

Abstract
Spontaneous pneumomediastinum and subcutaneous emphysema (Hamman's syndrome) are rare but potentially dangerous complications of labour. The authors reported a case of a 23-year-old primigravida, admitted to our hospital for delivery after 40 weeks of pregnancy. She delivered a baby of 4.27 kg after 9 h from the start of labour. A few minutes after delivery, the patient developed dyspnoea and chest tightness, which made her doctor suspect pulmonary embolism. A chest X-ray and CT scan revealed pneumomediastinum and subcutaneous emphysema. The patient had been followed up for 3 days in our hospital, without specific therapy.
Background
Hamman's syndrome is a rare postpartum complication. The first case was recorded in 1784 and there are only 200 other cases that have been published. Diagnosis should be made early to avoid unnecessary investigations and to rule out other serious chest diseases such as pulmonary embolism. Hamman's syndrome is usually a benign condition, which may require no treatment or just symptomatic therapy.
Case presentation
A 23-year-old primigravida, non-smoking woman, was admitted to our hospital for delivery shortly after a rupture of the amniotic sac after 40 weeks of pregnancy, induced by a fall. Her medical history is unremarkable, except for a laparoscopic repair for incarcerated inguinal hernia 6 years ago. No postoperative complications have been reported. Throughout her pregnancy, she suffered from anaemia which was treated by iron supplement and urinary infections cured by antibiotics. She delivered a baby of 4.27 kg after 9 h from the start of labour, who was hypotonic and pale for a short time. A few minutes after delivery, the patient developed dyspnoea and chest tightness, which made her doctor suspect pulmonary embolism. A chest X-ray revealed pneumomediastinum with extension upward into the soft tissue of the neck bilaterally (figure 1). CT confirmed pneumomediastinum and subcutaneous emphysema and have excluded pulmonary embolism (figure 2). The patient had been followed up for 3 days in hospital, without a specific therapy. Repeat chest X-ray showed regression of subcutaneous emphysema (figure 3). The symptoms have disappeared and the patient had been discharged for follow-up in outpatient clinic.
Figure 1.
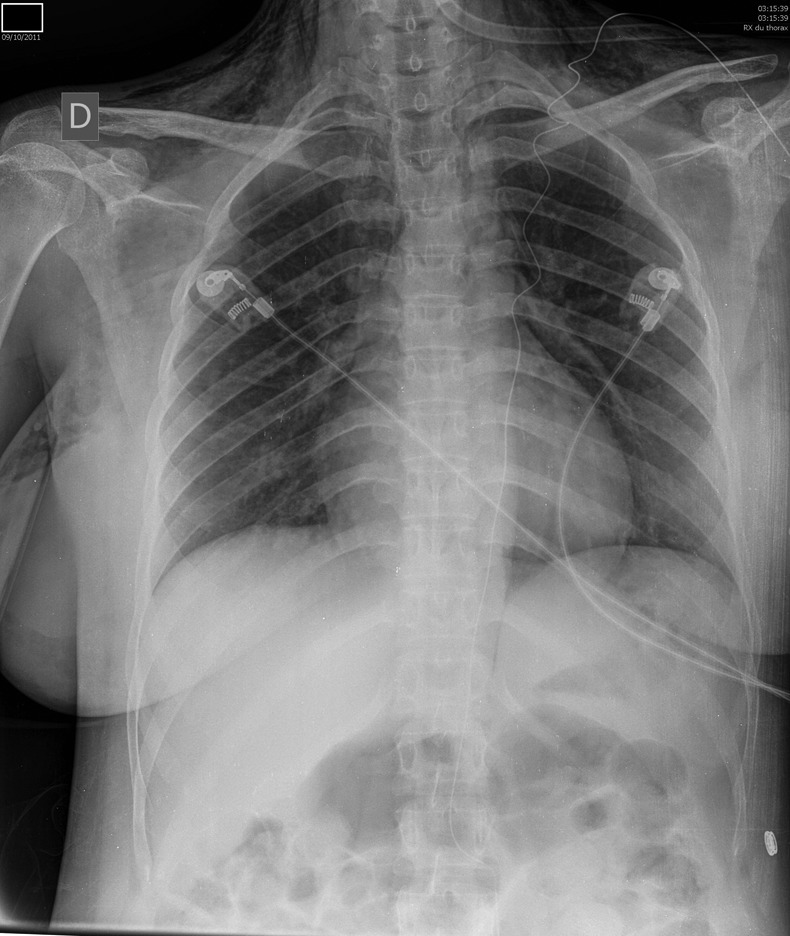
Initial chest X-ray showing a pneumomediastinum and subcutaneous emphysema.
Figure 2.

(A) CT scan of the chest showing free air in the mediastinum and in interstitial tissue (white arrow). (B) CT scan of the chest showing the pneumomediastinum displacing the vascular structures of the mediastinum, with extensive subcutaneous emphysema (asterisks). (C) Coronal reconstruction showing the pneumomediastinum. (D) Sagittal reconstruction showing free air under pleura interstitial tissue (white arrow).
Figure 3.

Chest X-ray of second day showing the clear regression of subcutaneous emphysema.
Differential diagnosis
Other aetiology of acute chest pain during or after labour are amniotic fluid embolism, pulmonary thrombus embolism, myocardial infarction, pneumothorax, aortic dissection, Boerhaave's syndrome, interstitial emphysema, pneumothorax, pneumopericardium, toxic effects of injected drugs, cardiac tamponade and mediastinitis.
Discussion
Simmons was the first who described a case of spontaneous pneumomediastinum during labour in 1793. According to some authors, the first documented case was in 1618 by the midwife of the Queen of France.1 Pneumomediastinum is the presence of air within the mediastinal spaces. It may occur secondary as a result of trauma or a pathological chest process or even spontaneously.
Postpartum pneumomediastinum in association with subcutaneous emphysema known as Hamman's syndrome is a rare complication of normal vaginal delivery. This syndrome was first described by Louis Hamman from Johns Hopkins Hospital in 1945.2 There are about 200 cases which have been reported in the last 400 years, with incidence about 1 in 100 000 vaginal delivery.3
The condition classically occurs in young, healthy primiparous women during the second stage of labour.4 However, clinical appearance, as in our case, may often be delayed until after delivery.
There are many theories that attempt to explain the causes of Hamman's syndrome. The most likely accepted one is the rupture of marginal pulmonary alveoli resulting from repetitive over inflations of the lungs and high intra-alveolar pressures during the second stage of labour.4 This can occur secondary to the Valsalva maneuvre as a result of continuous coughing, vomiting, screaming or pushing in labour. The increased intrathoracic pressure in the presence of decreased vascular calibre, establishes a pressure gradient into the vascular sheath which makes air dissect into the mediastinum. From the mediastinum, air migrates along fascial planes into the subcutaneous and retroperitoneal tissues.5 –7 Pneumothorax may coexist when air passes between visceral and parietal pleura.5
Chest pain is the most common symptom of Hamman's syndrome, other symptoms as cough, palpitations, dyspnoea, chest tightness, dysphagia and numbness of hands can be noted as well as palpable crepitus around the neck is pathognomonic.4 5 8
Pneumomediastinum should not be confused with other pathological conditions such as interstitial emphysema, pneumothorax and pneumopericardium, which mostly require specific types of management. Diagnosis of Hamman's syndrome as early as possible is important to exclude serious medical complications of pregnancy and labour that may require immediate treatment, such as pulmonary embolism, myocardial infarction, tension pneumothorax, aortic dissection and Boerhaave's syndrome.9 10
A chest X-ray is the single most important investigation to confirm the diagnosis, although CT is required if a standard X-ray is unhelpful and sometimes needed to rule out the other differential diagnosis.
In the absence of a pneumothorax that can cause cardiorespiratory collapse, Hamman's syndrome is usually a benign condition, which can resolve with bed rest or even with a conservative treatment within 2 weeks.7 Supportive management of Hamman's syndrome depends mainly on oxygen, analgesics and sedatives to relieve chest pain, dyspnoea and anxiety.
Malignant mediastinum is a very rare complication of massive pneumomediastinum in which acute collapse occurs and usually requires surgical intervention and splitting of the sternum to allow the escape of trapped air.7
Most cases have a self-limiting course like our case here, and recurrence is uncommon.6
Learning points.
Pneumomediastinum with subcutaneous emphysema is a rare complication of labour.
Its potential consequences require vigilance.
The main symptom is acute chest pain.
A definitive diagnosis is made radiographically.
CT scan confirm diagnosis and rule out other aetiology of acute chest pain.
Footnotes
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Gordon CA. Respiratory emphysema in labour. Am J Obstet Gynecol 1927;2013:633–46 [Google Scholar]
- 2.Hamman L. Mediastinal emphysema . JAMA 1945;2013:1–6 [Google Scholar]
- 3.Crean PA, Strong JM, FitzGerald MX. Spontaneous pneumomediastinum. Case report. Br J Obstet Gynaecol 1981;2013:952–4 [DOI] [PubMed] [Google Scholar]
- 4.Mahboob A, Eckford SD. Hamman's syndrome: an atypical cause of postpartum chest pain. J Obstet Gynaecol 2008;2013:652–3 [DOI] [PubMed] [Google Scholar]
- 5.Bonin MM. Hamman's syndrome(spontaneous pneumomediastinum) in a parturient: a case report. J Obstet Gynaecol Can 2006;2013:128–31 [DOI] [PubMed] [Google Scholar]
- 6.Tytherleigh MG, Connolly AA, Handa JL. Spontaneous pneumomediastinum. J Accid Emerg Med 1997;2013:333–4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Maier S, Graber P. Postpartum pneumomediastinum (Hamman's syndrome). CMAJ 2007;2013:32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Karson EM, Saltzman D, Davis MR. Pneumomediastinum in pregnancy: two case reports and review of literature. Pathophysiology and management. Obstet Gynecol 1984;2013(3 Suppl):39S–43S [PubMed] [Google Scholar]
- 9.Sutherland FW, Ho SY, Campanella C. Pneumomediastinum during spontaneous vaginal delivry. Ann Thorac Surg 2002;2013:314–15 [DOI] [PubMed] [Google Scholar]
- 10.Houari N, Labib S, Berdai MA, et al. Postpartum pneumomediastinum with subcutaneous emphysema: a case report. Ann Fr Anesth Reanim 2012;2013:728–30 [DOI] [PubMed] [Google Scholar]