for cardiovascular diseases: Is the social gradient reversing in northern India? Natl Med J India. 2010;23:206–9. [PubMed] [Google Scholar]
- 14.New Delhi: Department of AYUSH. Ministry of Health and Family Welfare; [Last accessed on 2012 May 15]. National Rural Health Mission: Mission Document. Available from: http://indianmedicine.nic.in/writereaddata/linkimages/7976103845-infrastructureSystemwise%20Statistics%20AYURVEDA.pdf . [Google Scholar]