

Abstract
Background:
Total knee arthroplasty (TKA) and total hip arthroplasty (THA) are the most widely practiced surgical options for arthritis all over the world and its application is rising in India. Indian Society of Hip and Knee Surgeons (ISHKS) has established a joints registry and has been collecting data for last 6 years.
Materials & Methods:
All members of ISHKS are encouraged to actively participate in the registry. A simple two page knee and hip form can be downloaded from the website www.ishks.com. The information collected includes patient demographics, indication for surgery, implant details and in case of revision arthroplasty: the details of implants removed and the cause of failure of primary arthroplasty. These forms are mailed to the central registry office and the data is fed in computerized registry. Data collection started in October 2006.
Results:
Joint registry is a very important initiative of ISHKS and till date, have data of 34,478 TKAs and 3604 THAs, contributed by 42 surgeons across India. Some important observations have emerged. Data of 34,478 TKAs was assessed: These included 8612 males (25%) and 25,866 females (75%). Average age was 64.4 years (Osteoarthritis range: 45 to 88 years; Rheumatoid arthritis range: 22 to 74 years). Average body mass index was 29.1 (Range: 18.1 to 42.9). The indication for TKA was osteoarthritis in 33,444 (97%) and rheumatoid arthritis in 759 (2.2%). Total of 3604 THA procedures were recorded. These included 2162 (60%) male patients and 1442 (40%) female patients. Average age was 52 years (Range 17 to 85 years) and average BMI was 25.8 (Range: 17.3 to 38.5). The indications for THA was AVN in 49%.
Conclusion:
The registry will become more meaningful in years to come. Active participation of all arthroplasty surgeons across India is vital for the success of the joints registry.
Keywords: Indian Society of Hip and Knee Surgeons, joints, registry, total hip arthroplasty, total knee arthroplasty
INTRODUCTION
Joint replacement (arthroplasty) as a surgical option for end stage arthritis is well established now and millions of patients across the world have benefited. India is a country of 1.2 billion people with significant knee and hip arthritis population. According to Frost and Sullivan research, the arthroplasty market is expected to grow at a compound annual growth rate of 26.7% during 2010-2017.1 According to this survey, almost 70,000 joint replacement surgeries were performed in India in the year 2011.1 The demand for joint replacement surgery is set to rise further; therefore, the urgent need for training of surgeons as well as monitoring the implant usage.
Indian society of hip and knee surgeons (ISHKS) was established in 2005 with several goals. Three important ones are arthritis research, surgeon training and setting up a joints registry. It is a registered Charitable Trust, with 26 arthroplasty surgeons across India as founder members.
Need for joints registry
Orthopedic joints implants such as used for total knee arthroplasty (TKA) and total hip arthroplasty (THA) are normally expected to last for more than a decade based on clinical studies.2,3 New implants continue to be introduced with the hope that they are better than previous ones, but not all new prosthesis are better. In fact, some joint replacement implants that were thought to be the latest and better have turned out to be failures and even recalled.4,5,6,7,8 History of arthroplasty implants shows that many devices such as threaded acetabular shells, metal backed patellar components, first generation ceramic heads and titanium bearing surfaces all failed early. Recent examples include early failure of Sulzer acetabular cup and 3 M capital hip implant and ASR (Articular Surface Replacement, DePuy, USA) hip resurfacing system.4,5,6,7,8 The clinical impact of failures such as these could be minimized with prompt reporting and ongoing data collection through registry. The worrying part is not that there have been failures, but how long they have taken to be detected. Failure of any such implants needs to be established early to reduce patient morbidity and mortality from their continued usage. Past experience of early failure of some devices has shown that early warning is necessary to reduce the social and economic impact of such early failures. The registry is very important as a watchdog to register and monitor all the arthroplasty implants and assesses the long term outcome. Registry data is completely confidential and no personal information about patients or surgeons is accessible to any commercial entity.
Several countries have already established the arthroplasty registry, Swedish National Arthroplasty registry being one of the oldest and most reputed one.9,10 Other countries that already have registry include Finland, Norway, Denmark, Australia, Hungary, New Zealand, Scotland, Canada, England/Wales, Romania, USA, South Africa and Malawi.11,12,13,14,15,16,17,18 All registries except England and Wales have been managed by Orthopaedic surgeons and without any government control.
As with all registries world over, active participation from arthroplasty surgeons is very important. Such participation is entirely voluntary and therefore compliance is a significant issue. Currently, ISHKS has 42 members who contribute to the registry on a regular basis.
MATERIALS AND METHODS
All members of ISHKS are encouraged to actively participate in the registry. A simple two page knee and hip form can be downloaded from the website www.ishks.com. Each surgeon is given a code to maintain the confidentiality of the data. The information collected includes patient demographics, indication for surgery, implant details and in case of revision arthroplasty: the details of implants removed and the cause of failure of primary arthroplasty. These forms are mailed to the central registry office and the data is fed in computerized registry.
RESULTS
Data collection started in October 2006 and until April 2012, information was collected on 34478 TKAs and 3604 THAs [Figure 1].
Figure 1.
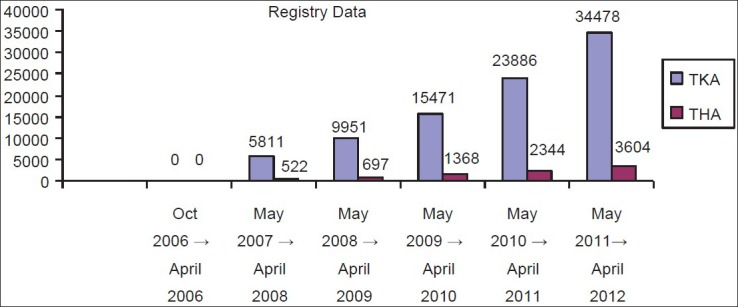
A bardiagram showing registry data of TKA and THA
Total Knee Arthroplasty
Data of 34,478 TKAs was assessed: These included 8612 males (25%) and 25,866 females (75%). Average age was 64.4 years (Osteoarthritis range: 45 to 88 years; Rheumatoid arthritis range: 22 to 74 years). Average body mass index was 29.1 (Range: 18.1 to 42.9). The indication for TKA was osteoarthritis in 33,444 (97%) and rheumatoid arthritis in 759 (2.2%).
The market share of various companies in India for TKA prosthesis is shown in Figure 2.
Figure 2.
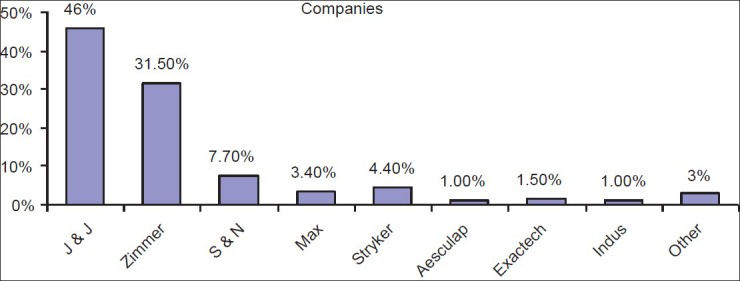
A bar diagram showing market share of various companies (TKA)
Primary TKA implant type
74% of primary TKA implants used are posterior stabilized fixed bearing with only 11% cruciate retaining implants used. Remaining 15% were rotating platform, constrained knees (e.g. LCCK, RHK from Zimmer and TC 3, Noiles Hinge from DePuy J and J).
Patellar resurfacing
With one company implant, 81% TKAs had patellar resurfacing. In stark contrast, with another make of implant, only 20% patellae were resurfaced.
Revision Total Knee Arthroplasty
Total of 281 procedures were recorded [Figure 3]. The indication for surgery was as follows:
Figure 3.
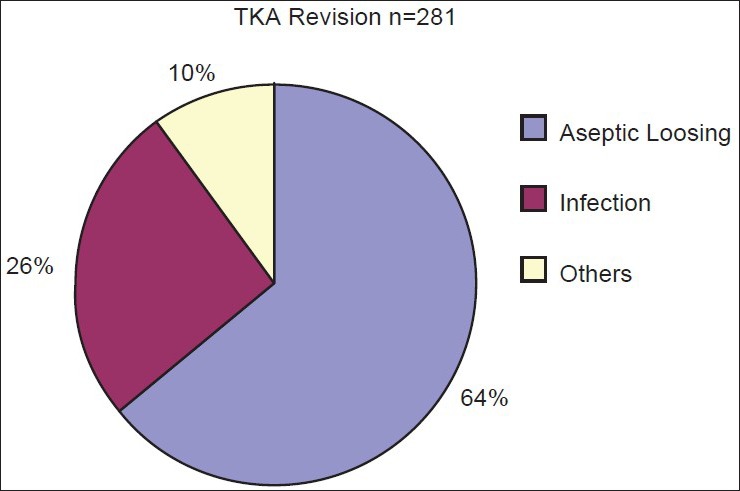
Pie chart showing TKA revision
Aseptic loosing = 64%
Infection = 26%
Others = 10%.
Total Hip Arthroplasty
Total of 3604 THA procedures were recorded. These included 2162 (60%) male patients and 1442 (40%) female patients. Average age was 52 years (Range 17 to 85 years) and average BMI was 25.8 (Range: 17.3 to 38.5). The indications for THA are shown in Figure 4.
Figure 4.
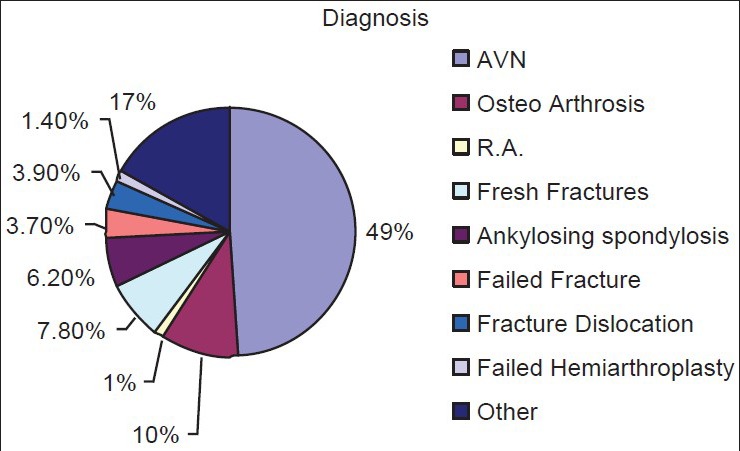
Pie chart showing indications of THA
Market share of various companies for THA is shown in Figure 5. The types of prosthesis used are shown in Figure 6. Total of 261 Revision THA procedures were recorded. The indications for surgery are shown in Figure 7.
Figure 5.
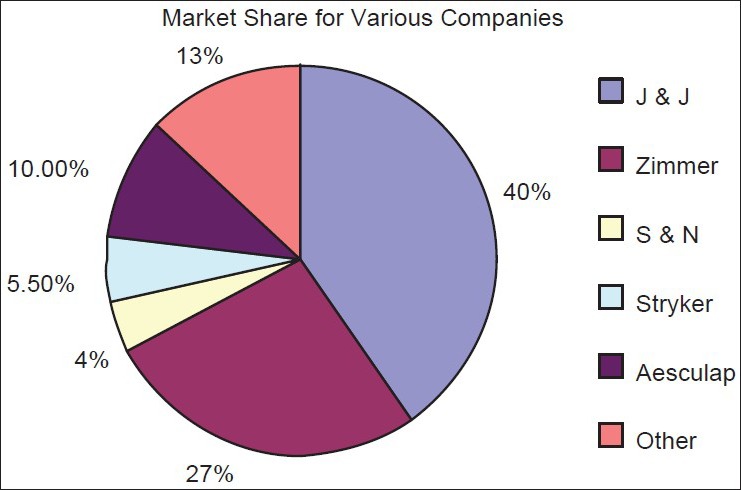
Pie chart showing market share of various companies of THA
Figure 6.
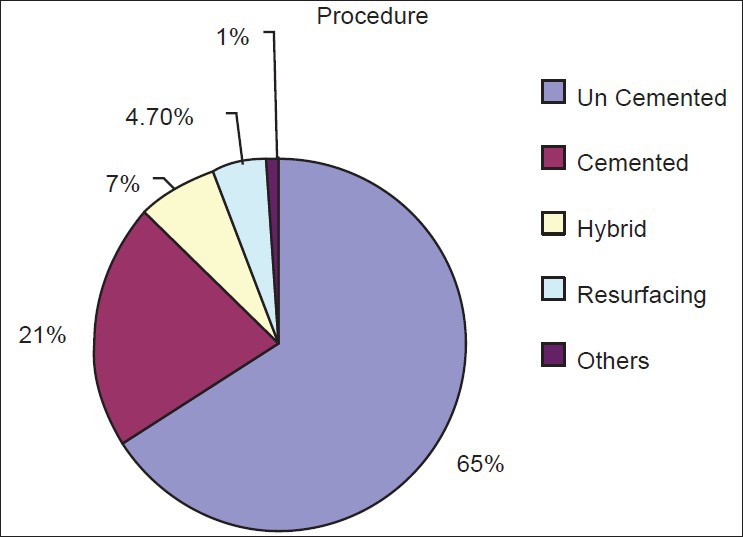
Pie chart showing types of prosthesis used in THA
Figure 7.
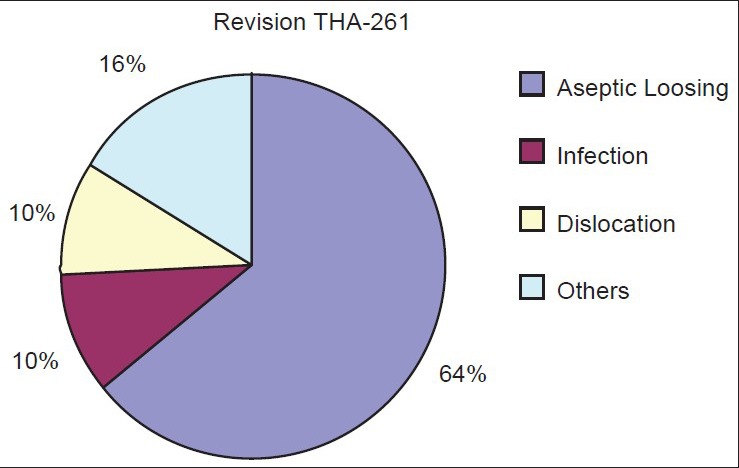
Pie chart showing indications of revision THA
DISCUSSION
Registry participation is entirely voluntary on the part of arthroplasty surgeons and thereby presents a problem. For the registry to provide meaningful and validated information, it should have at least 90% surgeon's participation. Apathy, lack of trust, fear of information disclosure are some of the reasons for nonparticipation by surgeons. In England and Wales, registry participation is likely to be very high as it is governed by department of health. Even in USA, where registry participation is voluntary, surgeon's participation is a problem. Education and assurance about concerns, is the key to improved participation.
The advantages and disadvantages of a government-run registry compared with an independently run registry are currently being debated.18 Registries in Sweden, Great Britain, Australia and Canada that collect outcome data through their national health care programs have all documented the early detection of joint replacement problems that led to timely interventions, preventing harm to additional patients and reducing arthroplasty revisions by as much as 10%.19,20,21
In India, arthroplasty numbers are set to go up significantly and therefore is an ideal time to set up a national joints registry. ISHKS has taken this initiative and has set up a base in Ahmedabad. All arthroplasty surgeons are requested to join this nationwide initiative, the fruits of which will be apparent in the years to come.
In the short time that the registry has been in place, some important facts have emerged: The incidence of rheumatoid arthritis as the indication for TKA is very low (2.2%). The prevalence of cemented TKA is absolute with no cases using uncemented total knee prosthesis. The use of posterior stabilized prosthesis is predominant (74%) with only 11% of cases are done using cruciate retaining prosthesis. The BMI of patients undergoing TKA is higher than those undergoing THA (29.1 vs. 25.8) indicating an entirely different patient population. The avascular necrosis of the hip is the indication for total hip replacement is 49% patients, with primary osteoarthritis in only 10% patients. This is a completely different disease demography compared with Caucasian population where primary osteoarthritis of the hip is predominant. It also reveals the preponderance of hip avascular necrosis, the etiology of which is likely to be widespread steroid and alcohol abuse. The uncemented hip prosthesis use is much higher (65%) than the cemented prosthesis. The incidence for revision of total knee arthroplasty for infection is much higher than revision for infected total hip replacement. This could suggest that many cases of infected hip arthroplasty must be left as Girdlestone arthroplasty.
If all arthroplasty procedures across the country are registered in the registry, it will be ideal. However, it is an enormous task in a country like India. Industry participation and perhaps government legislation are some of the avenues that can be considered to improve the surgeon participation.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1. [Last accessed on 2013 June 9]. Available from: http://www.researchandmarkets.com/reports/1877536/overview_of_orthopedic_joint_replacement_market.pdf .
- 2.Rodriguez JA, Bhende H, Ranawat CS. Total condylar knee replacement: A 20-year followup study. Clin Orthop Relat Res. 2001;388:10–7. [PubMed] [Google Scholar]
- 3.Callaghan JJ, Albright JC, Goetz DD, Olejniczak JP, Johnston RC. Charnley total hip arthroplasty with cement. Minimum twenty-five-year followup. J Bone Joint Surg Am. 2000;82:487–97. doi: 10.2106/00004623-200004000-00004. [DOI] [PubMed] [Google Scholar]
- 4. [Last accessed on 2013, September 6]. Available from: http://www.biomed.brown.edu/Courses/BI108/BI108_2007_Groups/group 05/pages/sulzer.html .
- 5. [Last accessed on 2013 June 9]. Available from: http://www.rcseng.ac.uk/surgeons/research/surgical-research/docs/An%20Investigation%20of%20the%20Performance%20of%20the%203M%20Capital%20Hip%20System%20Report%202001.pdf .
- 6.Bernthal NM, Celestre PC, Stavrakis AI, Ludington JC, Oakes DA. Disappointing short-term results with the DePuy ASR XL metal-on-metal total hip arthroplasty. J Arthroplasty. 2012;27:539–44. doi: 10.1016/j.arth.2011.08.022. [DOI] [PubMed] [Google Scholar]
- 7. [Last accessed on 2013 June 9]. Available from: http://www.asrrecall.depuy.com/countries_list .
- 8.de Steiger RN, Hang JR, Miller LN, Graves SE, Davidson DC. Five-year results of the ASR XL acetabular system and the ASR hip resurfacing system: An analysis from the Australian orthopaedic association national joint replacement registry. J Bone Joint Surg Am. 2011;93:2287–93. doi: 10.2106/JBJS.J.01727. [DOI] [PubMed] [Google Scholar]
- 9.Swedish Hip Arthroplasty Register. [Last accessed on 2013, September 6]. Available from: http://www.shpr.se/en/default.aspx .
- 10.Swedish Knee Arthroplasty Register. [Last accessed on 2013, September 6]. Available from: http://www.knee.nko.se/english/online/thePages/contact.php .
- 11.England/Wales National Joint Registry. [Last accessed on 2013, September 6]. Available from: http://www.njrcentre.org.uk .
- 12.US Department of Health and Human Services, Centre for Disease Control and Prevention, National Centre for Health Statistics. [Last accessed on 2013, September 6]. No authors listed. Available from: http://www.aaos.org/research/stats/patientstats.asp .
- 13.Finnish Arthroplasty Register. [Last accessed on 2013, September 6]. Available from: http://www.nam.fi/english/medical_devices/index.html .
- 14.Canadian Joint Replacement Register. [Last accessed on 2013 June 9]. Available from: http://www.cihi.ca/CIHI-ext-portal/internet/EN/TabbedContent/types+of+care/specialized+services/joint+replacements/cihi021359 .
- 15.Robertsson O. Knee arthroplasty registers. J Bone Joint Surg Br. 2007;89:1–4. doi: 10.1302/0301-620X.89B1.18327. [DOI] [PubMed] [Google Scholar]
- 16.Lubega N, Mkandawire NC, Sibande GC, Norrish AR, Harrison WJ. Joint replacement in Malawi: Establishment of a national joint registry. J Bone Joint Surg Br. 2009;91:341–3. doi: 10.1302/0301-620X.91B3.21706. [DOI] [PubMed] [Google Scholar]
- 17.Horan FT. Joint registries. J Bone Joint Surg Br. 2010;92:749–50. doi: 10.1302/0301-620X.92B6.24549. [DOI] [PubMed] [Google Scholar]
- 18.Capozzi JD, Rhodes R. Examining the ethical implications of an orthopaedic joint registry. J Bone Joint Surg Am. 2010;92:1330–3. doi: 10.2106/JBJS.I.01410. [DOI] [PubMed] [Google Scholar]
- 19.Herberts P, Malchau H. Long term registration has improved the quality of hip replacement: A review of the Swedish THR Register comparing 160,000 cases. Acta Orthop Scand. 2000;71:111–21. doi: 10.1080/000164700317413067. [DOI] [PubMed] [Google Scholar]
- 20.Herberts P, Malchau H. How outcome studies have changed total hip arthroplasty practices in Sweden. Clin Orthop Relat Res. 1997;344:44–60. [PubMed] [Google Scholar]
- 21.American Academy of Orthopaedic Surgeons. American Joint Replacement Registry project. [Last accessed on 2013 June 9]. Available from: http://www.aaos.org/registry .