

Abstract
Background
Speech-like utterances containing rapidly combined consonants and vowels eventually dominate the prelinguistic and early word productions of toddlers who are developing typically (TD). It seems reasonable to expect a similar phenomenon in young cochlear implants (CI) recipients. This study sought to determine the number of months of robust hearing experience needed to achieve a majority of speech-like utterances in both of these groups.
Methods
Speech samples were recorded at 3-month intervals during the first 2 years of CI experience, and between 6- and 24 months of age in TD children. Speech-like utterances were operationally defined as those belonging to the Basic Canonical Syllables (BCS) or Advanced Forms (AF) levels of the Consolidated Stark Assessment of Early Vocal Development-Revised.
Results
On average, the CI group achieved a majority of speech- like utterances after 12 months, and the TD group after 18 months of robust hearing experience. The CI group produced greater percentages of speech-like utterances at each interval until 24-months, when both groups approximated 80%.
Conclusion
Auditory deprivation did not limit progress in vocal development as young CI recipients showed more-rapid-than-typical speech development during the first 2 years of device use. Implications for the Infraphonological model of speech development are considered.
Keywords: SPEECH DEVELOPMENT, CHILDREN, HEARING LOSS, COCHLEAR IMPLANTS, VOCAL DEVELOPMENT
The widespread adoption of newborn hearing screening has made it possible to identify children with severe-profound hearing losses during the first months of life. Identified infants typically receive hearing aids and begin family-centered communication intervention programs soon after a diagnosis has been made. In cases where the benefits from hearing aids are very limited, children often receive cochlear implants (CIs). CIs typically provide auditory access to speech at conversational intensity levels, or “robust hearing” (Ertmer & Inniger, 2009, p.1581). Experiencing robust hearing early in life has led to rapid advances in prelinguistic vocal development during the first year of CI use (e.g., Ertmer & Mellon, 2001; Ertmer, Young, & Nathani, 2007; Moore & Bass-Ringdahl, 2002; Schauwers, Gillis, Daemers, De Beuklaer, & Govaerts, 2004). The current investigation extends this work by examining the culmination of prelinguistic vocal development during the second year of robust hearing experience.
During the first 2 years of life, the utterances of infants who are typically developing (TD) change from near-exclusive production of grunts, squeals, isolated vowels, and vowel glides (se Oller, 2000; Vihman, 1996, for reviews), to abundant production of utterances in which consonants and vowels are combined with rapid, adult-like timing (i.e., canonical productions). Whereas the emergence of canonical utterances is one of the most well-documented signs of advancement in prelinguistic speech development for infants with normal hearing and young CI recipients (Eilers & Oller, 1994; Iyer & Olller, 2008; Lynch, Oller, & Steffens, 1989; Moeller et al. 2007; Nathani, Oller, & Neal, 2007; Oller, 1980; Oller & Eilers, 1988; Stark, 1980, 1983; Stoel-Gammon & Otomo, 1986; see Ertmer & Nathani Iyer, 2010 for review), comparatively little is known about the time-course by which these speech-like utterances become dominant in either group.
Prelinguistic Vocal Development Following Cochlear Implantation at a Young Age
The gradual acquisition of mature speech patterns during the first 2 years of life is known as prelinguistic vocal development (hereafter referred to as “vocal development”). This process consists of overlapping periods in which non-canonical vocalizations (e.g., grunts, vocalic sounds, and squeals in isolation or a series) decrease in frequency as a variety of canonical vocalizations (e.g., CV syllables, strings of CV syllables, and CVC syllables produced with adult-like timing) become increasingly common (Koopmans van Beinum & van der Stelt, 1986; Nathani, Ertmer, & Stark, 2006; Oller, 1980; Stark, 1980; Zlatin, 1975). Advances at the prelinguistic level overlap with first words and are considered fundamental for a developing a mature phonological system (Vihman, Macken, Miller, Simmons, & Miller, 1985). Documenting these advances requires a classification system that can be applied across the continuum of vocalization types produced during the first 2 years of life.
Several systems for classifying infant and toddler utterances have been used in studies of TD children and those with hearing loss (see Ertmer & Nathani Iyer, 2010; Oller, 2000; and Vihman, 1996 for reviews). As highlighted by Vihman (1996), these systems have been remarkably similar in characterizing different types of vocalizations and identifying the ages at which they emerge. However, one common drawback of the models proposed by Koopmans-van Beinum and van der Stelt (1986), Oller, (1980 and 2000), Roug, Landburg, and Lundberg (1989), and Stark, (1980; 1983) is that they do not characterize vocal development beyond 12 or 14 months of age. The current study sought to overcome this limitation by classifying utterances through 24 months of age, using the Consolidated Stark Assessment of Early Vocal Development-Revised (Consolidated SAEVD-R; Ertmer et al. 2007). The Consolidated SAEVD-R is a three-level system that is based on the Stark Assessment of Early Vocal Development-Revised (SAEVD-R; Nathani et al. 2006; See Table 1). Several studies have shown both of these systems to be reliable and valid measures of vocal development in TD infants (Nathani et al. 2006) and young CI recipients (Ertmer & Jung, 2012; Ertmer et al. 2007).
Table 1.
Levels of the Consolidated Stark Assessment of Early Vocal Development-Revised, ages of expected emergence for each level, and examples of vocalization types emerging at each level (Ertmer & Jung, 2012).
| Consolidated SAEVD-R Levels | Age of Emergence (months) | Example Vocalization Types |
|---|---|---|
| Precanonical vocalizations (PC) | ||
| Includes vocalizations from: SAEVD-R level 1. (Reflexive vocalizations), SAEVD-R 1evel 2. (Control of Phonation), and SAEVD-R level 3. (Expansion). | 0 – 2 | Crying, vegetative (coughs, hiccups), grunts (quasi-resonant nuclei) |
| 1 – 4 | Primitive vowel-like sounds with poor vocal quality (fully resonant nuclei), “goos”, closants ( e.g., clicks, smacks, trills) | |
| 3–8 | Squeals, vowels and vowel-like productions, consonants, marginal babbling** | |
| Basic Canonical Syllables (BCS) | 5 – 10 | Consonant-vowel syllables with rapid transitions (e.g., CV, CVCV, CVCVCV), whispered vocalizations, babbling |
| Advance Forms (AF) | 9 – 18* | Closed syllables (CVC), CCV syllables, diphthongs, VC syllables, jargon*** |
The ages in this table are based on children from English-speaking homes. Age of emergence for some Advance Form vocalization types may differ across languages (Vihman, 1993).
A series of primitive and slowly combined consonant and vowel-like productions.
More than two CV syllables containing at least two different consonant and vowel types and the presence of changes in intonation or stress pattern during the series (e.g. [gagadibut] with rising intonation pattern).
Recently, Ertmer and Jung (2012) used the Consolidated SAEVD-R to chronicle the attainment of two developmental milestones during the first year of CI use: the establishment of the Basic Canonical Syllables (BCS) and the Advanced Forms (AF) levels (see table 1). These levels were considered established when each comprised at least 20% of all child utterances during a speech sample. The main findings of the study were that, ~75% of young CI recipients had established the BCS level at ≥ 20% after 6 months, and the AF level after 12 months of CI experience. In comparison, the group average for younger, TD infants who had normal hearing first approached the 20% level for BCS vocalizations after 12 months of robust hearing experience (i.e., at 12 months-old), but seldom produced AF utterances during the first year of life. The CI-related findings were in agreement with earlier studies of the time-course for reaching canonical milestones (Ertmer & Mellon, 2001; Ertmer et al. 2007; Moore & Bass-Ringdahl, 2002; Schauwers et al, 2004). The accelerated progress of young CI users has been attributed to the effectiveness of the CI signal, communication intervention efforts, and the recipients’ comparatively advanced neurological, cognitive, social, and motor maturity. That is, it was hypothesized that the interaction of these factors enabled children to perceive the phonetic, timing, and structural aspects of mature speech models and incorporate them in their own speech more readily than younger, less mature TD children who had comparable amounts of robust hearing experience (Ertmer et al, 2007; Ertmer & Jung, 2012).
Although expeditious progress in reaching the BCS and AF milestones cited above suggests that the entire process of vocal development will be completed at a more-rapid-than-typical pace, this prediction has not been tested through a direct comparison with children who have normal hearing. The current investigation sought to extend previously cited milestone studies by determining the time-course for attaining a dominance of utterances containing canonical syllables (i.e., speech-like utterances). For the purposes of this study, speech-like utterances were operationally defined as those represented at the BCS and AF levels of the Consolidated SAEVD-R (See Table 1). Only one previously published study, to our knowledge, has examined the time-course for achieving a majority of speech-like utterances after cochlear implantation.
Ertmer et al. (2007) examined the amount of CI-assisted hearing experience needed to complete prelinguistic vocal development. In that study, six young CI recipients who had received a CI before the age of 3;0 contributed speech samples monthly during the first 2 years of device use. The percentages of Precanonical (PC), BCS, and AF utterances in each sample were then analyzed to determine the time-course for completing vocal development. Vocal development was considered “completed” (p. 400) when the BCS and AF levels each accounted for at least 20% of all utterances during two consecutive monthly samples, and the percentage of utterances at the PC level was less than those of the later-emerging levels. The participants’ individual profiles revealed that, on average, the criteria for completion of vocal development were met at 12.5 months. Data from Nathani et al, 2006) showed that TD children approximate this level between 16 and 20 months of age.
Rationale and Theoretical Implications
There are three compelling reasons to examine the amount of robust hearing experience needed to achieve a majority of speech-like utterances. First, cross-sectional data from Nathani et al, (2006) showed that TD toddlers eventually reach a level of proficiency in which speech-like productions become dominant over non-canonical productions. However, data were not collected at regular intervals for the same child. The current study provides new longitudinal data regarding the time-course for achieving this level of proficiency in children with normal hearing. If accelerated progress continues to be noted, then the effects of a pre-implant period of auditory deprivation on vocal development can be considered minimal or non-existent.
Second, whereas it has been shown that young CI recipients make rapid progress in attaining canonical milestones, the time-course for achieving a majority of mature, speech-like utterances has received little research attention to-date. If young CI recipients continue to make expeditious progress toward adult-like speech patterns during the later phases of vocal development, they will have narrowed the speech-development gap with TD children. However, if relatively slower progress toward speech-like dominance is observed, then the later phase of vocal development would not be completed as efficiently as predicted by earlier milestone studies. In either case, results will inform clinical practice as new, evidence-based timelines for achieving speech-like dominance in CI recipients are documented. These expectations will enable clinicians to identify children who are making slow progress and to make adjustments in intervention in a more timely fashion.
Third, very little is known about the proportions of BCS and AF utterances during the later phases of vocal development. Analyzing these kinds of utterances separately can provide new insights into developmental trends for English-learning children It is hypothesized that the earlier-emerging BCS utterances--although continuing to occur-- would decrease or plateau as AF utterances emerge during the second year of robust hearing experience. Such an outcome would be similar to the reductions of non-canonical productions (e.g., squeals, isolated vowels) observed as canonical syllables emerge. If found, relatively lower percentages of BCS utterances would suggest that they had provided scaffolds for the development of more complex and adult-like AF utterances. The current investigation will quantify this phenomenon for the first time and determine whether young CI recipients and TD toddlers produce similar proportions of these utterance types during the second year of robust hearing. Comparison of the BCS and AF levels also has the potential to expand the Infraphonological model of vocal development (Oller, 2000) by identifying speech production principles that children master during the second year of vocal development.
Like the SAEVD-R, the Infraphonological model classifies child utterances based on descriptive categories rather than phonetic transcription (see Oller, 2000 for discussion). The four age-related stages and the corresponding principles mastered at each stage of the Infraphonological model are presented in Table 2. A comparison of Tables 1 and 2 reveals that these models are highly similar through the first four developmental levels/stages, but that they differ in age-ranges studied and the acknowledgement of a level/stage beyond canonical syllable production (i.e., the Advanced Forms level of the SAEVD-R). A unique strength of the Infraphonological model is that specific developmental principles (i.e., newly acquired abilities), are identified for each stage. Comparisons of trends for BCS and AF utterances will help to determine whether later-emerging protophones (i.e., vocalizations that are precursors of mature speech; Oller 2000) are produced in sufficient quantity to indicate that new and enduring principles have been mastered by young CI recipients and TD children.
Table 2.
Infraphonological model of vocal development proposed by Oller (2000).
| Stage | Onset in Months | Protophone Mastered | Principle Mastered |
|---|---|---|---|
| Phonation | 0 – 2 | Quasivowels | Normal phonation |
| Primitive articulation | 1–4 | Gooing | Articulation |
| Expansion | 3 – 8 | Marginal babbling, full vowels, raspberries, squealing | Full resonance |
| Canonical | 5 – 10 | Canonical babbling | Rapid formant transition in CV syllables |
Research questions
Three research questions were addressed in this study. (1) How many months of robust hearing experience are needed for speech-like utterances (i.e., utterances containing canonical productions from the BCS and AF levels) to become a clear majority of young CI recipients’ productions? (2) Does the time-course for achieving a majority of speech-like utterances differ for young CI recipients and TD toddlers? To address these questions, a criterion of ≥60% speech-like utterances per sample was set to ensure that utterances from the BCS and AF levels of the Consolidated SAEVD-R outnumbered non-canonical utterances from the PC level by at least three to two. Based on previously discussed findings of more-rapid-than-typical progress in attaining milestones, it was hypothesized that the CI children would achieve a majority of speech-like utterances with fewer months of robust hearing experience than TD children. (3) What trends are evident in the proportions of BCS and AF utterances during the first 2 years of robust hearing experience? Based on the phonetically diverse and structurally complex nature of adult speech models and children’s maturing speech production abilities, it was hypothesized that later-emerging AF utterances would increase to a greater extent than earlier-emerging BCS utterances during the second year of robust hearing experience. This outcome would document the existence of a fifth level of vocal development and help to reveal the infraphonological principles acquired during the final phase of vocal development.
Methods
Participants
Two groups of children participated in the current study: young CI recipients and typically developing children. The CI group initially consisted of eleven girls and eight boys who were identified with severe to profound bilateral hearing losses through newborn hearing screening (n = 12) or by 25 months of age (n = 7). All received their CIs before their third birthdays and all devices were activated between 9 and 36 months of age (M = 20.91 months, SD = 8.42). All were enrolled in auditory-oral, family-centered intervention programs and were from English-speaking families. Several children were subsequently excluded for the current report because of secondary disabilities in addition to hearing loss (n = 4), moving to a different city before the second year of CI use (n = 2), or missing two recording sessions during the second year of CI use (n = 1). Of the 12 remaining children, seven had unilateral and five had bilateral CIs. Regarding race and ethnicity, nine children were non-Hispanic white, two were black, and one was Hispanic white. Several of the children with unilateral CIs also wore hearing aids (HA) for various amounts of time. Participants OHLE, ETKO, and ABHO and wore a HA with their CIs throughout the study. JORO discontinued hearing aid use after receiving his CI. JOIR and DAST discontinued wearing HAs after 5 and 9 months of CI use, respectively. AAWI wore a CI and a HA until 21 months post-activation. See Table 3 for more hearing and demographic information.
Table 3.
Hearing and demographic information for children in the CI group.
| Child | Gender | HL identified (months) | Age at 1st CI activation (months; ear) | Age at 2nd CI implanted (months) | Etiology | Device (Processing Strategy) | Pre-CI Pure- or warble-tone thresholds (Unaided better ear-dB HL) | Mean CI- aided thresholds (SF1 or better ear) last available audiogram (months post activation) | ISP2 |
|---|---|---|---|---|---|---|---|---|---|
| Unilateral | |||||||||
| JOIR | M | NHS2 | 12 (R3) | Unknown | Freedom (ACE4) | 106 | 29 (19) | 25 | |
| DAST | M | 11 | 21 (R) | Malformed cochlea | Freedom (ACE) | 76; NR5≥4k | 26 (23 ) | 44 | |
| OLHE | F | NHS | 25 (R) | Unknown/ Dysplasiaa | Freedom (ACE) | 80 | 26 (24) | 66 | |
| ETKO | M | 20 | 26 (L6) | Complicated b | Freedom (ACE) | 90; NR≥4k | 22 (18) | 26 | |
| ABHO | F | NHS | 27 (L) | Unknown | PSP7 (HiRes- P8) | 89 | 23 (22 ) | 48 | |
| AAWI | F | 22 | 36 (R) | Cytomegalo virus | Freedom (ACE) | NR | 22.5 (24) | 40 | |
| JOROc | F | NHS | 36 (R) | Unknown | Freedom (ACE) | 96; NR≥2k | 18 (23) | 16 | |
| Bilateral | |||||||||
| OWJO | M | NHS | 9 | 22 | Unknown | Freedom (ACE) | NR | 16.7 (25) | 72 |
| MAJE | M | NHS | 13 | 13 | Connexin 26 | Freedom (ACE) | NR | 21.7 (20) | 52 |
| GIAI | F | NHS | 13 | 27 | Unknown | Freedom (ACE) | 100 | 20 (23) | 66 |
| MAMA | F | 13 | 18 | 20 | Unknown | Freedom (ACE) | 100 | 25 (21) | 12 |
| JAWE | F | NHS | 19 | 38 | Connexin 26 | PSP and Harmony (HiRes-P) | 87.5 | 39 (24) | 40 |
| Mean | 21.25 | 24.00 | 24.08 (22.17) | 42.25 | |||||
| SD | 9.00 | 9.30 | 5.85 (2.21) | 19.82 |
Bulbous deformity on apical turns bilaterally,
Apnea of prematurity, indirect hyperbilirubinemia, ototoxic medication exposure, presumed sepsis, and cerebellar hemorrhage, and
JORO was identified with a mild bilateral loss by ABR testing at 1 month; bilateral mild to severe loss at 19 months, and a moderately severe to profound loss (right ear) with a severe to profound hearing loss (left ear) at 20 months of age
Sound Field,
Nittrouer Index of Social Position (Nittrouer, & Burton, 2005), Newborn Hearing Screening,
Right,
Advanced Combination Encoder,
No response to pure- or warble-tones,
Left,
Platinum Series™ Sound Processor, and
HiResolution-Paired.
Family ISP level = {Father’s level}+{Mother’s level}, each parent’s level = (education score: 1–8) X (occupation score: 1–8). The maximum score for a family’s ISP is 128. Scores for single-parent families are doubled.
Twelve children (seven boys and five girls) who were typically developing were enrolled in the study at 6 months old. Eleven were non-Hispanic white children and one was of multiple races. These children had passed newborn hearing screening and were reported to have no hearing, developmental, behavioral, or learning difficulties by their parents upon enrollment and throughout the study. The children were not matched to the CI group in terms of gender because gender has not been found to affect the age of emergence of canonical productions (Oller, Eilers, Basinger, Steffans, & Urbano, 1995). One male child was excluded from data analysis after a speech delay was diagnosed at 24 months, and so the TD group consisted of 11 children. Although the children in the CI group were older than the TD controls (i.e., M = ~45 months vs 24 months at the end of the study), both groups were considered to have the same number of months of robust hearing experience at each data collection interval. Both the TD and the CI children were part of an earlier study of the first year of post-implantation vocal development (Ertmer & Jung, 2012).
The socio-economic status of children in each group was examined through the Index of Social Position (ISP; Nittrouer & Burton, 2005). This parent-interview tool yields information about occupation and educational levels. ISP scores were calculated using a modified procedure for single parent families in which the score of a single parent was doubled to make it comparable to that of families with two parents (Nittrouer, personal communication; February, 2008). All but one child in the CI group were from homes with two parents. More information about the ISP can be found in the footnotes for Table 3. Comparisons between the two groups showed a significant difference between the two groups of children, t (21) = 3.123, p <.005, with the ISP scores of TD group (M = 68.27, SD = 20.09) greater than those of the CI group (M = 42.25, SD = 19.82). Although a relationship between socio-economic status and advancements in vocal development has not been found among children with normal hearing (Oller et al, 1995), ISP scores were compiled as a possible explanatory factor in the event that longer time-courses for achieving a majority of speech-like utterances were noted in the CI- as compared to the TD-group. Classification of ISP scores into Low-, Mid-, or High-SES levels has not been reported previously (Nittrouer, 1996; Nittouer & Burton, 2005), and so ISP values were only used to compare the two groups of children rather than to characterize socio-economic status.
Research Design and Data Collection
A prospective, longitudinal research design was used to examine changes in children’s utterances during adult-child play interactions. Twenty-minute video- and audio- recordings were made at 10 intervals during the first 2 years of CI use (i.e., pre-implantation, early [within 2 months of CI activation], and 3, 6, 9, 12, 15, 18, 21, and 24 months after device activation for the CI group). Recordings of the TD children began at 6 months old and were repeated at 9, 12, 15, 18, 21, and 24 months of age. Data collection for the TD children was not begun prior to 6 months of age because speech-like, canonical vocalizations are not expected to be established before that age (Nathani et al. 2006; Oller, 1980; Stark, 1980). Time-courses for reaching vocal development milestones during the first year of CI use were recently reported by Ertmer and Jung (2012). The current study extended this work by examining the percentages of speech-like utterances (i.e., BCS + AF) in sessions recorded between 6 and 24 months of device use for the CI group, and between 6 months and 24 months of age for the TD group. Except for missing data from one session (participant JAWE at 6 months post-activation) all children contributed samples at every interval.
Sony mini-DVD camcorders (model number DCR-DVD405) were coupled with Bluetooth wireless microphones to make audio- and video-recordings. This camcorder digitally records audio-and video directly onto mini-DVD discs. The microphones were worn by the children in a pocket of specially designed vests so that a consistent microphone-mouth distance of less than 4 inches was maintained. Recordings of children in the CI group were made in small rooms at their intervention centers. Parents interacted with the young CI recipients in approximately 74% of these sessions. Familiar early interventionists interacted with the child whenever parents were not available. All of the recordings of TD children were made in the Speech Development Laboratory at Purdue University and a parent was involved in every session. Adults were instructed to play with the child in their usual way using a set of toys that was the same for each interaction and both groups of children. The sets included books, puzzles, dolls, cars, toy animals, and toy food items. The children were encouraged to pick out the toys they desired to play with at the start of each session.
Data Analysis
DVDs of adult-child interactions were reviewed and 50 consecutive child utterances from each session were parsed from DVD recordings and saved as individual digital audio files (.wav) using KayPENTAX Multi-Speech software. The operational definition of an “utterance” was based on previous studies of vocal development: an utterance is a vocalization or group of vocalizations separated from all others by either audible ingressive breath or by judges’ intuitions about utterance boundaries which are often indicated by a silence of one second or longer (Lynch, Oller, Steffens, & Buder, 1995; and Stark, 1980). Only utterances that appeared to be precursors for speech (i.e., protophones; see Oller, 2000 for discussion) were parsed and analyzed. Vegetative sounds such as burping, sneezing, and hiccups, and crying and laughing were excluded because they do not become more speech-like as children mature. The first 50 consecutive child utterances, or all utterances from sessions yielding less than 50 utterances, that were adequate in intensity and without excessive background noise or talk-over were classified using definitions from the Consolidated SAEVD-R (discussed below). Utterances of poor audio quality were discarded and replaced with the next consecutive utterance of acceptable quality. Out of 160 sessions, 90% (n = 144) contained a minimum of 50 child utterances. Approximately 3.6 % (n = 3) of sessions for CI children, and 17 % (n = 13) of sessions for TD children contained fewer than 50 utterances. On average, these shorter sessions yielded 33 (SD = 16.5) and 39.6 (SD = 12.4) utterances for the two groups, respectively.
Each selected utterance was saved as a digital sound-file and assigned a special code representing the child, the interval of the sample, and the number of the utterance within the sample (e.g. third of 50 utterances). This coding system ensured that the listener-judges who later classified child utterances were blind to the children’s hearing status (CI or normal) and the monthly interval at which the recording was made. Sound-files alone were used to classify vocalizations because video recordings can provide information about the presence or absence of a CI, the child’s age, and social communication contexts that might influence judgments when classifying vocalizations.
The operational definitions of the SAEVD-R (Nathani et al. 2006) were used to classify child utterances from sound-files. Utterances were then assigned into one of three categories of the Consolidated SAEVD-R (See table 1.): Precanonical (PC), Basic Canonical Syllables (BCS), or Advanced Forms (AF). These assignments were made to non-meaningful utterances as well as those containing recognizable spoken words. Using the Consolidated SAEVD-R, vocalization types from SAEVD-R levels 1 – 3 were classified as PC vocalizations because they lacked vowels and true consonants in combination with rapid transitions between them (Ertmer et al, 2007). Nathani et al. (2006) found that PC vocalizations are dominant before 8 months of age and decreased in frequency during the second year of life in TD children. PC vocalizations are produced by deaf and hearing infants alike and the frequency of these vocalizations does not appear to be affected by hearing status during the first year of life (Ertmer & Mellon, 2001; Ertmer et al. 2007; Nathani et al. 2006).
Child utterances were classified as BCS when they were produced with normal phonation and had at least one CV combination with a rapid transition (Oller & Lynch, 1992). Nathani et al. (2006) demonstrated that BCS vocalization types (e.g., CV, CVCVCV syllables) begin to emerge around 5 months of age and increase substantially after 9 months of age before accounting for approximately 40% of children’s output by 20 months of age. Deaf children have shown delays in the establishment of BCS utterances compared to infants who are TD (e.g., Oller & Eilers, 1988).
Utterances were classified as AFs when they were perceived as having the timing and composition characteristics of BCS but were relatively more phonetically, structurally, and/or prosodically complex. Examples include closed syllables such as VC, and CVC syllables, CCV syllables, and jargon (see table 1 for definition). AF vocalizations typically begin to emerge after 9 months and approximately 20% of children’s utterances contain AFs by 16 – 20 months of age (Nathani et al. 2006). These productions have rapid formant transitions and are readily recognized as adult-like productions through auditory-perceptual analysis. With the exception of isolated diphthongs, all of the vocalization types from the BCS and AF levels meet the requirements for canonical productions. Isolated diphthongs have been shown to emerge relatively late in vocal development (Nathani et al. 2006) and were classified at the AF level whenever they were perceived to have full resonances, rapid transitions and, adult-like durations (e.g., [aU] [aI]. Abnormally slow productions of vowel combinations were considered vowel glides rather than diphthongs, and classified at the PC level (see Nathani et al. 2006, for operational definitions).
Because children’s utterances often contain more than one kind of vocalization, each utterance was classified according to the most advanced vocalization type within it. This was done to ensure that the child’s highest level of ability was represented for each utterance. For example, an utterance that contained an isolated vowel, a squeal, and a CVCV syllable was classified at the BCS level because the CVCV syllable was the most advanced type of vocalization within the utterance. It is recognized that the frequency of speech-like vs. non-speech-like vocalizations may be different from the outcomes of the current analysis of utterances. However, as the utterance (including all vocalizations within it) has been the focus of analysis in prior studies of vocal development (Oller, 1980; Nathani et al. 2006; Stark, 1980), the current investigation examined changes at this level of analysis.
Reliability
A total of 7,812 utterances were originally classified into the PC, BCS, or AF categories by five graduate research assistants who were trained to use the SAEVD-R. Approximately 9% of these utterances were randomly selected and re-classified to assess intra-classifier (695 utterances) and inter-classifier (747 utterances) reliability. Reclassifications were completed 1 to 12 months after the original classification was made. Cohen’s Kappa was calculated to determine how well the original and second classifications concurred when corrected for chance agreement. A value of k = .97 was determined for intra-classifier agreement (point-to-point agreement = 99%), and a value of k = .89 was found for inter-classifier agreement (point-to-point agreement = 95%). Kappa values of greater than .75 have been characterized as excellent agreement by Fleiss (1981).
Statistical Analyses
A Generalized Linear Mixed Longitudinal model (GLMIX) was used to analyze the data. Because children with unilateral CIs and those with bilateral CIs were not significantly different in the number of months needed to achieve a majority of speech-like utterances (M = 9 and 11 months, respectively; t = 0.11) their data were analyzed together. The percentage of speech-like vocalizations served as the dependent variable, with Group (CI and TD) as the between-group variable and Interval (months 6 –24) as a within-group variable. To complete the statistical analysis, the raw number of utterances that were classified into the PC, BCS, and AF levels in each individual session, were converted to percentages. This step was taken for enable comparisons using data from sessions with fewer than 50 utterances. Percentage data were then modified through an arcsine transformation prior to examine the of main effects and interactions of Group (CI vs. TD) and Interval (sessions at 6, 9, 12, 15, 18, 21, and 24 months of robust hearing). Descriptive statistics were examined to characterize trends for BCS and AF vocalizations during the later phases of the study for these two groups of children.
Results
Following arcsine transformation of percentage scores, GLMX testing revealed significant main effects of Group f (1, 21) = 38.53, p <0.0001 and Interval f (7, 21) = 26.14, p <0.0001. Specifically, the CI group produced a greater percentage of speech-like utterances than the TD children when data from all intervals are summed. Further, significant differences in the percentage of speech-like utterances were observed across intervals when data for both the CI and TD groups were combined. A significant Group X Interval interaction was also determined f (6, 21) = 2.91, p = 0.0315, indicating that group scores across the intervals were not always different from each other.
Between-group post hoc analyses (Bonferroni t-tests, alpha p ≤0.05) were completed to determine the intervals at which the proportions of speech-like vocalizations differed for the two groups. The results of this comparison are presented in Figure 1. From this figure it can be seen that, for the CI group, the mean percentages of speech-like utterances increased steadily from 40% at 6 months to 83% at 24 months of robust hearing experience. Means also increased for the TD group, rising from <5% to 78% during the same period. CI group means were significantly greater than TD means at the every interval except the 24 months interval.
Figure 1.
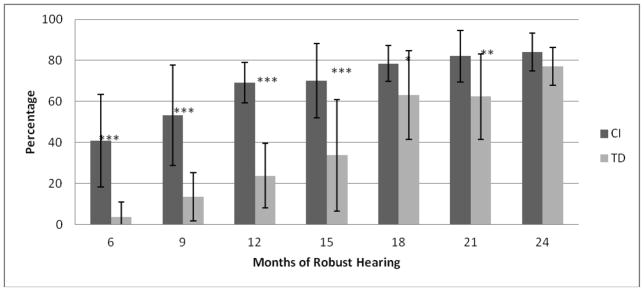
Comparisons of the percentages of speech-like utterances produced by the CI and TD groups at each interval.
* < 0.05; ** <0.01; *** < 0.001
In addition to group data, individual scores can provide insight into the time-course for achieving a majority of speech-like productions. From tables 4 and 5 it can be seen that individuals in the CI group made more rapid gains than those in the TD group. All CI users reached the 60% criterion for dominance of speech-like utterances at 18 months of CI experience (Figure 2; Table 4). All TD participants first met the same criterion at the 24 month interval (Figure 2; Table 5.).
Table 4.
Percentages of Precanonical (PC), Basic Canonical Syllables (BCS), Advanced Forms (AF) and Speech-like utterances (SL = [BCS + AF]) at each sampling interval for individuals in the CI group.
| CI children: | OWJO | JOIR | GIAI | MAJE | MAMA | JAWE | DAST | OLHE | ETKO | ABHO | JORO | AAWI | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age at activation (months): | 9 | 12 | 13 | 13 | 18 | 19 | 21 | 25 | 26 | 27 | 36 | 36 | |
| 6 months | PC | 71 | 68 | 80 | 100 | 58 | 48 | 28 | 76 | 46 | 26 | 50 | |
| BCS | 29 | 30 | 6 | 0 | 36 | 38 | 44 | 16 | 46 | 38 | 36 | ||
| AF | 0 | 2 | 14 | 0 | 6 | 14 | 28 | 8 | 8 | 36 | 14 | ||
| SL | 29 | 32 | 20 | 0 | 42 | 52 | 72 | 24 | 54 | 74 | 50 | ||
|
| |||||||||||||
| 9 months | PC | 58 | 18 | 92 | 90 | 36 | 36 | 32 | 24 | 64 | 26 | 44 | 42 |
| BCS | 30 | 44 | 6 | 6 | 54 | 30 | 30 | 50 | 22 | 16 | 40 | 22 | |
| AF | 12 | 38 | 2 | 4 | 10 | 34 | 38 | 26 | 14 | 58 | 16 | 36 | |
| SL | 42 | 82 | 8 | 10 | 64 | 64 | 68 | 76 | 36 | 74 | 56 | 58 | |
|
| |||||||||||||
| 12 months | PC | 34 | 16 | 28 | 38 | 46 | 28 | 34 | 36 | 18 | 16 | 40 | 36 |
| BCS | 40 | 36 | 42 | 40 | 38 | 64 | 24 | 28 | 40 | 26 | 32 | 24 | |
| AF | 26 | 48 | 30 | 22 | 16 | 8 | 42 | 36 | 42 | 58 | 28 | 40 | |
| SL | 66 | 84 | 72 | 62 | 54 | 72 | 66 | 64 | 82 | 84 | 60 | 64 | |
|
| |||||||||||||
| 15 months | PC | 48 | 14 | 30 | 76 | 32 | 18 | 12 | 22 | 24 | 18 | 22 | 42 |
| BCS | 41 | 52 | 52 | 22 | 44 | 64 | 34 | 46 | 30 | 34 | 44 | 42 | |
| AF | 11 | 34 | 18 | 2 | 24 | 18 | 54 | 32 | 46 | 48 | 34 | 16 | |
| SL | 52 | 86 | 70 | 24 | 68 | 82 | 88 | 78 | 76 | 82 | 78 | 58 | |
|
| |||||||||||||
| 18 months | PC | 24 | 20 | 20 | 38 | 24 | 18 | 8 | 34 | 8 | 20 | 22 | 22 |
| BCS | 46 | 28 | 52 | 26 | 22 | 34 | 38 | 46 | 48 | 20 | 22 | 38 | |
| AF | 30 | 52 | 28 | 36 | 54 | 48 | 54 | 20 | 44 | 60 | 56 | 40 | |
| SL | 76 | 80 | 80 | 62 | 76 | 82 | 92 | 66 | 92 | 80 | 78 | 78 | |
|
| |||||||||||||
| 21 months | PC | 34 | 2 | 12 | 40 | 30 | 18 | 2 | 27 | 12 | 10 | 8 | 20 |
| BCS | 30 | 38 | 30 | 28 | 26 | 58 | 16 | 27 | 34 | 20 | 28 | 30 | |
| AF | 36 | 60 | 58 | 32 | 44 | 24 | 82 | 46 | 54 | 70 | 64 | 50 | |
| SL | 66 | 98 | 88 | 60 | 70 | 82 | 98 | 73 | 88 | 90 | 92 | 80 | |
|
| |||||||||||||
| 24 months | PC | 30 | 12 | 18 | 12 | 32 | 12 | 2 | 22 | 18 | 6 | 6 | 20 |
| BCS | 22 | 20 | 44 | 26 | 20 | 50 | 20 | 30 | 24 | 12 | 48 | 48 | |
| AF | 48 | 68 | 38 | 62 | 48 | 38 | 78 | 48 | 58 | 82 | 46 | 32 | |
| SL | 70 | 88 | 82 | 88 | 68 | 88 | 3598 | 78 | 82 | 94 | 94 | 80 | |
Table 5.
Percentages of Precanonical (PC), Basic Canonical Syllables (BCS), Advanced Forms (AF) and Speech-like utterances (SL = [BCS + AF]) at each sampling interval for individuals in the TD group.
| TD children: | COKU | FACO | HOWA | ISIL | LIRO | OLHA | PARI | SASN | SYNE | TRTO | WIAB | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 6 months | PC | 96 | 76 | 100 | 100 | 100 | 100 | 100 | 98 | 100 | 91 | 98 |
| BCS | 2 | 24 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 2 | |
| AF | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | |
| SL | 4 | 24 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 9 | 2 | |
|
| ||||||||||||
| 9 months | PC | 89 | 92 | 77 | 64 | 100 | 90 | 100 | 96 | 87 | 85 | 70 |
| BCS | 11 | 8 | 15 | 32 | 0 | 10 | 0 | 4 | 6 | 6 | 18 | |
| AF | 0 | 0 | 8 | 4 | 0 | 0 | 0 | 0 | 6 | 8 | 12 | |
| SL | 11 | 8 | 23 | 36 | 0 | 10 | 0 | 4 | 13 | 15 | 30 | |
|
| ||||||||||||
| 12 months | PC | 84 | 94 | 46 | 86 | 100 | 62 | 84 | 72 | 62 | 80 | 68 |
| BCS | 16 | 6 | 44 | 14 | 0 | 32 | 16 | 22 | 34 | 20 | 12 | |
| AF | 0 | 0 | 10 | 0 | 0 | 6 | 0 | 6 | 3 | 0 | 20 | |
| SL | 16 | 6 | 54 | 14 | 0 | 38 | 16 | 28 | 38 | 20 | 32 | |
|
| ||||||||||||
| 15 months | PC | 94 | 92 | 30 | 65 | 36 | 78 | 92 | 82 | 16 | 76 | 68 |
| BCS | 6 | 8 | 52 | 33 | 44 | 18 | 8 | 18 | 54 | 22 | 28 | |
| AF | 0 | 0 | 18 | 2 | 20 | 4 | 0 | 0 | 30 | 2 | 4 | |
| SL | 6 | 8 | 70 | 35 | 64 | 22 | 8 | 18 | 84 | 24 | 32 | |
|
| ||||||||||||
| 18 months | PC | 17 | 54 | 16 | 34 | 36 | 66 | 32 | 54 | 22 | 22 | 80 |
| BCS | 33 | 36 | 30 | 44 | 54 | 28 | 32 | 36 | 36 | 54 | 20 | |
| AF | 50 | 10 | 54 | 22 | 10 | 6 | 36 | 10 | 42 | 24 | 0 | |
| SL | 83 | 46 | 84 | 66 | 64 | 34 | 68 | 46 | 78 | 78 | 20 | |
|
| ||||||||||||
| 21 months | PC | 28 | 52 | 6 | 18 | 27 | 44 | 52 | 28 | 46 | 24 | 76 |
| BCS | 26 | 44 | 36 | 16 | 39 | 31 | 24 | 48 | 36 | 69 | 24 | |
| AF | 46 | 4 | 58 | 66 | 35 | 25 | 24 | 24 | 18 | 7 | 0 | |
| SL | 72 | 48 | 94 | 82 | 73 | 56 | 48 | 72 | 54 | 76 | 24 | |
|
| ||||||||||||
| 24 months | PC | 26 | 12 | 14 | 26 | 18 | 16 | 16 | 20 | 30 | 31 | 40 |
| BCS | 4 | 38 | 24 | 8 | 20 | 36 | 52 | 34 | 30 | 12 | 20 | |
| AF | 70 | 50 | 62 | 66 | 62 | 48 | 32 | 46 | 40 | 57 | 40 | |
| SL | 74 | 88 | 86 | 74 | 82 | 84 | 84 | 80 | 70 | 69 | 60 | |
Figure 2.
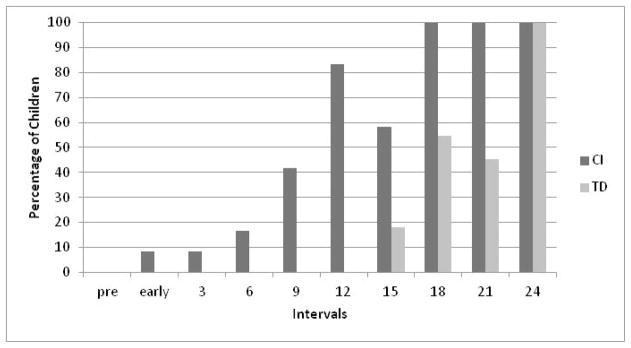
Percentage of children who produced speech-like utterances at least 60% of the time at each interval.
Trends for BCS and AF Utterances
The percentages of BCS and AF utterances for the CI and TD groups are presented in figures 3 and 4, respectively. In general, the BCS utterances were produced more frequently than AF through the first 15 – 18 months of robust hearing experience and both groups reached a maximum of approximately 40% during this time. BCS scores then decreased slightly for both groups. In contrast, AF utterances emerged more slowly but increased steadily before becoming the most common type of speech-like utterance toward the end of the study. Speech samples for the two groups contained nearly-identical percentages of AF utterances after 2 years of robust hearing (i.e., 54% for CI and 52% for TD children).
Figure 3.

Mean percentages of BCS and AF utterances produced at each interval by the CI group.
Figure 4.

Mean percentages of BCS and AF utterances produced at each interval by the TD group.
Two main developmental trends are revealed by the means presented in Figures 3 and 4. First, increases in BCS vocalizations were observed until 15 months in the CI group and 18 months in the TD group. Decreases or plateaus in BCS percentages were noted after those intervals. Second, the percentages of AF vocalizations increased substantially between 6 and 24 months for the CI group, and between 15 and 24 months for the TD group. Regarding the CI group, the latter trend indicates that, by the 24 month interval, AF utterances had increased to more than double the levels previously observed after 12 months of CI use (i.e., Mean BCS = ~38% and Mean AF = ~25%; Ertmer & Jung, 2012). Scores for individual CI and TD participants can be found in Tables 4 and 5, respectively.
Discussion
Time-course for achieving a majority of speech-like utterances
Previous investigations of vocal development in young CI recipients have found that early- and mid-developmental milestones (i.e., the emergence and establishment of Basic Canonical Syllables and Advanced Forms) have been reached with fewer months of robust hearing experience than seen in TD infants (Ertmer & Mellon, 2001; Ertmer et al, 2007; Moore & Bass-Ringdahl, 2002; Schauwers et al, 2004). The current investigation demonstrated that this expeditious rate of progress continued as children shifted from mainly Precanonical utterances to a majority of speech-like utterances (i.e., utterances containing canonical productions from the BCS and AF levels) during the second year of CI use. On average, the CI group achieved a majority of speech-like utterances with fewer months of robust hearing experience than younger, TD children (i.e., 12 vs. 18 months, respectively). The number of required months was, on average, quite similar to findings of the Ertmer et al. (i.e., 12.5 months; 2007) study and consistent across individual participants. As Figure 2 and Table 4 show, every CI user met the 60% criterion after18 or fewer months of CI-assisted hearing experience. In contrast, the TD group required 24 months of robust hearing experience before every child reached the same criterion (Figure 2 and Table 5). Rapid progress was anticipated because the CI recipients were more mature than the TD children when they first began to hear. None-the-less, based on comparable amounts of robust hearing experience, the findings indicate that the more-rapid-than-typical speech development noted in previous milestone studies continued well in the 2nd year of CI-assisted hearing.
It is important to acknowledge that, in addition to relatively advanced maturity in cognitive, social, and motor development, participation in oral intervention programs also likely contributed to the rapid pace of vocal development in the CI children. Further, the use of hearing aids by several children, although not sufficient for achieving robust access to speech models might have contributed to children’s knowledge of some basic aspects of the speech signal such as fundamental frequency and durational cues. Thus, intervention, pre-CI hearing experiences, and children’s relatively advanced maturity at the time of implantation appear to have interacted to promote relatively rapid progress in speech development across the first 2 years of robust hearing experience.
It is interesting to note that a majority of the CI group’s utterances were classified as speech-like at every interval after 12 months of CI use. Further, the CI and TD children produced nearly identical percentages of speech-like utterances after 2 years of robust hearing (Figure 1). Considered together with the findings of earlier milestone studies, the results strongly suggest that an early period of auditory deprivation does not negatively affect progress in vocal development for deaf children who are implanted by 3 years of age and participate in oral intervention programs (Ertmer & Jung, 2012; Ertmer et al, 2007). The participant’s expeditious progress also reaffirms the value of early cochlear implantation for speech development (Connor, Craig, Raudenbush, Heavner, & Zwolan, 2006).
Taken together, our recent and current findings provide new expectations for examining the effects of CI use on early speech development. Specifically, oral, English-learning children without secondary disabilities can be expected to produce BCS and AF utterances at the 20% level by 6 and 12 months after device activation, respectively (Ertmer & Jung, 2012). As the young CI recipients in the current investigation showed, the percentages of these forms increased quickly and a clear shift toward dominance of speech-like utterances appeared between 12 and 18 months post-activation (Figure 2; and table 4). It is important to recognize that these expectations, although quite congruent with previously published longitudinal data, were based on a group of 12 children. Replication studies with larger samples are needed to establish these findings.
Work in our lab has also shown that vocal development is accompanied by sizable increases in phonological accuracy and expressive vocabulary during the first post-CI year (Ertmer & Inniger, 2009; Ertmer, Strong, & Sadagopan, 2003; Ertmer, Kloiber, Jung, Kirleis, & Bradford, 2012). Thus, implantation by 3 years of age leads to co-occurring advancements in early speech and semantic development. Examining progress in each of these areas can help to identify children who are making limited progress through the first-word stage. Re-evaluation and intervention modifications might then be initiated for children who show sizable delays. Such modifications could include CI re-mapping, communication modality changes, or increased amount of services, for example. Further studies of young CI recipients who use signs and speech together (i.e., simultaneous communication) and those who have multiple disabilities are needed to determine the time-course of vocal development in these groups.
Developmental trends for BCS and AF utterances
Utterances that were classified at the BCS and the AF levels showed different developmental trends across the first 2 years of robust hearing (See Figures 3 and 4). Accounting for approximately 30% of all utterances in young CI users at 6 months, BCS utterances showed only slight increases to approximately 40% at 15 months before decreasing to 30% again at 24 months. A similar trend was seen for the TD group as well: BCS utterances increased gradually from 5% at 6 months to slightly less that 40% at 18 months before decreasing to approximately 25%. Thus, the percentages of BCS utterances accounted for less than one third of all utterances at the 24 month interval in both groups. Recall that BCS utterances typically emerge around 5–10 months of age and include mainly CV and CVCV syllables and babbling (see Table 1; See Nathani et al, 2006; Oller, 2000; Vihman, 1996 for reviews). The comparatively early emergence of BCS utterances suggests that these first syllabic productions might have served as rudimentary approximations of adult speech models. That is, they might have been used to develop and integrate speech perception, neuro-motor coordination, and auditory feedback during a time when children are not yet able to replicate more complex syllable shapes, diphthongs, and prosodic patterns of adult speech. Then, as the link between auditory perception and speech production is strengthened, and speech-motor coordination is improved, BCS productions are increasingly replaced by the more complex and adult-like utterances of the AF level. In this way, BCS productions can be thought of as scaffolds for learning to produce the more diverse and complex syllable shapes found in adult’s connected speech models. In addition, the emergence of spoken words might also lead to syllable shape expansion as an increasing variety of word forms are recognized and attempted.
A different trajectory was seen for AF utterances, with both groups of children showing steady increases from 15 – 24 months (Figures 3 and 4). Recall that AFs begin to emerge around 10 months of age and continue to increase through the second year of life in TD children (Nathani et al. 2006). Compared to the BCS level, the AF level is characterized by variety of more complex syllable shapes (.e.g., VC, CVC, CCV), well-formed diphthongs, and jargon—multisyllabic utterances that integrate varied stress, intonation, and timing (see Table 1). Thus, AFs more closely resemble the syllable shape diversity of connected speech than those from the BCS level. The fact that AFs accounted for more than half of all utterances after 24 months of CI experience suggests that both groups of children had sufficient speech perception and production ability to closely approximate mature, connected speech patterns. Again, the emergence of spoken words and word combinations is also likely to lead to diversity in phonological forms. It is important to remember, however, that findings for AFs are influenced by the relatively frequent use of diphthongs and closed syllables in spoken English. Children who are acquiring languages that have fewer closed syllables or diphthongs (e.g., Japanese, French, Finnish and Italian) might show different trends for BCS and AF utterances.
Implications for the Infraphonological Model
Children’s shift to a majority of AF utterances reconfirms the existence of the fifth level of vocal development contained in the SAEVD-R: Advance Forms (Nathani et al, 2006). However, to fulfill the requirements of a developmental stage in the Infraphonological model, a newly mastered principle must also be identified. Clearly, AF utterances are canonical in nature (including isolated diphthongs because of their rapid formant transitions) and so the principle of rapid formant transition is not new to the AF level. What then, makes AF utterances different from the Basic Canonical Syllables level of the SAEVD-R and the Canonical level of the Infraphonological model?
Table 1 shows that the types of vocalizations found at the AF level are mainly characterized by two features beyond the mastery of rapid CV transitions: the production of syllables that require rapid VC transitions (closed syllables), and the introduction of prosody during syllable string production; as heard in jargon. Regarding the first feature, closed syllables (e,g., VC and CVC) require a rapid shift from vowel to consonant; an ability found to emerge later than well-formed CV productions and babbling (Nathani et a., 2006). By adding closed syllables to a repertoire that already includes CV-based syllables, children can produce a greater variety of syllable shapes, and syllable strings that more closely approximate adult connected speech models. However, the connected speech of adults is also characterized by changes in intonation, syllable duration, and loudness. These features can be heard as children produce jargon. Taken together then, there appear to be two newly mastered infraphonological principles at the AF level: rapid VC transitions and the ability to inject strings of diverse syllables with prosodic emphasis. Additional studies of vocal development are needed to examine the compatibility of these developmental trends and principles for children learning non-English languages.
Conclusions and Future Directions
This investigation has shown that young CI recipients continue to make relatively rapid advancements in vocal development through the second year of device use. On average, speech-like utterances reached the 60% majority status after 12 months and comprised more than 80% of samples taken after 24 months of CI experience. Majority status for speech-like utterances was achieved with fewer months of robust hearing experience than seen for the younger, TD group that first achieved a speech-like majority after 18 months of robust hearing. Taken together with findings from earlier studies of post-implantation vocal development milestones (Ertmer & Jung, 2012; McCaffery, Davis, MacNeilage, & von Hapsburg, 1999; Moore & Bass-Ringdahl, 2002; Schauwers et al. 2004) it is apparent that young, English-learning, CI recipients who are oral communicators and have no secondary disabilities can be expected to sustain accelerated progress in vocal development throughout the first 2 years of device use. The consistency of these findings strongly suggests that a relatively short period of auditory deprivation does not impose limitations or decelerate early auditory-guided speech development, and that implantation within a sensitive period for spoken language development promotes this process. Children’s more-rapid-than typical progress further supports the notion that young CI recipients are primed to integrate auditory perceptual and speech production abilities by their relatively advanced state of maturity when robust hearing is first introduced.
There is still much to be learned about the effects of cochlear implant experience on very young children’s speech development. At the prelinguistic level, questions remain about the nature of segmental acquisition and the rate at which phonetic inventories grow. Phonological questions naturally arise as children begin to say words on a regular basis. In particular, more information is needed to understand the relationship between speech perception and speech production, the syllable shapes of first words, segmental accuracy, and the intelligibility of speech after extended CI use. The ultimate goal of research in these areas is to determine whether the combination of early identification, cochlear implant technology, and specialized intervention enable deaf children to become proficient oral communicators. Through comparisons with children who have normal hearing, this work will also increase understanding of the processes that enable TD children to begin to talk like adults.
Acknowledgments
This research was funded by a grant to the first author from the National Institute on Deafness and Other Communication Disorders (R01DC007863). We are especially grateful to the parents and children who made this study possible. We are also indebted to the following individuals for their assistance in participant recruitment and data collection: Michele Wilkins, Wendy Ban Deters, Monica Brumbaugh Jennifer Haney, and Monica Lynch at Child’s Voice school (Wood Dale, IL); Jean Moog, Rhonda Bennight, Mariana Helbig, and Laurie Preusser at the Moog Center (Chesterfield, MO); Margo Appenzeller, Megan Mercurio, Carey Evans Ratliff, and Meredith Wessels at the Ohio Valley Voices (Loveland, OH); Mary Daniels, Cheryl Broekelmann, Kathy Gallagher, Barb Meyers, Judy Odendahl, and Audrea Strelo at the St. Joseph Institute for the Deaf (Chesterfield, MO); Teri Ouellette and Carrie Tamminga at the St. Joseph Institute for the Deaf (Indianapolis, IN). Jennifer Slanker, Christy Macak, Elesha Sharp, and Stephanie Wieczorek helped in data processing and utterance classification. Denise Bradford completed the statistical analyses in consultation with Bruce Craig. Thanks also to Kim Oller and Suneeti Nathani Iyer for their helpful feedback during the revision of this manuscript.
References
- Connor CM, Craig HK, Raudenbush SW, Heavner K, Zwolan TA. The age at which young deaf children receive cochlear implants and their vocabulary and speech-production growth: Is there an added value for early implantation? Ear and Hearing. 2006;27(6):628–644. doi: 10.1097/01.aud.0000240640.59205.42. [DOI] [PubMed] [Google Scholar]
- Eilers RE, Oller DK. Infant vocalizations and the early diagnosis of severe hearing impairment. Journal of Pediatrics. 1994;124:199–203. doi: 10.1016/S0022-3476(94)70303-5. [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Inniger KJ. Characteristics of the transition to spoken words in two young cochlear implant recipients. Journal of Speech, Language, and Hearing Research. 2009;52:1579–1594. doi: 10.1044/1092-4388(2009/06-0145). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ertmer DJ, Jung J. Prelinguistic vocal development in young cochlear implant recipients and typically developing infants: Year 1 of robust hearing experience. Journal of Deaf Studies and Deaf Education. 2012;17(1):116–132. doi: 10.1093/deafed/enr021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ertmer DJ, Kloiber DT, Jung J, Kirleis KC, Bradford D. Consonant production accuracy in young cochlear implant recipients: developmental sound classes and word position effects. American Journal of Speech-Language Pathology. 2012;21:342–353. doi: 10.1044/1058-0360(2012/11-0118). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Mellon JA. Beginning to talk at 20 months: Early vocal development in a young cochlear implant recipient. Journal of Speech, Language, and Hearing Research. 2001;44:192–206. doi: 10.1044/1092-4388(2001/017). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Nathani Iyer S. Prelinguistic vocalizations in infants and toddlers with hearing loss: Identifying and stimulating Auditory-guided Speech Development. In: Marschark M, Spencer P, editors. The Oxford University Handbook Deaf Studies, Language, and Education. Vol. 2. New York, New York: Oxford University Press; 2010. pp. 360–375. [Google Scholar]
- Ertmer DJ, Strong LM, Sadagopan N. Beginning to communicate after cochlear implantation: Oral language development in a young child. Speech, Language, and Hearing Research. 2003;46:328–340. doi: 10.1044/1092-4388(2009/06-0145). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Young NM, Nathani S. Profiles of vocal development in young cochlear implant recipients. Journal of Speech, Language, and Hearing Research. 2007;50:393–407. doi: 10.1044/0161-1461(2002/016). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fleiss JS. Statistical Methods for Rates and Proportions. New York, New York: Wiley; 1981. [Google Scholar]
- Iyer SN, Oller DK. Prelinguistic vocal development in typical hearing and infants with severe-to-profound hearing loss. Volta Review. 2008;108:115–138. [PMC free article] [PubMed] [Google Scholar]
- Koopmans-van Beinum FJ, van der Stelt JM. Early stages in the development of speech movements. In: Lindblom B, Zetterström R, editors. Proceedings of the Institute of Phonetic Sciences Amsterdam. Vol. 5. Amsterdam: University of Amsterdam; 1986. pp. 30–43. [Google Scholar]
- Lynch MP, Oller DK, Steffens M. Development of canonical vocalizations in a child with congenital absence of cochleas: The case of total deafness. Applied Psycholinguistics. 1989;10:315–333. doi: 10.1017/S0142716400008651. [DOI] [Google Scholar]
- Lynch MP, Oller DK, Steffens ML, Buder EH. Phrasing in Prelinguistic vocalizations. Developmental Psychology. 1995;28:3–25. doi: 10.1002/dev.420280103. [DOI] [PubMed] [Google Scholar]
- McCaffery HA, Davis BL, MacNeilage PF, von Hapsburg D. Multichannel cochlear implantation and the organization of early speech. Volta Review. 1999;101:5–28. [Google Scholar]
- Moeller MP, Hoover B, Putman C, Arbataitis K, Bohnenkamp G, Peterson B, et al. Vocalizations of infants with hearing loss compared with infants with normal hearing: Part I –Phonetic development. Ear & Hearing. 2007;28:605–627. doi: 10.1097/AUD.0b013e31812564ab. [DOI] [PubMed] [Google Scholar]
- Moore JA, Bass-Ringdahl S. Role of infant vocal development in candidacy for and efficacy of cochlear implantation. Annals of Otology, Rhinology, and Laryngology. 2002;111:52–55. doi: 10.1093/deafed/enq013. [DOI] [PubMed] [Google Scholar]
- Nathani S, Ertmer DJ, Stark RE. Assessing vocal development in infants and toddlers. Clinical Linguistics and Phonetics. 2006;20:351–369. doi: 10.1080/02699200500211451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nathani S, Oller DK, Neal AR. On the robustness of vocal development: an examination of infants with moderate-to-severe hearing loss and additional risk factors. Journal of Speech, Language, and Hearing Research. 2007;50:1425–44. doi: 10.1044/1092-4388(2007/099). [DOI] [PubMed] [Google Scholar]
- Nittrouer S. The relation between speech perception and phonemic awareness. Journal of Speech, Language, and Hearing Research. 1996;39:1059–1070. doi: 10.1044/jshr.3905.1059. [DOI] [PubMed] [Google Scholar]
- Nittrouer S, Burton LT. The role of early language experience in the development of speech perception and phonological processing abilities: Evidence from 5-year-olds with histories of otitis media with effusion and low socioeconomic status. Journal of Communication Disorders. 2005;38(1):29–63. doi: 10.1016/j.jcomdis.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Oller DK. The emergence of the sounds of speech in infancy. In: Yeni-Komshian G, Kavanaugh J, Ferguson C, editors. Child phonology. New York, New York: Academic Press; 1980. pp. 93–112. [Google Scholar]
- Oller DK. The emergence of the speech capacity. Mahwah, New Jersey: Lawrence Erlbaum Associates; 2000. [Google Scholar]
- Oller DK, Eilers R. The role of audition in infant babbling. Child Development. 1988;59:441–449. doi: 10.1111/1467-8624.ep8589370. [DOI] [PubMed] [Google Scholar]
- Oller DK, Eilers RE, Basinger D, Steffens ML, Urbano R. Extreme poverty and the development of precursors to the speech capacity. First Language. 1995;15:167–188. doi: 10.1177/014272379501504403. [DOI] [Google Scholar]
- Oller DK, Lynch MP. Infant vocalizations and innovations in infraphonology: Toward a broader theory of development and disorders. In: Ferguson CA, Menn L, Stoel-Gammon C, editors. Phonological Development. Models: Research, Implications. Timonium, MD: York Press; 1992. pp. 509–536. [Google Scholar]
- Roug l, Landburg I, Lundberg LJ. Phonetic development in early infancy: A study of four Swedish children during the first eighteen months of life. Journal of Child Language. 1989;16:19–40. doi: 10.1017/s0305000900013416. [DOI] [PubMed] [Google Scholar]
- Schauwers K, Gillis B, Daemers K, de Beukelaer C, Govaerts PJ. Cochlear implantation between 5 and 20 months of age: The onset of babbling and the audiologic outcome. Otology and Neurotology. 2004;25:263–270. doi: 10.1097/00129492-200405000-00011. [DOI] [PubMed] [Google Scholar]
- Stark RE. Stages of speech development in the first year of life. In: Yenikomshian G, Kavanaugh JF, Ferguson CA, editors. Child Phonology I: Production. New York: Academic Press; 1980. [Google Scholar]
- Stark RE. Phonatory development in young normally hearing and hearing-impaired children. In: Hochberg I, Levitt H, Osberger MJ, editors. Speech and hearing of the hearing-impaired: Research, training, and personnel preparation. Baltimore: University Park; 1983. [Google Scholar]
- Stoel-Gammon C, Otomo K. Babbling development of hearing-impaired and normally hearing subjects. Journal of Speech and Hearing Disorders. 1986;51:33–41. doi: 10.1044/jshd.5101.33. [DOI] [PubMed] [Google Scholar]
- Vihman MM. Variable paths to word production. Journal of Phonetics. 1993;21:61–82. [Google Scholar]
- Vihman MM. Phonological development: The origin of language in the child. Oxford, U.K: Blackwell; 1996. [Google Scholar]
- Vihman MM, Macken MA, Miller R, Simmons H, Miller J. From babbling to speech: A reassessment of the continuity issue. Language. 1985;61:395–443. doi: 10.2307/414151. [DOI] [Google Scholar]
- Zlatin M. Final report, Project No 3-4014, NE-G-00-3-0077. National Institutes of Health Research Grants; 1975. Preliminary descriptive model of infant vocalization during the first 24 weeks: Primitive syllabification and phonetic exploratory behavior. [Google Scholar]