

Abstract
Erdheim-Chester disease (ECD) is an uncommon non-Langerhans-cell histiocytosis, due to excessive production of histiocytes deposited in various organs and tissues in the human body. FDG PET was performed in a 68-year-old man with documented active ECD to evaluate the extent of the disease. The patient was previously treated with high dose subcutaneous Interferon alpha 2b, 1,000,000 units 3 times a week, but treatment was interrupted approximately 5 weeks prior to evaluation at NIH due to side effects of the medication. FDG PET/CT showed lesions were imaged in brain, heart, mediastinum and abdomen.
Keywords: PET/CT, FDG, Erdheim-Chester Disease, histiocytosis
FIGURE 1.
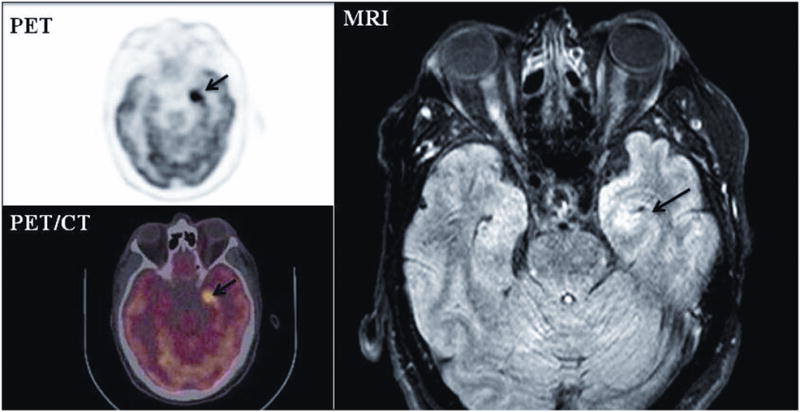
A 68-year-old male was admitted to the National Institutes of Health Clinical Center for evaluation on a NHGRI IRB approved natural history protocol of Erdheim-Chester disease (ECD). Transaxial images of PET, fused PET/CT and MRI showed a hypermetabolic focus in the left medial temporal lobe with a bodyweight SUVmax of 14.8, (arrow), and a lesion in the left putamen (SUVmax of 10.7) (not shown). Intracranial lesions imaged by MRI and CT are usually multifocal and can involve brain, meninges, perivascular, and other areas.1
FIGURE 2.
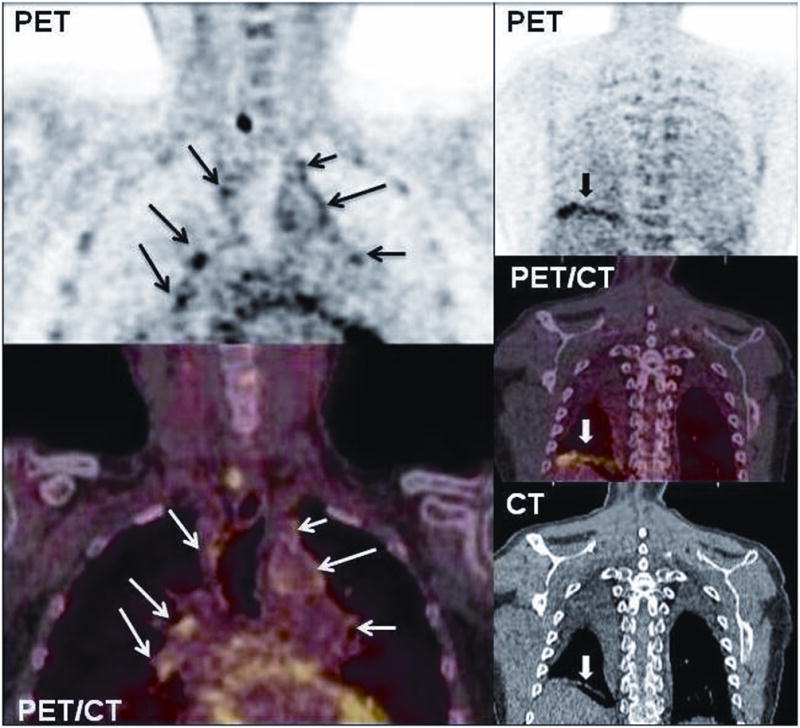
Coronal chest images of PET and fused PET/CT show several abnormal areas in the mediastinum and hila (arrows) and right posterior lower lung (fat arrow). The right perihilar lesion had an SUVmax of 6.1.
FIGURE 3.
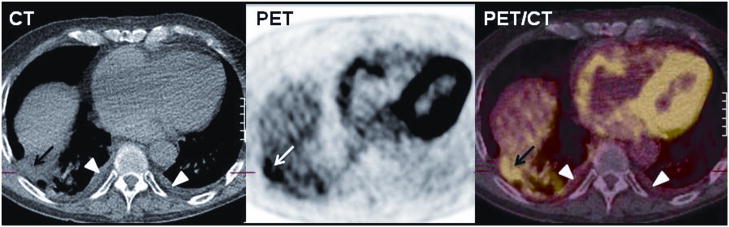
Transaxial images of PET and fused PET/CT show increased FDG uptake in the right posterior lung (SUVmax of 5) corresponded to an area of old granulomatous disease as described in CT (arrow). Chest CT demonstrated also a small bilateral pleural effusion as seen also in PET/CT with no FDG uptake (arrowheads). Patients with ECD may have lung involvement, manifested as interstitial lung disease and pulmonary fibrosis and pleural involvement and infiltration.2,3
FIGURE 4.

Transaxial images of PET (A), fused PET/CT (B), and MRI (C) showed increased FDG uptake in right atrial wall mass (arrows). When ECD is associated with cardiovascular involvement, the prognosis is worse due to fatal complications from heart failure, tamponade, myocardial infarction, abdominal aortic stenosis and periaortic or perirenal artery fibrosis [4].
FIGURE 5.
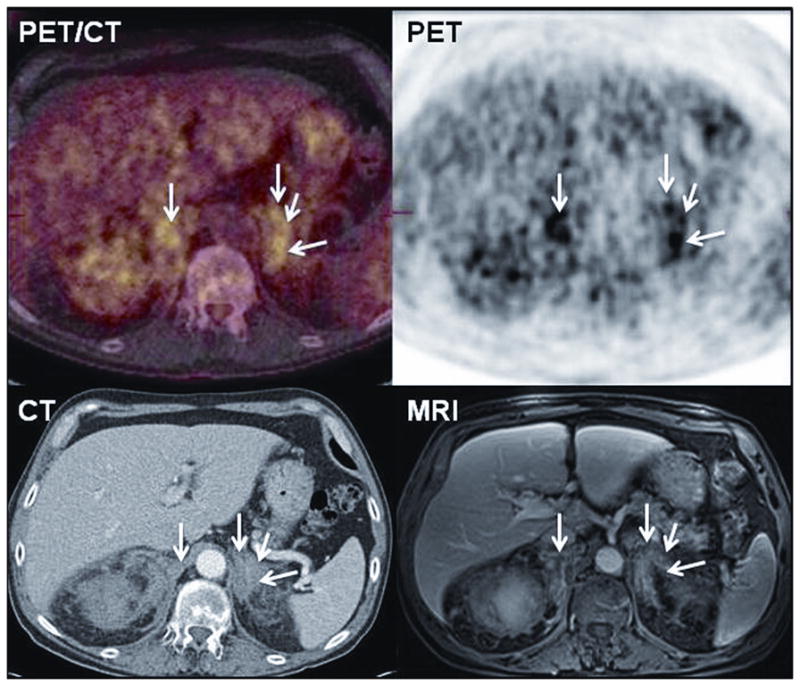
In the abdomen PET (C), CT (B) and fused PET/CT (A), transverse images showed multiple areas of FDG uptake in the suprarenal adrenal areas (SUVmax up to 8.1) (arrows). MRI showed enlarged, shaggy adrenals consistent with fibrosis encasing the adrenals similar to previous reports [5].
FIGURE 6.

Bilateral enlarged kidneys on PET (A) image. Retroperitoneal fibrosis with perirenal (arrows) and periaortic (not shown) involvement was reported by MRI (B). CT showed extensive retroperitoneal soft tissue thickening surrounding the kidneys (arrows). CT studies in patients with ECD may show enlarged kidneys, renal infiltration, sometimes leading to ureteral stenosis [6, 7].
FIGURE 7.
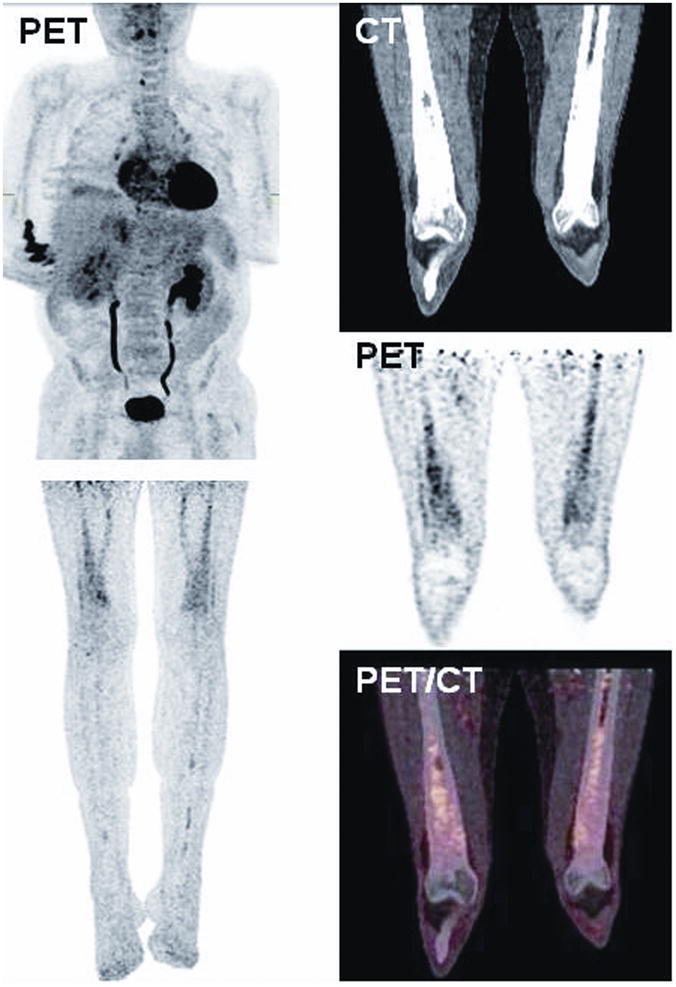

A, PET/CT images show diffuse FDG uptake in long bones (humeri, femurs, and tibias).
FIGURE 7B. X-rays showed sclerotic lesions with some cystic changes in both femoral necks. Minimal periosteal thickening with diaphyseal marrow sclerosis was noted in the distal femurs by x-rays, the proximal and distal tibias and both fibulas, the proximal humeri and distal right radius and ulna.
FIGURE 8.
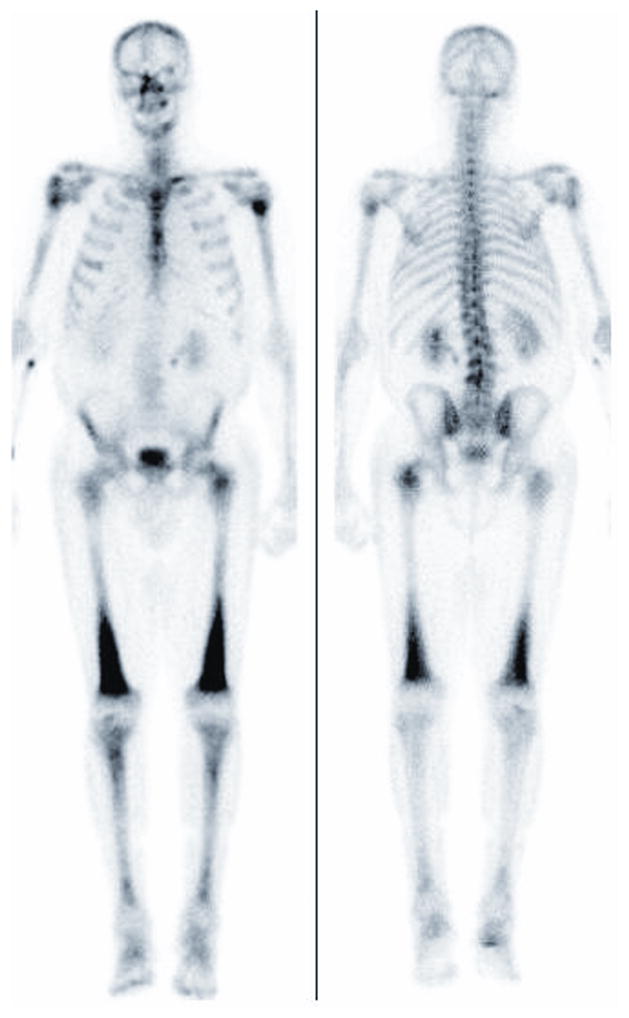
The MDP bone scan shows intense radiotracer activity in bilateral extremities such as the femurs, humeri and tibias. The existence of bilateral osteosclerotic bone involvement has been reported in the diaphysis 98%, 8 and skull and facial bone lesions in 80% of patients.1
FIGURE 9.
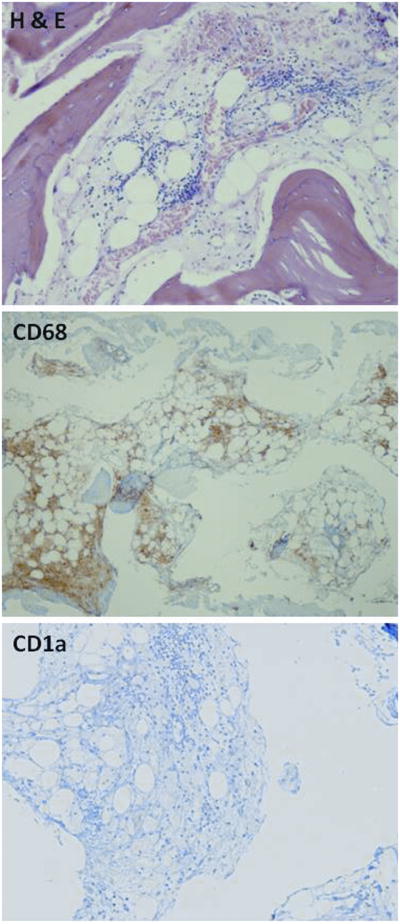
Bone marrow biopsy typically shows positive CD68, CD4, and CD163, and negative to CD1a histiocytes [4]. H & E staining of bone marrow revealed hypocellular bone marrow with focal fat atrophy and presence of foamy histiocytes with granular eosinophilic cytoplasm. Immunohistochemistry showed positive CD68 staining and negative CD1a staining.
References
- 1.Drier A, Haroche J, Savatovsky J, et al. Cerebral, facial, and orbital involvement in Erdheim-Chester disease: CT and MR imaging findings. Radiology. 2010;255:586–594. doi: 10.1148/radiol.10090320. [DOI] [PubMed] [Google Scholar]
- 2.Brun AL, Touitou-Gottenberg D, Haroche J, et al. Erdheim-Chester disease: CT findings of thoracic involvement. Eur Radiol. 2010;20:2579–2587. doi: 10.1007/s00330-010-1830-7. [DOI] [PubMed] [Google Scholar]
- 3.Shamburek RD, Brewer HB, Jr, Gochuico BR. Erdheim-Chester disease: a rare multisystem histiocytic disorder associated with interstitial lung disease. Am J Med Sci. 2001;321:66–75. doi: 10.1097/00000441-200101000-00010. [DOI] [PubMed] [Google Scholar]
- 4.Haroche J, Amoura Z, Dion E, et al. Cardiovascular involvement, an overlooked feature of Erdheim-Chester disease: report of 6 new cases and a literature review. Medicine (Baltimore) 2004;83:371–392. doi: 10.1097/01.md.0000145368.17934.91. [DOI] [PubMed] [Google Scholar]
- 5.Haroche J, Amoura Z, Touraine P, et al. Bilateral adrenal infiltration in Erdheim-Chester disease. Report of seven cases and literature review. J Clin Endocrinol Metab. 2007;92:2007–2012. doi: 10.1210/jc.2006-2018. [DOI] [PubMed] [Google Scholar]
- 6.Andre M, Delevaux I, de Fraissinette B, et al. Two enlarged kidneys: a manifestation of Erdheim-Chester disease. Am J Nephrol. 2001;21:315–317. doi: 10.1159/000046267. [DOI] [PubMed] [Google Scholar]
- 7.Dundee P, Bouchier-Hayes D, Iles L, et al. Renal calculi in a patient with Erdheim-Chester disease. Int Urol Nephrol. 2005;37:453–456. doi: 10.1007/s11255-004-0020-4. [DOI] [PubMed] [Google Scholar]
- 8.Dion E, Graef C, Miquel A, et al. Bone involvement in Erdheim-Chester disease: imaging findings including periostitis and partial epiphyseal involvement. Radiology. 2006;238:632–639. doi: 10.1148/radiol.2382041525. [DOI] [PubMed] [Google Scholar]