

Abstract
Angiolipoma, spindle cell lipoma, myelolipoma, chondrolipoma and myxolipoma are histological variants of lipomas arising from fat tissue. Although angiolipoma is the most common tumour in the trunk and forearm, it occurs infrequently in the head and neck region. In this report we present a case of angiolipoma occurring in the buccal mucosa of a 33-year-old man. The patient had noticed a painless mass in his buccal mucosa for 2 months. The surgically removed tumour, measuring 4 × 4 cm in diameter was histologically evaluated. The tumour was composed of proliferations of mature fat cells and connective tissue containing many small blood vessels, which were evenly distributed.
Background
Lipomas are the most common benign mesenchymal tumours composed of mature adipocytes.1 They are well separated from the surrounding tissues by a thin fibrous capsule.2 They are usually slow-growing, soft and asymptomatic masses. The most common localisation of a lipoma is just below the surface of the skin, although it may be found anywhere in the body where adipose tissue is located.1 Even though these neoplasms tend to be highly vascular, identification of vessels is difficult because of compression. Lipomas are subclassified into multiple different histological subtypes based on the appearance of the associated stroma. Angiolipoma, spindle cell lipoma, myelolipoma, chondrolipoma and myxolipoma are some histological variants of lipomas.3
Although angiolipoma is the most common neoplasm seen in the trunk and extremities of young people, it occurs infrequently in the head and neck region. Angiolipoma is very rarely found in the soft tissue of the oral region, with only 21 reported cases.4 In this report, the authors present the clinical, macroscopical and histopathological features of infiltrating angiolipoma excised from the cheek.
Case presentation
A 33-year-old man with an apparently good general health was referred to K.M. Shah Dental College and Hospital, with swelling on the lower right side of the face since 2 months. It was not associated with pain, paresthaesia or discharge (figure 1). On extraoral examination, approximately 4 × 3 × 2 cm swelling extending from corner of mouth to 4 cm anterior to ear was present on right cheek (figure 2). The overlying skin was normal. Swelling was well circumscribed, soft in consistency, movable, tender, non-fluctuant and no bruit was present. On intraoral examination a non-fluctuant swelling of approximately 1 × 1 cm was noted (figure 3). Based on the clinical findings, leiomyoma, was given as provisional diagnosis.
Figure 1.

Extraoral clinical picture (front view).
Figure 2.

Extraoral clinical picture (side view).
Figure 3.

Intraoral clinical picture.
Investigations
Macroscopic examination revealed, a single bit of tissue which was 4 × 4 × 2 cm in size, irregular in shape, yellowish brown in colour, soft in consistency having irregular borders and rough surface (figure 4).
Figure 4.

Complete surgical removal of the lesion.
Microscopically, it was composed of proliferation of mature adipose cells intermixed with small-sized to medium-sized dilated blood vessels, infiltrating the underlying muscles (figure 5). The blood vessels were evenly scattered within the lesion (figure 6). The fat cells had no conspicuous cellular atypia (figure 7). There was a diffuse infiltration of chronic inflammatory cells. The tumour was non-encapsulated (figure 8). The histological features were suggestive of infiltrating angiolipoma.
Figure 5.

Gross specimen.
Figure 6.
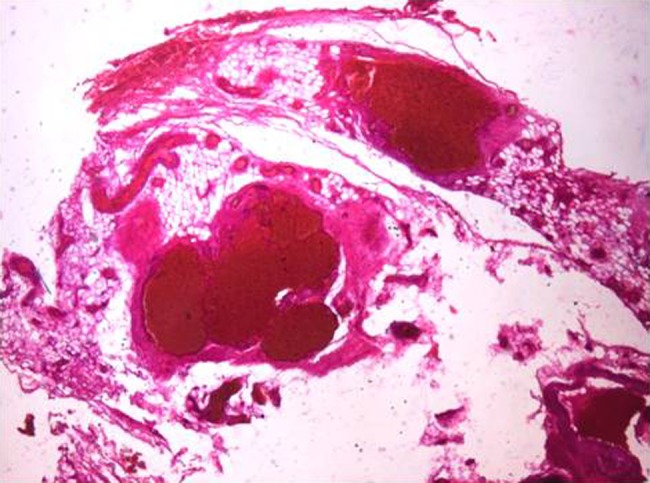
H&E (4×) histopathological view.
Figure 7.
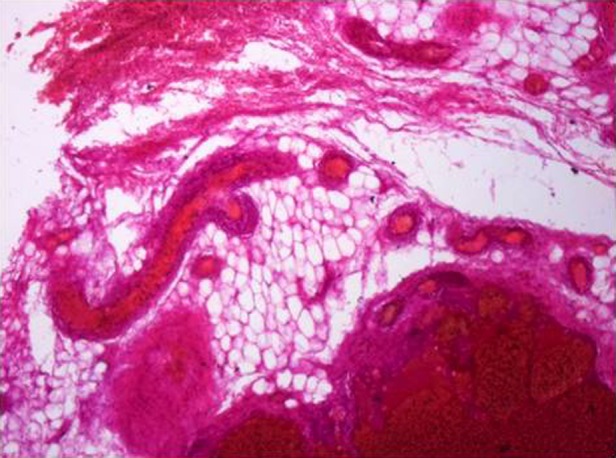
H&E (10×) histopathological view.
Figure 8.
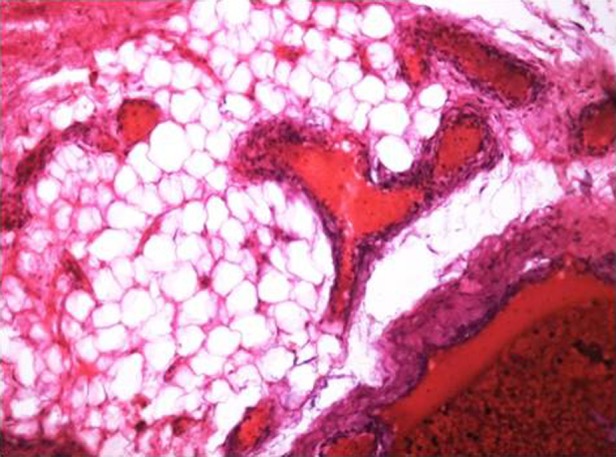
H&E (40×) histopathological view.
Differential diagnosis
On the basis of patient's history, clinical examination, diagnosis of haemangioma, leiomyoma, neurilemmoma was hypothesised.
Treatment
Surgical excision was performed under local anaesthesia through an extraoral approach (figure 4). Since it was not adhering to the surrounding tissue, detachment was easy and the mass was removed as a lump and sent for histopathological examination.
Outcome and follow-up
After surgical excision of the tumour and regular follow-up of the patient with clinical examination has not revealed any signs of recurrence until today.
Discussion
Angiolipoma was first described as a rare entity in 1912 by Bowen,5 but was established as a distinct entity in 1960 by Howard and Helwig.6 Later it was classified as infiltrating and non-infiltrating types depending on the histopathological features.7
Non-infiltrating angiolipomas are encapsulated. The size can vary from 1 to 4 cm. Angiolipomas tend to be located on the forearms, upper arms, thighs and anterior abdominal wall and are more common in men than in women. The face, scalp, palms or soles are hardly ever involved. Infiltrating angiolipomas are characterised by a non-encapsulated tumour and extend into surrounding tissues. They are usually diagnosed in older patients. They have two anatomical forms: intermuscular and intramuscular.4
The aetiology of lipoma is still unknown. It is believed that diabetes mellitus induced by hypercholesterolaemia and obesity, radiation and a familial or genetic link, such as abnormality of chromosome 12, may be involved in lipoma development.8 9 However, in the literature, trauma is also mentioned as one of the aetiological factors.8 There are two different opinions about the occurrence of so-called traumatic lipomas. The first is that, after trauma, adipose tissue prolapses through fascia, resulting in a direct impaction. The second opinion is that, after soft tissue trauma and haematoma formation, cytokines mediate differentiation and proliferation of preadipocytes, resulting in lipoma formation.9
Histopathological characteristics of angiolipomas include (1) gross evidence of tumour formation; (2) microscopic evidence of more than 50% of mature lipocytes in the tumour and (3) microscopic evidence of angiomatous proliferation.10 These were the findings in our case.
Differential diagnosis includes haemangioma, leiomyoma, neurilemmoma and Kaposi's sarcoma. The presence of phleboliths in CT, pulsation and fluctuation are helpful to rule out haemangioma. However, histopathological evaluation is required for exclusion of leiomyoma and neurilemmoma. Kaposi's sarcoma is a vascular malignancy, while lipoma is an adipose mesenchymal neoplasm. Palate, gingiva and tongue are the most common locations and clinically Kaposi's sarcoma occurs as ulcerative exophytic reddish lesion.
Surgical excision is the treatment for infiltrating and non-infiltrating angiolipomas. Carbon dioxide laser and liposuction may be alternative options for treatment of single or multiple angiolipomas. In the present case, we performed surgical excision. These lesions have been removed by both intraoral and external approaches depending on the relation of lesion to oral cavity. The intraoral approach has better cosmetic result.11 Most of the reported lesions were on mucosal side and were of smaller size and hence could be removed by intraoral route. Our patient had a lesion and was projecting from the outer side of the cheek hence this lesion was excised by external approach. An external approach was described to be safer by Aniceto et al.12
Generally, recurrences are very rare. The exception is for infiltrating angiolipoma, which have a recurrence rate of 35–50%.13 Our patient reported 6 months postoperatively without any discomforts and no signs of recurrence.
Learning points.
The diagnosis of angiolipoma is based on clinical as well as histopathological examination. Ultrasonography and fine needle aspiration cytology may be useful in diagnosis of angiolipoma.
The appropriate treatment for infiltrating and non-infiltrating angiolipoma is the surgical excision, with excision including the surrounding tissues recommended for an infiltrating angiolipoma in which the capsule is absent or partially associated with the tumour.
There is no evidence that angiolipomas undergo malignant transformation, due to the lack of atypia, pleomorphism or mitotic figure in angiomatous or adipose tissue.
Footnotes
Contributors: All the authors have contributed in preparing the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Auo HJ, Kang JM. Infiltrating angiolipoma of the nasopharynx: adjacent to an aberrant internal carotid artery. Auris Nasus Larynx 2009;2013:247–50 [DOI] [PubMed] [Google Scholar]
- 2.Regezi JA, Sciubba J. Oral pathology: clinicalpathologic correlations. 2nd edn Philadelphia: WB Saunders, 1993:235–7 [Google Scholar]
- 3.Williams TP, Stewart JCB. Soft tissue cysts and benign neoplasms. In: Fonseca RJ. ed. Oral and maxillofacial surgery. Philadelphia: WB Saunders, 2000:127–51 [Google Scholar]
- 4.Altug HA, Sahin S, Sencimen M, et al. Non-infiltrating angiolipoma of the cheek: a case report and review of the literature. J Oral Sci 2009;2013:137–9 [DOI] [PubMed] [Google Scholar]
- 5.Bowen JT. Multiple subcutaneous hemangiomas, together with multiple lipomas, occurring in an enormous numbers in an otherwise healthy muscular subject. Am J Med Sci 1912;2013:189–92 [Google Scholar]
- 6.Howard WR, Helwig EB. Angiolipoma. Arch Dermatol 1960;2013:924–31 [DOI] [PubMed] [Google Scholar]
- 7.Enzinger FM, Weiss SW. Soft tissue tumors. 3rd edn St Louis: Mosby, 1995:384–405 [Google Scholar]
- 8.Merscher S, Marondel I, Pedeutour F, et al. Identification of new translocation breakpoints at 12q13 in lipomas. Genomics 1997;2013:70–7 [DOI] [PubMed] [Google Scholar]
- 9.Aust MC, Spies M, Kall S, et al. Posttraumatic lipoma: fact or fiction? Skinmed 2007;2013:266–70 [DOI] [PubMed] [Google Scholar]
- 10.Hamdan AL, Mahfoud L, Rifai H, et al. Infiltrative angiolipoma of the neck. Middle East J Anesthesiol 2011;2013:433–4. [PubMed] [Google Scholar]
- 11.Aniceto GS, Saez RS, Penin AG. Angiolipoma of cheek: report of a case. J Oral Maxilloface Surg 1990;2013:512–15 [Google Scholar]
- 12.Ali MH, el-Zuebi F. Angiolipoma of cheek. J Oral Maxillofac Surg 1996;2013:213–15 [DOI] [PubMed] [Google Scholar]
- 13.Brki A, Özçamur Ç, Gürkan-Köseo˘glu B, et al. Angiofibrolipoma of the buccal mucosa: a case report. J Oral Sci 2010;2013:173–6 [DOI] [PubMed] [Google Scholar]