

Abstract
Xanthomatous meningioma is an extremely rare variant of meningioma that is characterized histopathologically by the presence of tumor cells with lipid-filled vacuolated cytoplasm. In this report, we describe the fifth documented case of xanthomatous meningioma and review its clinicopathological features. A 76-year-old Japanese male presented with dizziness. Magnetic resonance imaging demonstrated a well-circumscribed tumor in the left parasagittal to frontal region with attachment of the dura mater. Histopathological examination of the resected specimen revealed proliferation of polygonal to spindle cells with eosinophilic cytoplasm and bland round to oval nuclei. Whorl formation and psammomas were scattered, and mitotic figures were rarely seen. A peculiar finding was the presence of extensive xanthomatous change continuing to the above-mentioned typical meningothelial meningioma. These tumor cells had clear vacuolated cytoplasm and bland round to oval nuclei. Immunohistochemically, xanthomatous cells were positive for epithelial membrane antigen. Accordingly, an ultimate diagnosis of xanthomatous meningioma was made. Our clinicopathological analysis revealed that xanthomatous meningioma affects children to young persons or the elderly, and four of five cases were located in the supratentorial region. Although the detailed mechanism underlying the xanthomatous change has not been clarified, this change is thought to result from a metabolic abnormality of the neoplastic meningothelial cells. Further, xanthomatous change has also been reported in atypical and anaplastic meningiomas. Therefore, it is important to recognize that xanthomatous change can occur in meningiomas, and to avoid misidentifying these cells as macrophages.
Keywords: Meningioma, metaplastic, xanthomatous, adipophilin
Introduction
Meningioma is a neoplasm derived from meningothelial cells that shows various histopathological features. A recent World Health Organization Classification divides grade I meningioma into 9 subtypes: meningothelial, fibrous, transitional, psammomatous, angiomatous, microcystic, secretory, lymphoplasmacyte-rich, and metaplastic [1]. Metaplastic meningioma is one of the rarest subtypes, and is defined as a tumor containing striking focal or widespread mesenchymal components including osseous, cartilaginous, lipomatous, myxoid, or xanthomatous tissue, singly or in combinations [1]. Xanthomatous change is characterized histopathologically by the presence of a significant number of tumor cells with vacuolated lipid-filled cytoplasm. Metaplastic meningioma with extensive xanthomatous change, namely “xanthomatous” meningioma, has been extremely rarely reported [2-5]. Herein, we report the fifth documented case of xanthomatous meningioma and review its clinicopathological features.
Case report
A 76-year-old Japanese male presented with dizziness at an outpatient clinic. Magnetic resonance imaging demonstrated a well-circumscribed tumor in the left parasagittal to frontal region with attachment to the dura mater (Figure 1). He was referred to our hospital for operation of the tumor, and subsequently a total resection of the tumor was performed under a clinical diagnosis of meningioma.
Figure 1.
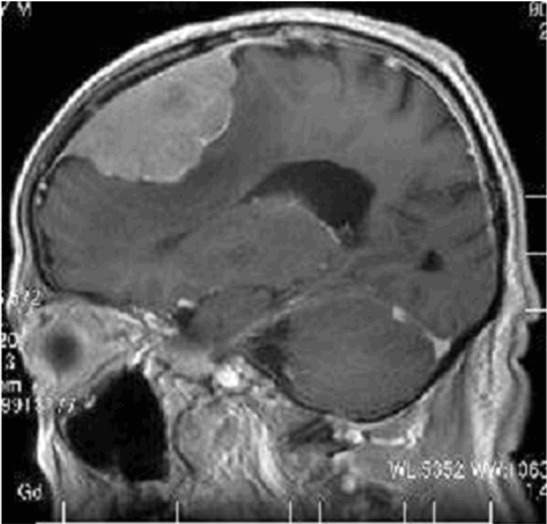
Magnetic resonance imaging showing a well-circumscribed tumor with attachment to the dura mater in the parasagittal to frontal region.
Histopathological examination of the resected tumor revealed proliferation of polygonal to spindle cells with eosinophilic cytoplasm and bland round to oval nuclei containing small nucleoli (Figure 2A-C). Whorl formation and psammomas were scattered (Figure 2A, 2C). Mitotic figures were rarely seen (0-1/10 high-power fields). No geographic necrosis was present. A peculiar finding was the presence of extensive xanthomatous change within the tumor that comprised approximately 50% of the tumor, continuing to the above-mentioned typical meningothelial meningioma. The tumor cells had clear vacuolated cytoplasm and centrally located bland round to oval nuclei (Figure 2A-C). No mitotic figures were found in the xanthomatous area. A transition between the conventional meningioma and the xanthomatous area was present (Figure 2A, 2C). Moreover, infiltration of foamy macrophages and small lymphocytes was observed focally. Neither mature adipocytes nor osteocartilaginous tissue was present within the tumor. No invasion into the brain parenchyma or bone was noted.
Figure 2.

Histopathological features. A: The tumor comprises two components. The conventional meningioma component (upper right) is composed of polygonal cells with eosinophilic cytoplasm and bland round to oval nuclei. The xanthomatous component (lower left) comprises vacuolated clear cytoplasm with bland round nuclei. HE, x 200. B: Xanthomatous component. The tumor cells have rich clear vacuolated cytoplasm. HE, x 400. C: A transition between the conventional meningioma and the xanthomatous area is present. Psammomas are present. HE, x 100.
Immunohistochemical studies were performed using an autostainer (Ventana) by the same method as previously reported [6-9]. Epithelial membrane antigen (EMA) was expressed in both the conventional meningioma and the xanthomatous component (Figure 2A). Vimentin was also expressed in both components. CD68, MAC387, and lysozyme were expressed only in the xanthomatous component. Interestingly, adipophilin was expressed in the xanthomatous component as well as in the conventional meningioma (Figure 3B). The average Ki-67 labeling index was 2.1%, and there were a few areas of 4-5% within the tumor.
Figure 3.
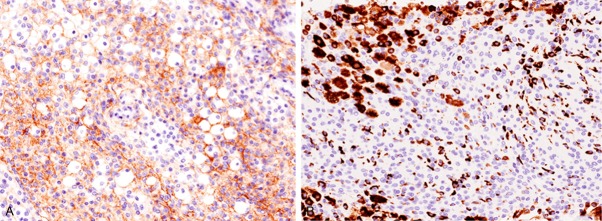
Immunohistochemical features. A: Epithelial membrane antigen is expressed in the xanthomatous area, x 200. B: Adipophilin is expressed in the xanthomatous area as well as in the conventional meningioma, x 200.
According to these findings, an ultimate diagnosis of xanthomatous meningioma was made.
Discussion
The term “xanthomatous” meningioma was first coined by Kepes in 1994 [2]. Since then, only three additional cases with detailed histopathological and immunohistochemical features have been reported and we describe here the fifth documented case of xanthomatous meningioma. Table 1 summarizes the clinicopathological features of the four previously reported cases of xanthomatous meningioma as well as the present one. The distribution of the patients is interesting. This type of tumor affects children to young persons or the elderly (Table 1). Four of five cases were located in the supratentorial region, and one case was located in the posterior cranial fossa [3]. Ijiri et al. reported a case of radiation-associated xanthomatous meningioma in 10-year-old child, who had been treated for ependymoma at the age of 2 years following radiation therapy (total 55.5 Gy) [4].
Table 1.
Clinicopathological features of xanthomatous meningioma
| Case No. | Age/Gender | Location | Transition between conventional meningioma and xanthomatous area | Immuohistochemistry | Reference |
|---|---|---|---|---|---|
| 1 | 24/Male | Right parietal | + | CD68 (+) | [2] |
| 2 | 2/Female | Posterior pyramid | Not available | EMA (+) | [3] |
| 3 | 10/Male | Right frontal | + | CD68 (+) | [4] |
| 4 | 61/Female | Right occipital to parietal | + | EMA (+), CD68 (+), Ki-67 LI 2.2% | [5] |
| Present case | 76/Male | Left parasagittal to frontal | + | EMA (+), CD68 (+), adipophilin (+), Ki-67 LI 2.1% |
EMA, epithelial membrane antigen; Ki-67 LI, Ki-67 labeling index.
The histopathological hallmark of xanthomatous meningioma is the presence of xanthomatous tumor cells [2-5]. These xanthomatous cells have been considered as neoplastic meningothelial cells, not macrophages because these cells were positive for EMA, as also seen in the present case although macrophage markers, such as CD68 and lysozyme, also were expressed [2-5].
This report is the first to examine the immunohistochemical analysis of adipophilin in xanthomatous meningioma. Adipophilin is an antibody that recognizes protein associated with lipid droplets, and is used as a useful immunohistochemical marker [10]. Interestingly, adipophilin was expressed in the xanthomatous area as well as in the conventional meningothelial meningioma component of the present case. This suggests that the conventional meningothelial meningioma component may have lipid droplet within the cytoplasm although xanthomatous differentiation was not observed by light microscopic examination.
Lipomatous meningioma is also a rare histopathological subtype of meningioma that is characterized by the presence of adipocytes [12]. Roncaroli et al. reported the clinicopathological features of 18 cases of this type of tumor [11]. In their series, 6 cases had xanthomatous meningothelial cells admixed with adipocyte-like cells, and a transition between the two components was evident in some cases [11]. Lipid deposition was observed in both of the two components, and these changes may appear to result from a metabolic abnormality of the neoplastic meningothelial cells, although the detailed mechanism underlying xanthomatous change has not been clarified [11]. Further, as mentioned above, conventional meningothelial meningioma cells showed a positive immunoreactivity for adipophilin, therefore, a metabolic abnormality may occur in these cells, resulting in the obvious xanthomatous change.
Albeit extremely rare, the xanthomatous change has also been observed in atypical and anaplastic meningiomas [12]. Taraszewska et al. reported three cases of atypical meningioma and two cases of anaplastic meningioma with xanthomatous changes [12]. The xanthomatous change was extensive in all three atypical meningiomas and focal in the two anaplastic meningiomas [12]. This change can occur in atypical and anaplastic meningiomas as well as grade I meningioma.
In conclusion, we have described a case of xanthomatous meningioma. Xanthomatous change may be caused by a metabolic change in the neoplastic meningothelial cells, and this change can occur in atypical and anaplastic meningiomas. It is important for pathologists to recognize that xanthomatous change can occur in meningiomas, and not to misidentify these cells as macrophages.
References
- 1.Perry A, Louis DN, Scheithauer BW, Budka H, von Deimling A. Meningiomas. In: Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, editors. World Health Organization Classification of Tumours of the Central Nervous System. Lyon: IARC Press; 2007. pp. 164–172. [Google Scholar]
- 2.Kepes JJ. Lipidized meningothelial tumor cells in “zanthomatous” meningioma express macrophage antigen. J Neuropathol Exp Neurol. 1994;53:384–388. doi: 10.1097/00005072-199407000-00010. [DOI] [PubMed] [Google Scholar]
- 3.Germano A, Galatioto S, La Rosa G, Caffo M, Cardia E. Xanthomatous posterior pyramid meningioma in a 2-year-old girl. Childs Nerv Syst. 1997;13:406–411. doi: 10.1007/s003810050109. [DOI] [PubMed] [Google Scholar]
- 4.Ijiri R, Tanaka Y, Hara M, Sekido K. Radiation-associated xanthomatous meningioma in a child. Childs Nerv Syst. 2000;16:304–308. doi: 10.1007/s003810050519. [DOI] [PubMed] [Google Scholar]
- 5.Ikota H, Nakazato Y. A case of metaplastic meningioma with extensive xanthomatous change. Neuropathology. 2008;28:422–426. doi: 10.1111/j.1440-1789.2008.00865.x. [DOI] [PubMed] [Google Scholar]
- 6.Ishida M, Iwai M, Yoshida K, Kagotani A, Okabe H. Sarcomatoid carcinoma with small cell carcinoma component of the urinary bladder: A case report with review of the literature. Int J Clin Exp Pathol. 2013;6:1671–1676. [PMC free article] [PubMed] [Google Scholar]
- 7.Ishida M, Mori T, Umeda T, Kawai Y, Kubota Y, Abe H, Iwai M, Yoshida K, Kagotani A, Tani T, Okabe H. Pleomorphic lobular carcinoma in a male breast: case report with review of the literature. Int J Clin Exp Pathol. 2013;6:1441–1444. [PMC free article] [PubMed] [Google Scholar]
- 8.Nakanishi R, Ishida M, Hodohara K, Yoshida T, Yoshii M, Okuno H, Horinouchi A, Iwai M, Yoshida K, Kagotani A, Okabe H. Prominent gelatinous bone marrow transformation presenting prior to myelodysplastic syndrome: a case report with review of the literature. Int J Clin Exp Pathol. 2013;6:1677–1682. [PMC free article] [PubMed] [Google Scholar]
- 9.Ishida M, Mochizuki Y, Iwai M, Yoshida K, Kagotani A, Okabe H. Pigmented squamous intraepithelial neoplasia of the esophagus. Int J Clin Exp Pathol. 2013;6:1890–1893. [Google Scholar]
- 10.Ishida M, Okabe H. Sebaceous carcinoma with apocrine differentiation (seboapocrine carcinoma) Pathol Int. 2012;62:438–440. doi: 10.1111/j.1440-1827.2012.02820.x. [DOI] [PubMed] [Google Scholar]
- 11.Roncaroli F, Scheithauer BW, Laeng RH, Cenacchi G, Abell-Aleff P, Moschopulos M. Lipomatous meningioma. A clinicopathologic study of 18 cases with special reference to the issue of metaplasia. Am J Surg Pathol. 2001;25:769–775. doi: 10.1097/00000478-200106000-00008. [DOI] [PubMed] [Google Scholar]
- 12.Taraszewska A, Matyja E, Bogucki J. Xanthomatous changes in atypical and anaplastic maningiomas. Light and electron microscopic investigations. Folia Neuropathol. 2000;38:125–134. [PubMed] [Google Scholar]