

Abstract
Aim:
A randomized controlled clinical study was undertaken to evaluate the effectiveness of scaling and root planing (SRP) by using Magnifying Loupes (ML) and dental operating microscope (DOM).
Materials and Methods:
A total of 90 human teeth scheduled for extraction from 18 patients aged between 25 and 65 years suffering from generalized chronic severe periodontitis were randomly assigned to three treatment groups. Group 1 consisted SRP performed without using magnification (unaided), Group 2-SRP with ML and Group 3-SRP with DOM. Following extractions, samples were prepared for (i) evaluation of surface topography by atomic force microscopy, (ii) presence of smear layer, debris by scanning electron microscopy (iii) elemental analysis by energy dispersive X-ray analysis. Data was subjected to statistical analysis using analysis of variance, post-hoc (Tukey-HSD) and Chi-square test.
Results:
Statistically significant (P < 0.001) difference was found among the different treatment groups. Group 3 was the best while Group 1 was the least effective technique for SRP. Order of efficacy in terms of the surface was found to be - Palatal < Lingual < Distal ≃ Mesial < Buccal. Efficiency in mandibular to maxillary teeth was found to be significant (P < 0.05), also anterior to posterior teeth (P < 0.05).
Conclusion:
Magnification tools significantly enhance the efficacy of supragingival and subgingival SRP.
Keywords: Atomic force microscopy, dental operating microscope, energy dispersive X-ray spectroscopy, magnification, scaling and root planing, scanning electron microscopy
Introduction
The goals of periodontal therapy are to alter or eliminate the microbial ecology and contributing risk factors for periodontitis, thereby arresting the progression of disease and preserving the dentition in health, comfort and function with appropriate aesthetics and to prevent the recurrence of periodontitis.[1]
Scaling and root planing (SRP) is one of the most commonly utilized conservative procedures for the treatment of periodontal diseases and has been used as the “gold standard” therapy in comparison to other therapeutical procedures.[2] The traditional modality as an initial periodontal treatment phase is to perform SRP by jaw quadrant at a series of appointments.[3] Corbet EF[4] in 1977 set forth the rationale for root planing such as root smoothness, removal of diseased cementum and preparation for new attachment. It is necessary because deposits of calculus on root surfaces are frequently embedded in cemental irregularities, which contain bacterial endotoxins that penetrate into the cementum. Therefore, careful subgingival SRP is an effective means to eliminate gingivitis and reduce the probing depth even at sites with initially deep periodontal pockets.[5,6,7]
The world of periodontics has seen a rapid change in the last 30 years with ever improving treatment modalities. New diagnostic instruments and surgical techniques were embraced by the periodontists all over the world. Vast array of instruments and equipments such as micro ultrasonics, endoscope, Lasers and magnification tools are available to achieve a biologically acceptable root surface. However, there is still a lack of information regarding the efficacy of SRP by using magnification. Magnification is becoming an increasingly important requirement for high quality contemporary dentistry. Magnifying Loupes (ML), dental operating microscope (DOM) are the common magnification tools used in the dental practice, providing distinct advantages to the clinician such as illumination, magnification and increased precision in the delivery of operating skills.[8]
Limited data is available in the literature regarding the use of magnification for performing SRP. Hence, the present research was undertaken to evaluate the efficacy of supragingival and subgingival SRP with and without the use of ML and DOM, based on the results of microanalysis of root surface post SRP, by scanning electron microscopy (SEM), elemental analysis of root surface by energy dispersive X-ray analysis (EDAX) and micro morphology of root surface by atomic force microscopy (AFM).
Materials and Methods
Study was conducted in the Department of Periodontology. Ethical clearance was obtained from the Institutional Ethics Committee in accordance with the declaration of Helsinki. Patients were explained about the procedure to be performed and the consent was obtained. Detailed case history of all patients was recorded. Supragingival and Subgingival SRP were performed on the teeth to be extracted.
Study design
A randomized controlled clinical study consisting of 90 human teeth scheduled for extraction from 18 patients aged between 25 and 65 years suffering from generalized chronic severe periodontitis were randomly assigned to following three treatment groups with inclusion and exclusion criteria.
Group 1: SRP performed by magnetostrictive ultrasonic scaler (Cavitron, Dentsply) followed by hand instruments with sharp Gracey curettes and Subgingival scalers (Hu-Friedy) without using any magnification device, i.e., unaided
Group 2: SRP performed by magnetostrictive ultrasonic scaler (Cavitron, Dentsply) followed by hand instruments with sharp Gracey Curettes and Subgingival Scalers (Hu-Friedy) with the help of ML of magnification ×4.5 to ×5.5 (Microsurgery Instruments Co: Texas)
Group 3: SRP performed by magnetostrictive ultrasonic scaler (Cavitron, Dentsply) followed by hand instruments with sharp Gracey Curettes and Subgingival Scalers (Hu-Friedy) with DOM of magnification ×3.5, ×5.0, ×8.5, ×13.5, ×20.5 (3D Medical Systems, USA).
Inclusion criteria
Patients with good general health, aged between 25 and 65 years suffering from generalized chronic severe periodontitis
Teeth scheduled for the extraction having 8-10 mm attachment loss
Caries free teeth
Teeth without wasting diseases or cervical restorations.
Exclusion criteria
Patients allergic to local anesthesia
Endodontically involved teeth
Pregnant women.
Before extracting the teeth, area was marked with the help of a round bur, making a first linear groove at the location of the gingival margin to designate supragingival area, (distance between cementoenamel junction and the marked groove). Teeth were then extracted avoiding trauma to the root surface and were placed in 1% methylene blue for 2 min to stain the attached tissues and second linear groove was marked at the level of junctional epithelium demarcating the subgingival area (distance between the first and second groove). Teeth in three different groups were then placed in normal saline and transported for AFM and SEM along with EDAX analysis. Samples from all surfaces, supragingival and subgingival area were selected and a 1 mm × 2 mm × 1 mm thick slice of each surface and area to be analyzed was cut with the help of diamond disc. SEM and EDAX analysis was carried out. AFM was carried out at Department of Physics, Indian Institute of Technology, Delhi for topographic analysis. All the images and graphs were obtained by AFM explorer manufactured by Veeco-Thermo Microscopes (USA) with using contact mode with tips from silicon nitride (type 1520-00, Veeco). Maximum measurable changes of the surface profile had been measured for obtaining images with in 10 μm × 10 μm with in the center of each section put on the stage.
AFM surface roughness evaluation
To define surface topography of sample, the following parameters were evaluated.[9]

Sample preparation for SEM and EDAX evaluation
Sections of all samples were stored in normal saline to avoid dehydration and evaluated by SEM along with EDAX. Photographs of the central portion of each specimen were taken at ×3200 magnification by SEM (LEO 430 USA). SEM examination was performed by a single blinded examiner. Element analysis of root surface was performed by EDAX. The number and energy of the X-rays emitted from a specimen can be measured by an energy-dispersive spectrometer. As the energy of the X-rays is characteristic of the difference in energy between the two shells and of the atomic structure of the element from which they were emitted, this allows the elemental composition of the specimen to be measured. Comparison of mean values of minerals in different groups was also compared with normal root (without calculus – negative control) and subgingival calculus (positive control) values.
The parameters evaluated were: Surface morphology (regular, irregular or flaky surface), presence or absence of smear layer, debris, calculus, scratches and the opening of dentinal tubules.
Grading
The grades are given as follows:[10]
Grade I: Absence of visible debris and plaque, with good exposure of dentinal tubules and no evidence of remaining smear layer
Grade II: No visible debris; no exposure of dentinal tubules; and presence of smear layer
Grade III:Presence of visible debris and plaque all over the scanned area; no visible tubuli; and smear layer present on the entire surface.
All observations were tabulated by a single observer and were subjected to statistical analysis using Statistical Package for Social Sciences 15.0. The Chi-square, analysis of variance (ANOVA) and Tukey HSD tests were used to compare the within the group and between group variances among the study groups.
Results
Group 1 sample
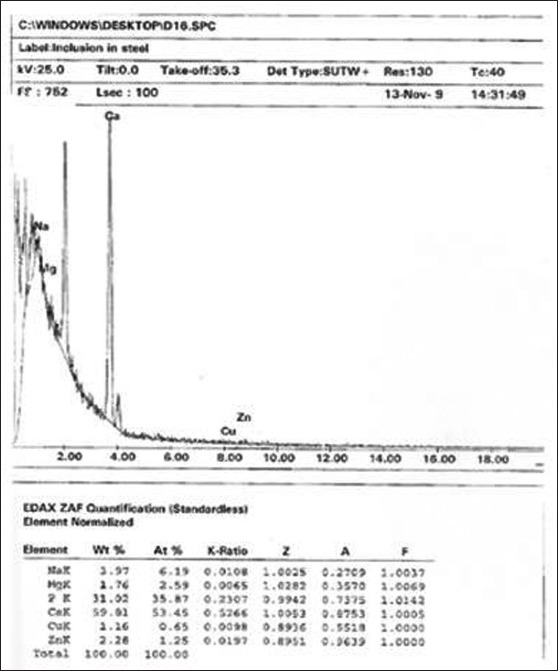
Topographic analysis by AFM of post SRP, unaided group sample revealed the presence of debris, calculus and scratches all over the surface [Figure 1]. SEM analysis of the same group showed the presence of visible debris all over the scanned area, smear layer present on the entire surface and no visible dentinal tubules at magnification ×3200 [Figure 2] and EDAX analysis revealed maximum levels of mineral contents for magnesium (Mg), potassium (K) and minimum P on the surface in weight% as shown in [Figure 3].
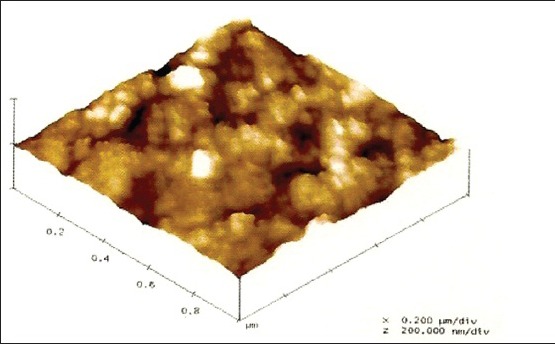
Figure 1.
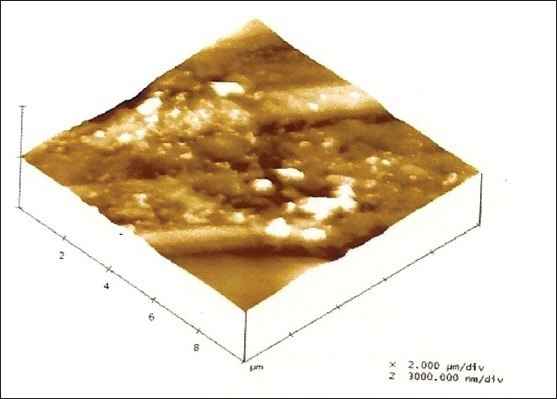
Topographic analysis by atomic force microscopy of post scaling and root planing of unaided group reveals the presence of debris, calculus and scratches all over the surface
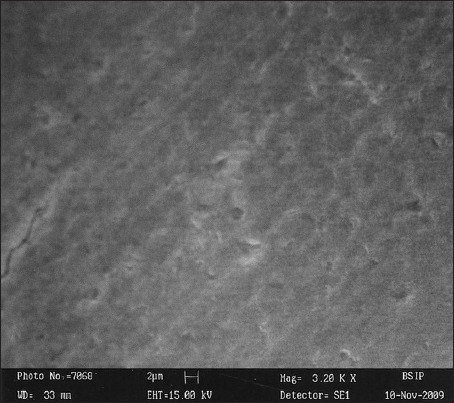
Figure 2.
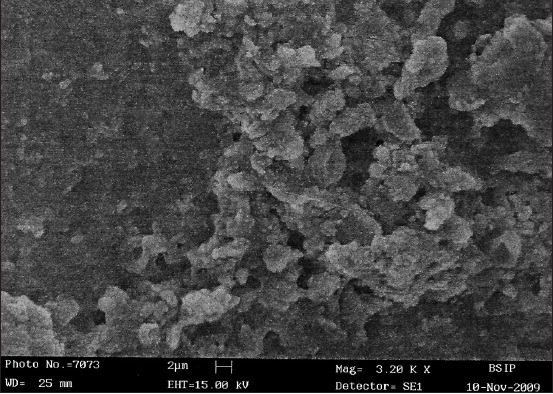
Scanning electron microscopy analysis of the post scaling and root planing of unaided group shows the presence of visible debris all over the scanned area, smear layer present on the entire surface and no visible dentinal tubules at magnification ×3200
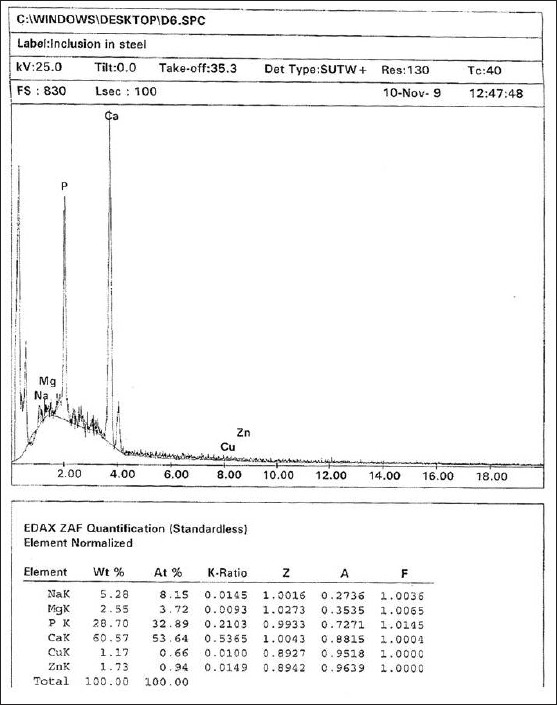
Figure 3.
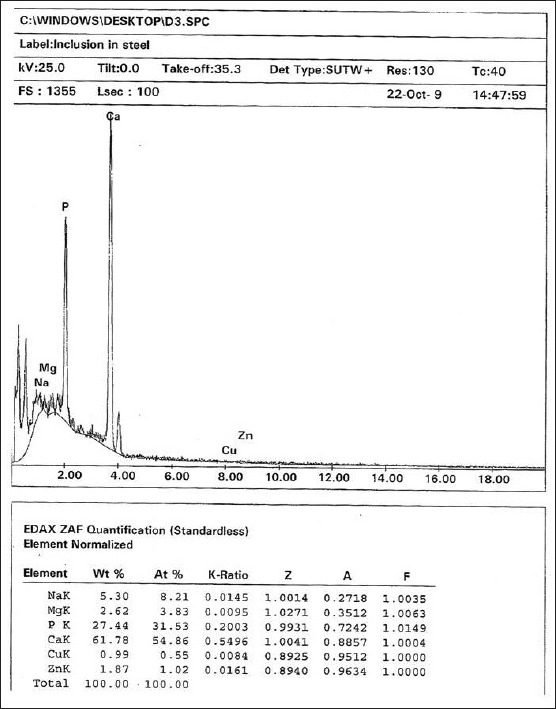
Energy dispersive X-ray analysis of the post scaling and root planing of unaided group reveals maximum levels of mineral contents for Mg, K and minimum P in weight%
Group 2 sample
Topographic analysis by AFM of post SRP, ML sample revealed the presence of smear layer with opening of dentinal tubules at some places [Figure 4]. SEM analysis of the same group showed no visible debris, with some opening of dentinal tubules and presence of smear layer on the surface at magnification ×3200 [Figure 5] and EDAX analysis revealed mineral contents on the surface of ML sample in weight% as shown in [Figure 6].
Figure 4.
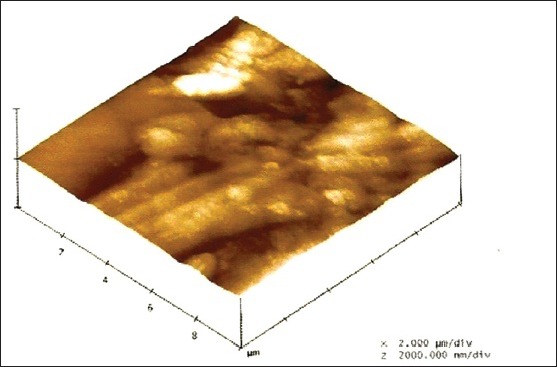
Topographic analysis by atomic force microscopy of post scaling and root planing, Magnifying Loupes sample reveals the presence of smear layer with opening of dentinal tubules at some places
Figure 5.
Scanning electron microscopy analysis of the post scaling and root planing of Magnifying Loupes group shows no visible debris, with some opening of dentinal tubules and presence of smear layer on the surface at magnification ×3200
Figure 6.
Post scaling and root planing, energy dispersive X-ray analysis reveals mineral contents on the surface of Magnifying Loupes sample in weight%
Group 3 sample
Topographic analysis by AFM of post SRP, DOM sample revealed clear surface with opening of dentinal tubules all over the surface [Figure 7]. SEM analysis of the same group showed absence of visible debris with good exposure of dentinal tubules and no evidence of remaining smear layer at magnification ×3200 [Figure 8] and EDAX analysis revealed complete elimination of diseased cementum as shown in [Figure 9].
Figure 7.
Topographic analysis by atomic force microscopy of post scaling and root planing, dental operating microscope sample revealed clear surface with opening of dentinal tubules all over the surface
Figure 8.
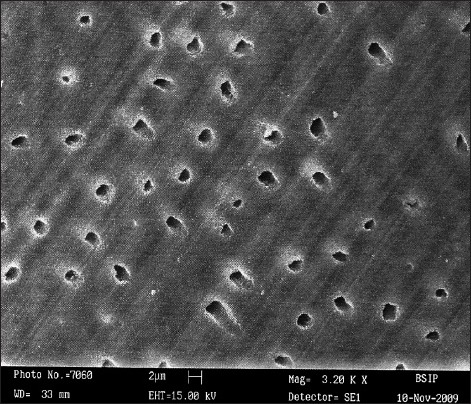
Post scaling and root planing, scanning electron microscopy analysis of dental operating microscope group showed absence of visible debris with good exposure of dentinal tubules and no evidence of remaining smear layer at magnification ×3200
Figure 9.
Post scaling and root planing, energy dispersive X-ray analysis of dental operating microscope group revealed mineral values indicating complete elimination of diseased cementum
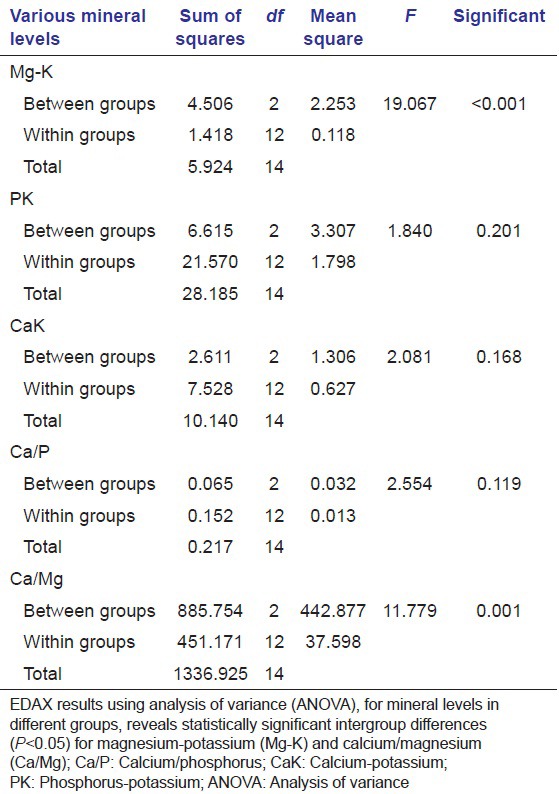
EDAX results using ANOVA for mineral levels in different groups is shown in Table 1, revealing statistically significant intergroup differences (P < 0.05) for magnesium-potassium (Mg-K) and calcium/magnesium (Ca/Mg).
Table 1.
ANOVA for mineral levels in different groups
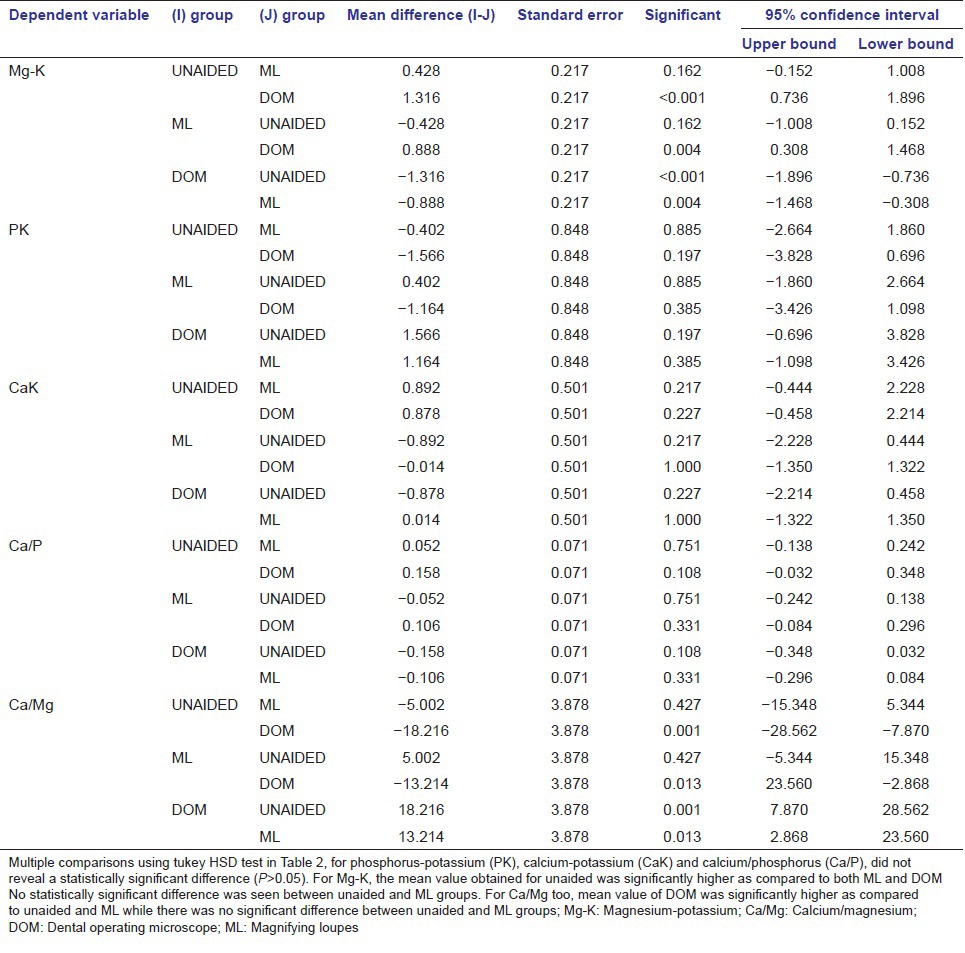
Multiple comparisons using Tukey HSD test in Table 2, for phosphorus-potassium (PK), calcium-potassium (CaK) and calcium/phosphorus (Ca/P), didn’t reveal a statistically significant difference (P > 0.05). For Mg-K, the mean value obtained for unaided was significantly higher as compared to both Loupe and DOM; no statistically significant difference was seen between unaided and Loupe groups. For Ca/Mg too, mean value of DOM group was significantly higher as compared with unaided and Loupe groups while there was no significant difference between unaided and ML groups.
Table 2.
Multiple comparisons using (Tukey HSD) test
One sample t-test was used to calculate significance of difference from controls shown in Table 3. For Mg-K, all the three groups had significantly higher mean value as compared with negative control (P < 0.05), the significance of difference was very highly significant for unaided and ML groups (P < 0.001) while for DOM group it was just significant (P = 0.020). As compared with positive control, all three groups had significantly lower mean values. The difference from positive control was highly significant for unaided group (P = 0.003) while for ML and DOM groups it was very highly significant (P < 0.001).
Table 3.
Comparison of mean values of minerals in different groups as compared to normal root without calculus (negative control) and subgingival calculus (positive control) values
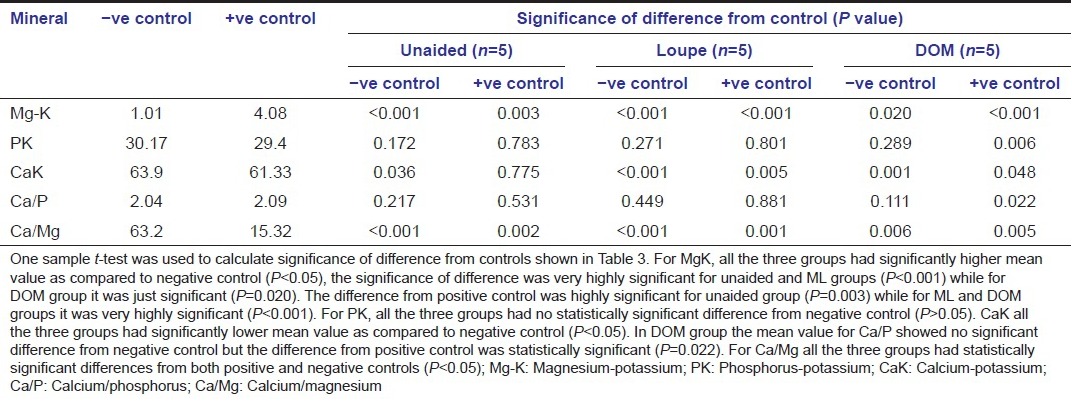
For PK, all three groups had no statistically significant difference from negative control (P > 0.05). However, as compared with positive control, DOM group had significantly higher mean value (P = 0.006) while the other two groups did not show a statistically significant difference.
For CaK, all the three groups had significantly lower mean value as compared with negative control (P < 0.05), however for positive control, unaided group did not show a significant difference (P = 0.775) while the mean value of ML and DOM groups were significantly lower (P < 0.05).
For Ca/P, the mean value of unaided group and ML group was not significantly different from either positive control or negative control. However, for DOM group the mean value showed no significant difference from negative control, but the difference from positive control was significant statistically (P = 0.022).
For Ca/Mg, all the three groups had statistically significant differences from both positive and negative controls (P < 0.05).
Grade distribution in three groups is depicted in Table 4. Entire 240 specimens in DOM group were graded as I, all 240 specimens in Loupe group were graded as II and all the specimens in unaided group were graded as III. There was a statistically significant difference among the groups (P < 0.001).
Table 4.
Grade comparison between the groups
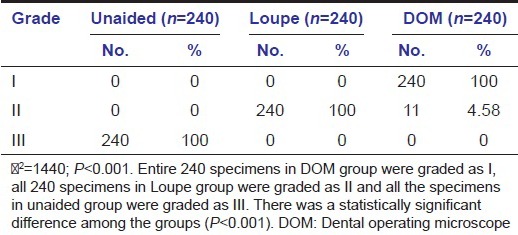
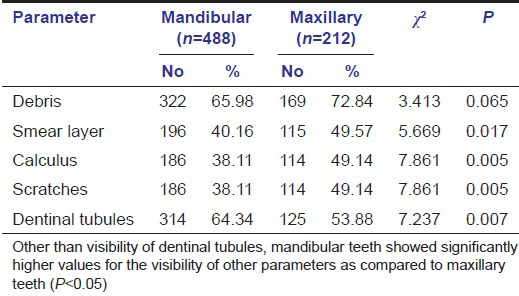
Table 5 analyzes the efficacy of SRP in mandibular to maxillary arch. Other than visibility of dentinal tubules, mandibular teeth showed significantly higher values for the visibility of other parameters as compared with the maxillary teeth (P < 0.05).
Table 5.
Efficacy of scaling and root planing in mandibular and maxillary teeth
Order of efficacy in terms of the surface was found to be-Palatal < Lingual < Distal ~_ Mesial < Buccal as shown in Table 6. Visibility of all the parameters other than dentinal tubules and debris, mesial and palatal surface showed higher values as compared to other aspects (P < 0.05). No significant difference in visibility of debris was seen among different surfaces (P = 0.675).
Table 6.
SEM analysis for efficacy of scaling and root planing in different aspects of teeth at ×3200
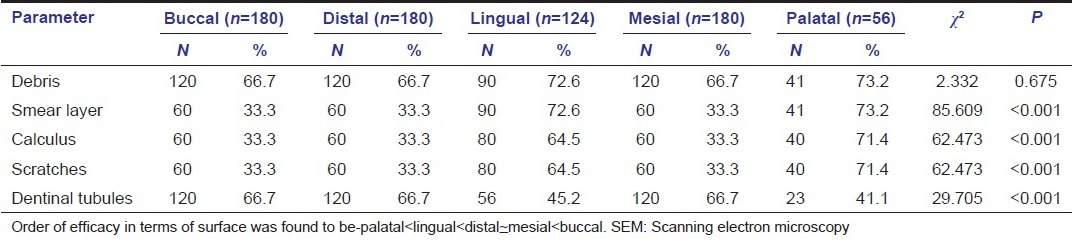
The proportion of Grade I and Grade II results was higher in lingual aspect as compared to all the other aspects while the proportion of Grade III results was higher in palatal aspect as compared to other aspects.
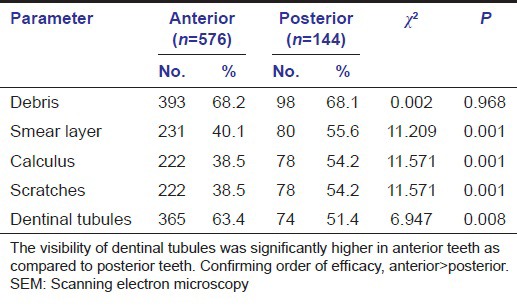
Results of SEM analysis for the efficacy of SRP, in anterior to posterior teeth at ×3200 are depicted in Table 7. Other than dentinal tubules and debris, for all the other parameters the visibility in anterior teeth was significantly lower as compared to posterior teeth (P < 0.05). No significant difference in visibility of debris was seen between two groups (P = 0.968). The visibility of dentinal tubules was significantly higher in anterior teeth as compared to posterior teeth. On the basis of above findings, the order of efficacy was anterior > posterior.
Table 7.
SEM analysis for efficacy of scaling and root planing in anterior/posterior teeth at ×3200
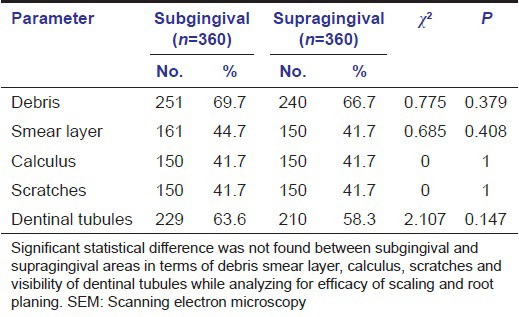
Significant statistical difference was not found between subgingival and supragingival areas in terms of debris smear layer, calculus, scratches and visibility of dentinal tubules while analyzing for efficacy of SRP in the area as shown in Table 8. On the basis of above findings, both areas were found to be equally effective when root planing was done in higher magnifications.
Table 8.
SEM analysis for efficacy of scaling and root planing in subgingival and supragingival area at ×3200
DOM group was proved to be the best while unaided group was the least effective technique as far as the cleaning efficiency was concerned. Mandibular teeth were more efficiently managed as compared to maxillary teeth while anterior teeth were more efficiently managed as compared to posterior teeth. Buccal surfaces were most effectively cleaned followed by mesial, distal, lingual and least effective was palatal. Supragingival and subgingival SRP were equally effective when performed under magnification.
Discussion
Removal of supra and sub gingival plaque and calculus along with the reduction of inflammation is the most important factor and always a primary goal of periodontal therapy. Traditional techniques involve blind, closed subgingival SRP or a flap for access surgery. Numerous studies indicated the difficulty in removing these accretions to the point that histologic manifestations of chronic inflammation are eliminated.[2,3,4,5] Deeper the pocket, the harder it is to instrument the area.
Closed SRP give good short term clinical results with shrinkage of pockets and a decrease in gingival inflammation but symptoms often slowly return. This is attributed to incomplete removal of subgingival plaque and calculus. Ultrasonic instrumentation has more advantages over hand instrumentation. SRP along with surgical approach may often yield better results, but it generally has greater post treatment morbidity and greater recession than nonsurgical approach. Closed root planing using an endoscope could produce the positive results clinically and histologically.[10,11,12,13,14,15]
The present study reveals the effectiveness of SRP under different magnifications using ML and DOM. Microanalysis of root surface was performed by using SEM, EDAX and AFM to study the root surface characteristics, elements and topography respectively, also discloses that SRP under magnification is more effective. Various studies have demonstrated the application of AFM for the investigations of ultra-morphology of superficial and deep dentin.[9,11,14] Selvig used a transmission electron microscope to observe alterations within cementum.[16]
EDAX results of the present study for levels of Mg and K showed that Group 1 had maximum levels followed by Group 2 and Group 3. However, for P and K, the order was just reverse with Group 1 showing minimal and Group 3 showing maximum values. For Ca and K, there was not much difference yet Group 1 had maximum value and Group 2 had minimum value. For Ca/P ratio, Groups 1 and 2 had very close values while Group 3 had minimum value. For Ca/Mg ratio, the differences were most evident, showing minimum value in Group 1 and maximum value for Group 3.
The most common elements detected on the root surface by EDAX, were P, Ca, Cu, Zn and Mg, while the few other elements detected, were sodium (Na), chlorine (Cl), K, aluminum (Al) and sulfur (S). It seems reasonable that there could be different elemental make-ups of hard tissue, even to the density and concentration of such constants as Ca and P. Concentrations did not vary to a great extent within the same root. Perhaps deep within the periodontal pocket, it is the organic phase of cementum that is affected by periodontal disease, but not the mineral phase as shown in various other studies.[17,18,19,20,21,22] Presence of minerals such as Cu, Zn and Mg are normal inorganic structures found in cementum of diseased and non-diseased root. This observation is in consistent with findings obtained by Barton and Van Swol,[23] which stated that any differences in the elements concentration noted within the root structure could be due to the concentration of these ions in body fluids during tooth formation. It is also possible that the dietary intake and ion exchange after tooth eruption could be reflected within the roots.
It was observed from the present study that magnification tools significantly enhance the efficacy of supra gingival and sub gingival SRP. Magnifying loupe with limited magnification showed better results than the unaided group. DOM proved to be the best aid in producing smooth root surface free of debris, calculus, scratches etc., and eliminating diseased cementum effectively.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Cobb CM, Drisko CH. Parameter on chronic periodontitis with slight to moderate loss of periodontal support. American Academy of Periodontology. J Periodontol. 2000;71(Suppl 5):853–5. doi: 10.1902/jop.2000.71.5-S.853. [DOI] [PubMed] [Google Scholar]
- 2.Ivie M, Kardum, Jurak I, Troselj KG, Pavelie K, Aurer, et al. The effect of scaling and root planing on the clinical and microbiological. Parameters of periodontal diseases. Acta Stomatol Croat. 2001;35:39–42. [Google Scholar]
- 3.Badersten A, Nilveus R, Egelberg J. Effect of nonsurgical periodontal therapy. II. Severely advanced periodontitis. J Clin Periodontol. 1984;11:63–76. doi: 10.1111/j.1600-051x.1984.tb01309.x. [DOI] [PubMed] [Google Scholar]
- 4.Corbet EF, Vaughan AJ, Kieser JB. The periodontally-involved root surface. J Clin Periodontol. 1993;20:402–10. doi: 10.1111/j.1600-051x.1993.tb00380.x. [DOI] [PubMed] [Google Scholar]
- 5.Daly CG, Seymour GJ, Kieser JB, Corbet EF. Histological assessment of periodontally involved cementum. J Clin Periodontol. 1982;9:266–74. doi: 10.1111/j.1600-051x.1982.tb02066.x. [DOI] [PubMed] [Google Scholar]
- 6.Newman HN, Hardy JH. Middle zone of the root surface integument of human teeth affected by chronic periodontitis. J Clin Periodontol. 1984;11:16–20. doi: 10.1111/j.1600-051x.1984.tb01304.x. [DOI] [PubMed] [Google Scholar]
- 7.Baker PJ, Roopenian DC. Genetic susceptibility to chronic periodontal disease. Microbes Infect. 2002;4:1157–67. doi: 10.1016/s1286-4579(02)01642-8. [DOI] [PubMed] [Google Scholar]
- 8.Belcher JM. A perspective on periodontal microsurgery. Int J Periodontics Restorative Dent. 2001;21:191–6. [PubMed] [Google Scholar]
- 9.Batista LH, Júnior JG, Silva MF, Tonholo J. Atomic force microscopy of removal of dentin smear layers. Microsc Microanal. 2007;13:245–50. doi: 10.1017/S1431927607070419. [DOI] [PubMed] [Google Scholar]
- 10.Dibart S, Capri D, Casavecchia P, Nunn M, Skobe Z. Comparison of the effectiveness of scaling and root planing in vivo using hand vs. rotary instruments. Int J Periodontics Restorative Dent. 2004;24:370–7. [PubMed] [Google Scholar]
- 11.Leknes KN, Lie T, Böe OE, Selvig KA. A correlation study of inflammatory cell mobilization in response to subgingival microbial colonization. J Periodontol. 1997;68:67–72. doi: 10.1902/jop.1997.68.1.67. [DOI] [PubMed] [Google Scholar]
- 12.Leknes KN, Lie T, Wikesjö UM, Bogle GC, Selvig KA. Influence of tooth instrumentation roughness on subgingival microbial colonization. J Periodontol. 1994;65:303–8. doi: 10.1902/jop.1994.65.4.303. [DOI] [PubMed] [Google Scholar]
- 13.Leknes KN, Lie T, Wikesjö UM, Böe OE, Selvig KA. Influence of tooth instrumentation roughness on gingival tissue reactions. J Periodontol. 1996;67:197–204. doi: 10.1902/jop.1996.67.3.197. [DOI] [PubMed] [Google Scholar]
- 14.Kubinek R, Zapletalova Z, Vujtek M, Novotný R, Kolarova H, Chmelickova H. Examination of dentin surface using AFM and SEM. Mod Res Educ Top in Microsc. 2007;11:593–8. [Google Scholar]
- 15.Ribeiro FV, Casarin RC, Nociti FH, Júnior, Sallum EA, Sallum AW, Casati MZ. Comparative in vitro study of root roughness after instrumentation with ultrasonic and diamond tip sonic scaler. J Appl Oral Sci. 2006;14:124–9. doi: 10.1590/S1678-77572006000200011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Selvig KA. Biological changes at the tooth-saliva interface in periodontal disease. J Dent Res. 1969;48:846–55. doi: 10.1177/00220345690480053901. [DOI] [PubMed] [Google Scholar]
- 17.Alvarez-Pérez MA, Alvarez-Fregoso O, Ortiz-López J, Arzate H. X-ray microanalysis of human cementum. Microsc Microanal. 2005;11:313–8. doi: 10.1017/S1431927605050221. [DOI] [PubMed] [Google Scholar]
- 18.Eide B, Lie T, Selvig KA. Surface coatings on dental cementum incident to periodontal disease. I. A scanning electron microscopic study. J Clin Periodontol. 1983;10:157–71. doi: 10.1111/j.1600-051x.1983.tb02204.x. [DOI] [PubMed] [Google Scholar]
- 19.Neiders ME, Eick JD, Miller WA, Leitner JW. Electron probe microanalysis of cementum and underlying dentin in young permanent teeth. J Dent Res. 1972;51:122–30. doi: 10.1177/00220345720510010501. [DOI] [PubMed] [Google Scholar]
- 20.Maidwell-Smith M, Wilson M, Kieser JB. Lipopolysaccharide (endotoxin) from individual periodontally involved teeth. J Clin Periodontol. 1987;14:453–6. doi: 10.1111/j.1600-051x.1987.tb02250.x. [DOI] [PubMed] [Google Scholar]
- 21.Wirthlin MR, Pederson ED, Hancock EB, Lamberts BL, Leonard EP. The hypermineralization of diseased root surfaces. J Periodontol. 1979;50:125–7. doi: 10.1902/jop.1979.50.3.125. [DOI] [PubMed] [Google Scholar]
- 22.Khounganian RM, Osman HI. Energy dispersive X-ray analysis of periodontally diseased and nondiseased human teeth using scanning electron microscopy. Egypt Dent J. 2006;52:1455–65. [Google Scholar]
- 23.Barton NS, Van Swol RL. Periodontally diseased vs. normal roots as evaluated by scanning electron microscopy and electron probe analysis. J Periodontol. 1987;58:634–8. doi: 10.1902/jop.1987.58.9.634. [DOI] [PubMed] [Google Scholar]