

Description
A newborn, weighing 2200 g, was delivered through caesarean section, at 35 weeks gestational age, for fetal distress. No antenatal scan had been performed. The neonate presented with severe respiratory distress shortly after birth and requiring urgent intubation. The chest X-ray (figure 1A) revealed a wide mediastinum with poor visualisation of the trachea. A tracheobronchogram, using water-soluble contrast medium (figure 1B), performed in the neonatal intensive care unit demonstrated severe narrowing of the trachea from tracheal midpoint up to and including the carina and origins of both main bronchi. The echocardiography confirmed a structurally normal heart. In addition a cystic fluid filled mass in the anteriorsuperior mediastinum was visualised. At flexible bronchoscopy anterior compression of the trachea with no structural tracheal stenosis was demonstrated. The chest CT (figure 2) confirmed a large, predominately low-density, non-enhancing, heterogeneous mass in the anterior mediastinum with posterior displacement and critical circumferential narrowing of the trachea. A congenital teratoma was suspected and complete surgical excision of the mass (60×40×22 mm) was performed on day 5 of life. Histology confirmed a benign grade 1 immature teratoma originating from the thymus. The neonate was successfully extubated 9 days postoperatively and made an uneventful recovery. At follow-up the infant remained asymptomatic.
Figure 1.
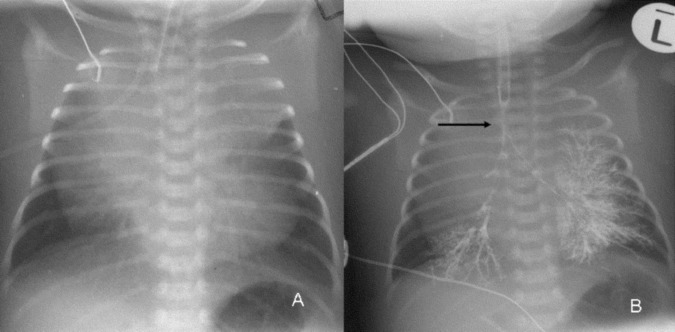
Plain frontal radiograph and frontal radiograph with tracheobronchography using a water-soluble contrast agent performed in the neonatal intensive care unit (ICU). (A) The frontal radiograph demonstrates an endotracheal tube in situ while the lower portions of the trachea are indistinct and presumed compressed. The wide mediastinum in the presence of a compressed trachea is therefore presumed to be pathological and suggestive of an anterior mediastinal mass possibly arising from the thymus. (B) Tracheobronchography performed using 2 mL of low-osmolar water-soluble contrast administered through the endotracheal tube was performed and in the neonatal ICU confirms severe narrowing of the midtrachea to lower trachea (arrow) presumably due to an anterior medistinal mass.
Figure 2.

Axial CT scan after intravenous contrast injection demonstrates posterior displacement of the great vessels, trachea and oesophagus as well as circumferential severe narrowing of the trachea (arrow) caused by a large anterior mediastinal mass of predominantly low density with minimal peripheral heterogenous enhancement. The mass origin was presumed to be the thymus.
Fetal mediastinal teratomas represent only 10% of congenital teratomas. Congenital mediastinal teratomas are rare congenital abnormalities.1 These lesions can present with unmanageable airway compression and acute cardiorespiratory failure.2 Treatment requires immediate recognition and complete surgical excision of the lesion. α-Fetoprotein blood levels can be used to monitor the presence of tumour cells.3 Before and after surgery these values were 60 390.8 and 9361.7 µg/L, respectively in our patient.
Other congenital mediastinal lesions that can present in the newborn period include bronchogenic cysts, bronchopulmonary foregut malformations, lymphangiomas and neuroblastomas. These congenital malformations can be suspected on fetal antenatal scanning so that optimal management can be planned.
Learning points.
Congenital teratoma can be the cause of an anterior mediastinal mass in a neonate.
Congenital teratoma can cause significant airway compression in a neonate.
Tracheobronchogram may be a useful investigation in neonates with suspected airway obstruction.
Footnotes
Contributors: AB was the treating doctor in this case. PG and RG were responsible for the investigation and the decisions about surgery. SA was responsible for the radiological investigations.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Schild RL, Plath H, Hofstaetter C, et al. Prenatal diagnosis of a fetal mediastinal teratoma. Ultrasound Obstet Gynecol 1998;2013:369–70 [DOI] [PubMed] [Google Scholar]
- 2.Tsao K, Albanese CT, Harrison MR. Prenatal therapy for thoracic and mediastinal lesions. World J Surg 2003;2013:77–83 [DOI] [PubMed] [Google Scholar]
- 3.Tjalma WA. The value of AFP in congenital cervical teratoma. J Pediatr Surg 2003;2013:1846. [DOI] [PubMed] [Google Scholar]