

Description
A 57-year-old man presented to us with epigastric pain, decreased appetite, weight loss (8 kg) for 2 months prior to presentation. He noted a lump on the left side of the neck for 15 days. He was a chronic smoker, smoking two packs of bidi per day for about 20 years. On examination, he had a 3.5×4 cm, firm, non-tender lump in the left supraclavicular region between the two heads of the sterno-cleidomastoid muscle, that is, Virchow's node (figure 1). Systemic examination was normal. An upper gastrointestinal (GI) endoscopy revealed an ulceroproliferative growth in the antrum (figure 2). A histopathological examination following the biopsy was consistent with adenocarcinoma.
Figure 1.

Enlarged node in the left supra-clavicular region.
Figure 2.
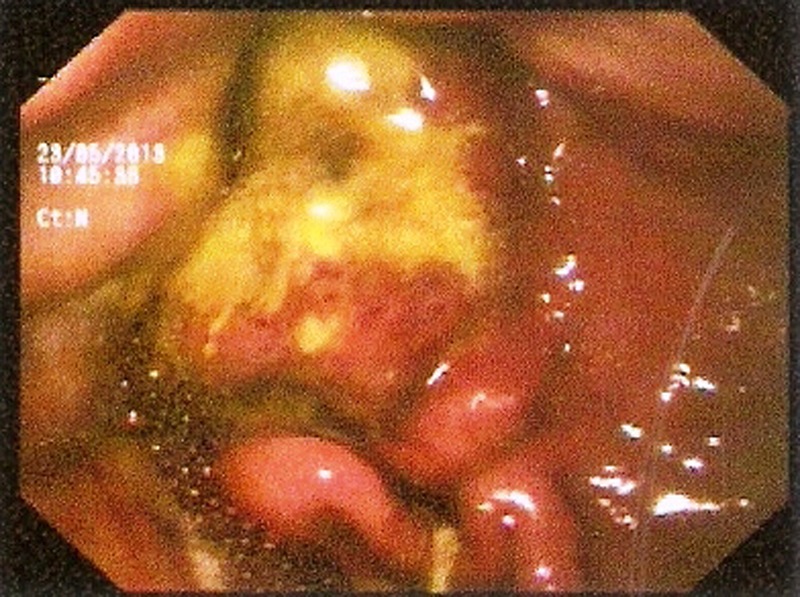
Upper gastrointestinal endoscopy showing ulceroproliferative growth in the antrum.
Virchow's node lies near to the junction of the thoracic duct and the left subclavian vein, where the lymph from most of the body drains into the systemic circulation.1 Tumour embolisation of the GI cancers via the thoracic duct usually leads to the enlargement of left supraclavicular node. The latter is called Troisier's sign and can be the first clue to a GI malignancy. For the same reason, they are also called sentinel or signal nodes. Stomach cancer primarily presenting with Troisier's sign without any other symptoms is very uncommon. It is important to know that metastasis to the supraclavicular lymph node indicates stage 4 disease. Although Virchow's node or the Troisier's node is typically enlarged in gastric cancer, it can also be seen in lymphoma, breast, oesophageal, pelvic and testicular cancers.2 Due to the poor performance status, we referred our patient for palliative therapy.
Learning points.
Due to superficial location and hence easy examination, Virchow's node enlargement is an important clue for the gastrointestinal (GI) malignancy.
It is a sign of advanced disease.
Virchow's node can also enlarge in non-GI malignancies like lymphoma, breast, oesophageal, pelvic and testicular cancers.
Footnotes
Contributors: DS and NK were involved in patient management, concept of paper, data acquisition, drafting the article, revision and final approval. SKD was involved in patient management, concept of paper, data acquisition, revision and final approval. MW involved in patient management, concept of paper, drafting the article, revision, final approval.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Baumgart DC, Fischer A. Virchow's node. Lancet 2007;2013:1568. [DOI] [PubMed] [Google Scholar]
- 2.Siosaki MD, Souza AT. Virchow's node. N Engl J Med 2013;2013:6. [DOI] [PubMed] [Google Scholar]